
Abstract
We are celebrating the 10th anniversary of robot-assisted laparoscopic radical cystectomy (RARC) with urinary diversion (UD), and it seems that this operation is successfully following the footsteps of robot-assisted laparoscopic radical prostatectomy. Until now, approximately 1000 RARCs have been recorded; of them, only 102 were performed totally intracorporeally with a formation of an ileal neobladder. Despite the small numbers, morbidity and functional outcomes seem to be acceptable, when compared with the gold standard—the open procedure. It is imperative that in a challenging procedure such as this, the console surgeon follow a standardized protocol of all surgical steps to ensure the optimal results. In this article, we are sharing Karolinska's experience and discuss all perioperative issues along with ways of dealing with tricky cases.
Methods
Indications and contraindications
The inclusion criteria for robot-assisted formation of an orthotopic ileal neobladder are the same as in open surgery. All major contraindications for laparoscopic surgery (pulmonary insufficiency, multiple abdominal adhesions, bulky disease) are applied in robotic surgery as well.
The absolute contraindications for neobladder formation are: • Disease infiltration of the urethra distal to the prostate • Impaired renal (serum creatinine >2 mg/dL) and hepatic function • Decreased mental capability and hand dexterity
The relative contraindications are: • Inflammatory bowel disease (Crohn disease) • Impotent external sphincter, urinary incontinence • History of recurrent urethral strictures • Previous abdominal or pelvic irradiation • Severe comorbidities, elderly patients (octogenarians) • Morbid obesity
Preoperative workup and patient preparation
Standard preoperative evaluation included chest radiography, CT of the abdomen and pelvis, basic laboratory assessments, and appropriate medical clearance. Patients with pT2 + tumor had received preoperative neoadjuvant platinum-based chemotherapy. Options for UD were discussed, and orthotopic neobladder was offered to those deemed suitable.
In patients who were scheduled for orthotopic neobladder, mechanical bowel preparation (osmotic laxative) should be used the day before surgery. A stoma site is also marked the day before surgery (in case of conversion to ileal conduit). Broad-spectrum intravenous (IV) antibiotics (third generation cephalosporine plus metronidazole) are administrated at the start of the procedure and are usually stopped on postoperative day (POD) 2. All patients receive a central venous catheter, a nasogastric tube that is removed at the end of the operation, unless there is a risk of respiratory aspiration, and a patient-controlled analgesia pump.
Instrumentation
All required instruments are depicted in Table 1.
Surgical Steps
Port placement
Six-ports are placed, starting with the camera port 5 cm above the umbilicus in the midline. The camera port is placed according to the Hasson technique, while the other ports are placed in direct view. During the port placement, a pressure of 18 mm Hg may facilitate trocar placement by creating additional tension to the abdominal wall. Two robotic ports are placed symmetrically in the level of the umbilicus on the left and right side, lateral to the rectus sheath. A hybrid third robotic port is placed just above and medial to the left anterior superior iliac spine through a 15-mm standard laparoscopic port, thereby enabling laparoscopic stapling by the assistant when the third robotic port is temporarily disconnected. Two assistant 12-mm ports are placed on either side of the right robotic instrument port (Fig. 1).
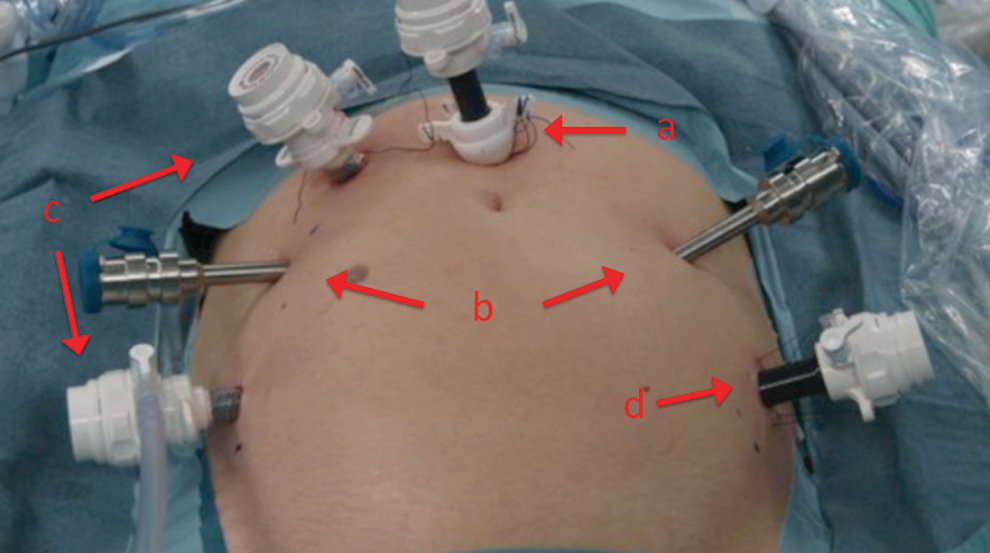
Trocar configuration for the standard da Vinci system:
It is always important to make sure that the fourth-arm port and the left robotic arm port are not in the same alignment to avoid clashing of the robotic arms.
Because this article is focused in the ileal neobladder, we will describe meticulously the surgical steps that are related to this specific part of the operation. The previous steps, such as ureteral dissection, posterior dissection of the seminal vesicles and the vasa deferentia, the cystoprostatectomy for males, or anterior exenteration for females have been described previously. 1,2
Enterourethral anastomosis
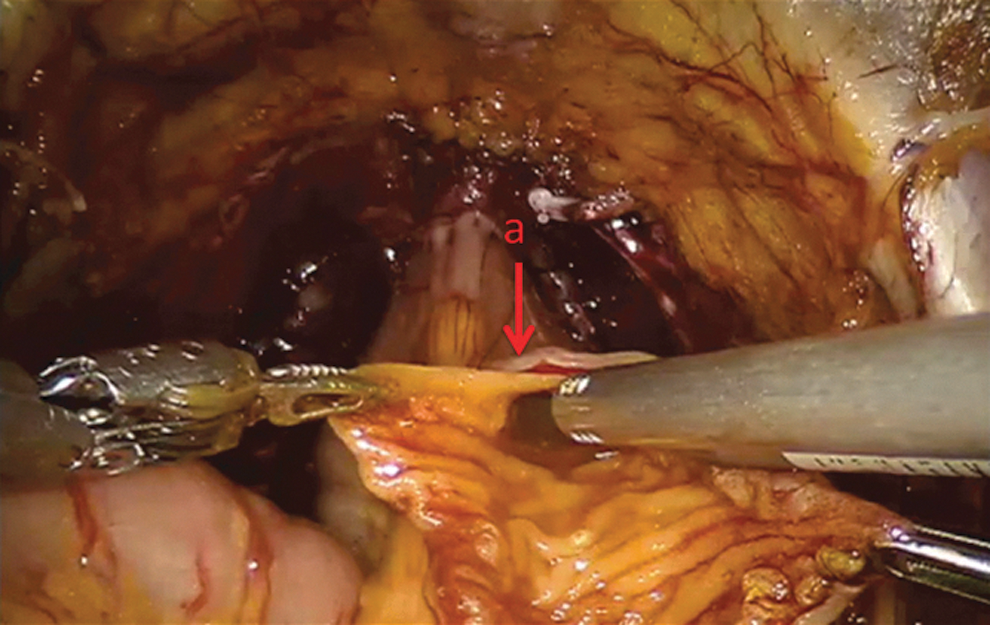
For this step, we reduce the Trendelenburg position to 10 degrees to 15 degrees. The 0-degree lens is used. The ileum is sufficiently mobilized to be positioned in the urethral proximity. Using robotic scissors, a 20F opening (Fig. 2) is created to the antimesentric site of the ileum. The specific site of incision will be selected to the site that is sufficiently placed close to the urethra. The anastomosis is performed according to the Van Velthoven technique with a two-time 16-cm running 4-0 Quill™ suture, allowing for 10 to 12 stitches (Fig. 3). A needle driver and a Cadiere forceps are used for this step.
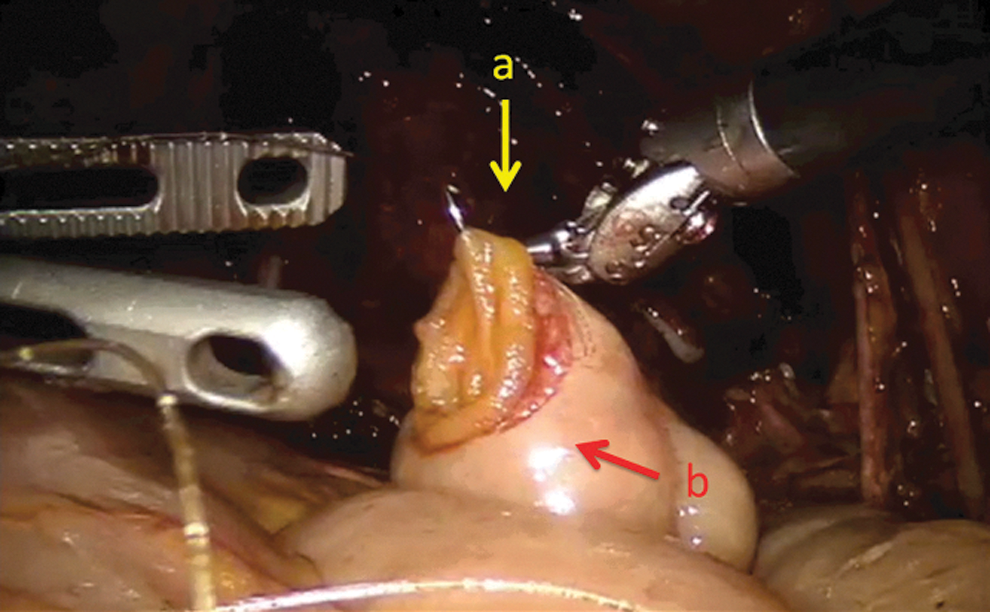
A 20F opening
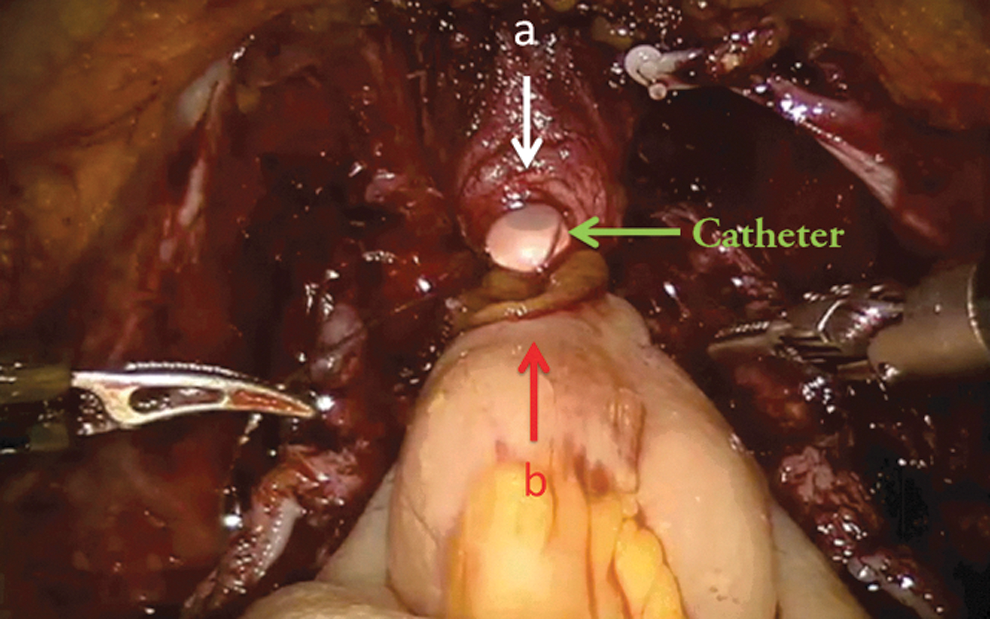
Anastomosis between urethra
It is important before the above maneuver to preserve an adequate urethral stump and have a silicone catheter placed. In cases when the ileal mesentery is applying tension, the surgeon can perform the following: • Pass two Ligaloop strings (Braun-Dexon, Spangenberg, Germany) around the intestine to stretch the ileal segment and bring it into position. • Dissect and release the covering peritoneum of the mesentery. • Staple the mesentery further medially. • Dissect the part of the ileum around the ileocecal valve.
Isolation of 50 cm of ileum
The Studer technique is used for the formation of the neobladder, which will be fashioned with a 50-cm segment of ileum. The intestine is isolated using a laparoscopic 60-mm intestinal stapler (Endo-GIA; Covidien Corp, Dublin, Ireland) (Fig. 4). The stapler is inserted by the bedside surgeon, using the hybrid 15-mm port. First, the descending segment is created by stapling approximately 10 cm away from the urethroileal anastomosis. The ascending segment then is stapled 40 cm proximal to the urethroileal anastomosis. The continuity of the small bowel is restored by using the same stapler and performing a side-to-side anastomosis with the antimesentery parts facing each other. An additional transverse firing of the Endo-GIA stapler is used to secure the open ends of the ileal limbs.
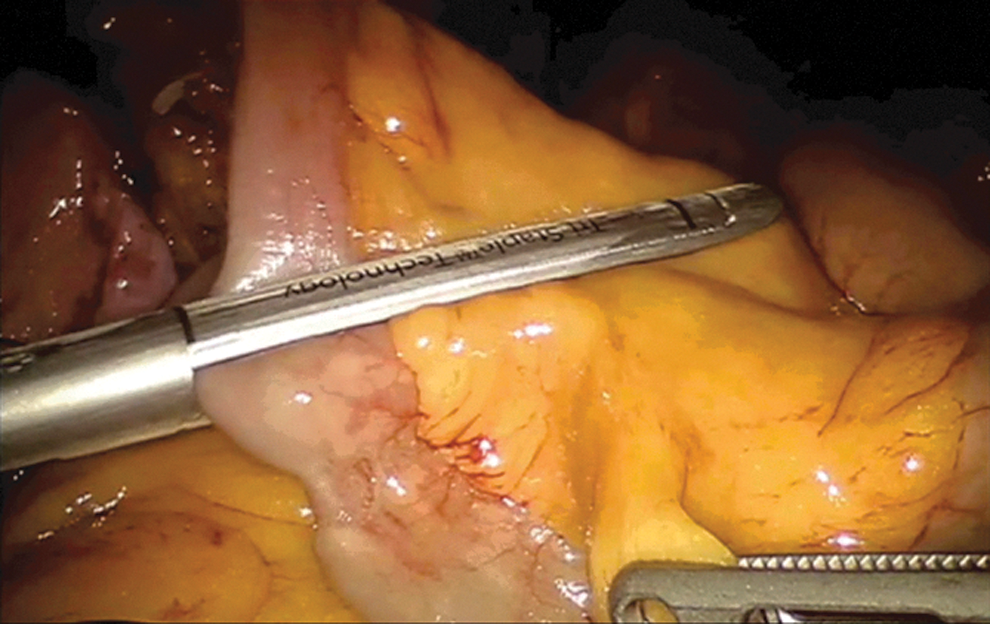
Stapling of ileum.
The ileal loop is usually contracted during the operation; thus, there is a risk of constructing a low-volume neobladder if we staple shorter segments. It is probably better to staple 4 to 5 cm more than usual for safety. An easy way to measure the ileal segments is by using the stapler's ruler.
Detubularization
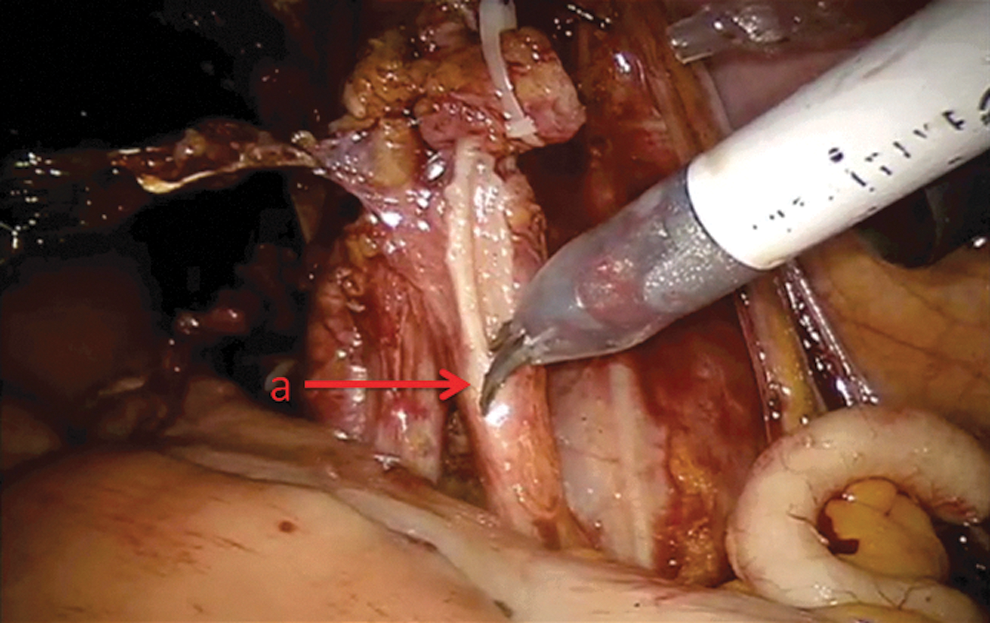
The distal 40 cm of the isolated ileal segment are detubularized along the antimesenteric border with cold scissors (Fig. 5). A 10-cm intact proximal isoperistaltic afferent limb is preserved for the ureteral anastomosis.
Detubularization of ileum, antimesenterically
Formation of Studer neobladder
The posterior part of the Studer pouch is sutured using multiple running sutures (15 cm 3-0 V-Loc™) in a seromuscular fashion, without suturing the mucosa. Once the posterior part is completed, the distal half of the anterior part of the reservoir is sutured, using the same suture. The 0-degree or 30-degree lens can be useful for this part of the procedure. The proximal half of the anterior part of the reservoir is left open and is closed during the last part of the operation.
In this step, it is probably better to start suturing the posterior wall from above and not from the urethral side, because in the latter fashion, there is a possibility of having an uneven Studer pouch, which will be difficult to compensate.
Ureteroileal anastomosis
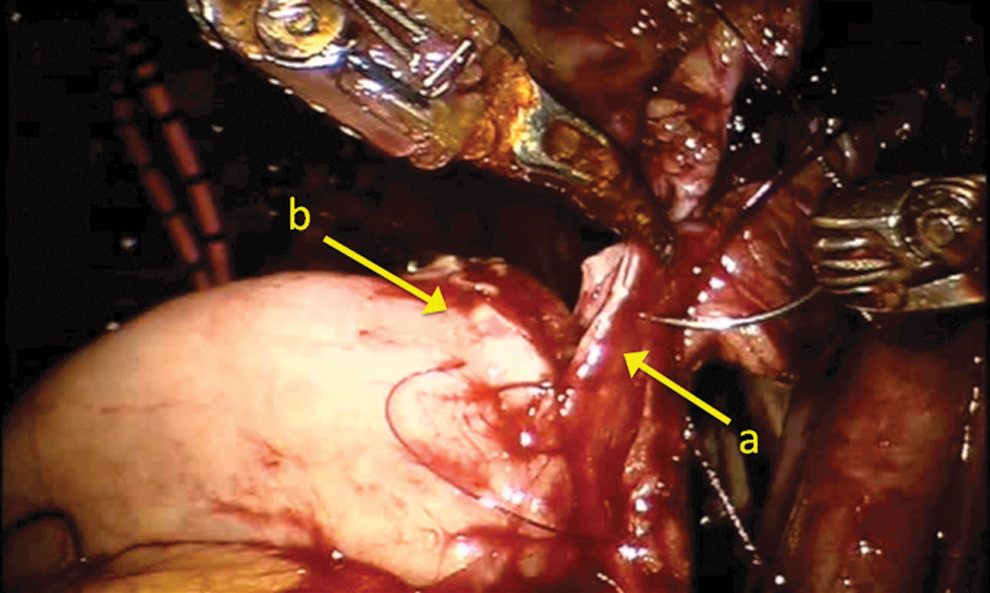
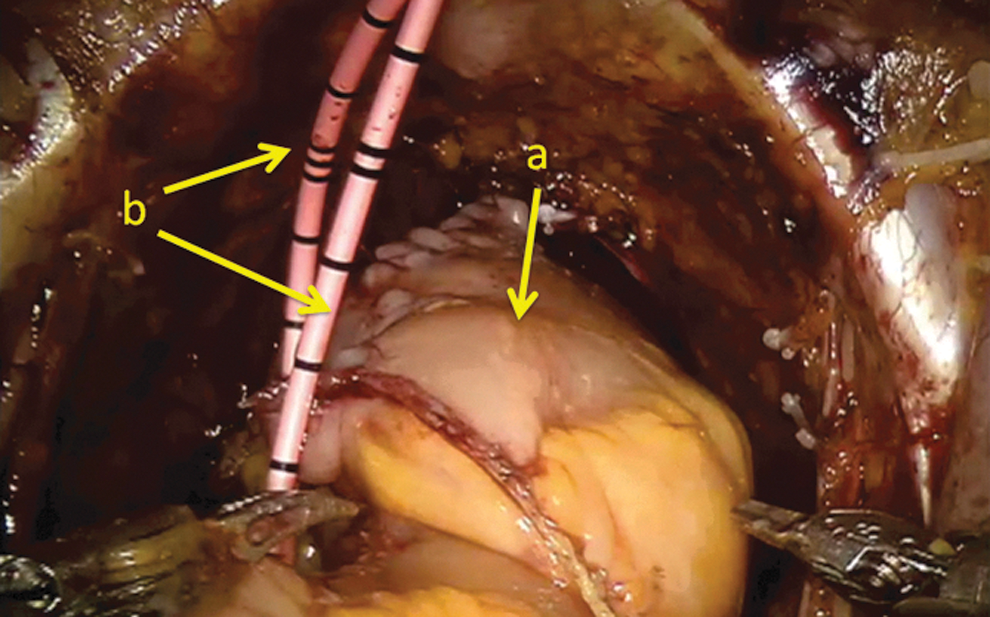
A Wallace ureteral plate is created using the 0-degree lens. A 3-0 Biosyn stitch is placed at the distal end of each ureter. The left ureter is transposed to the right by tunneling the sigmoid mesentery, just below the level of the inferior mesenteric artery. The ureters are then spatulated 2 cm (Fig. 6). The posterior walls of the ureters are sutured side to side, using a 15-cm 4-0 V-Loc suture. Before starting the anastomosis, two single-J 40-cm ureteral stents are introduced using guidewires through two separate 4-mm incisions in the midline just above the pubic symphysis. Using the Cadiere forceps, the stents are pulled through the afferent limb (Fig. 7) and pushed up into the ureters (Fig. 8). The ureteroileal anastomosis is executed using a two-time 16 -cm 4-0 Quill suture (Fig. 9). Finally, the stents are sutured and fixed to the skin.
Spatulation of the right ureter
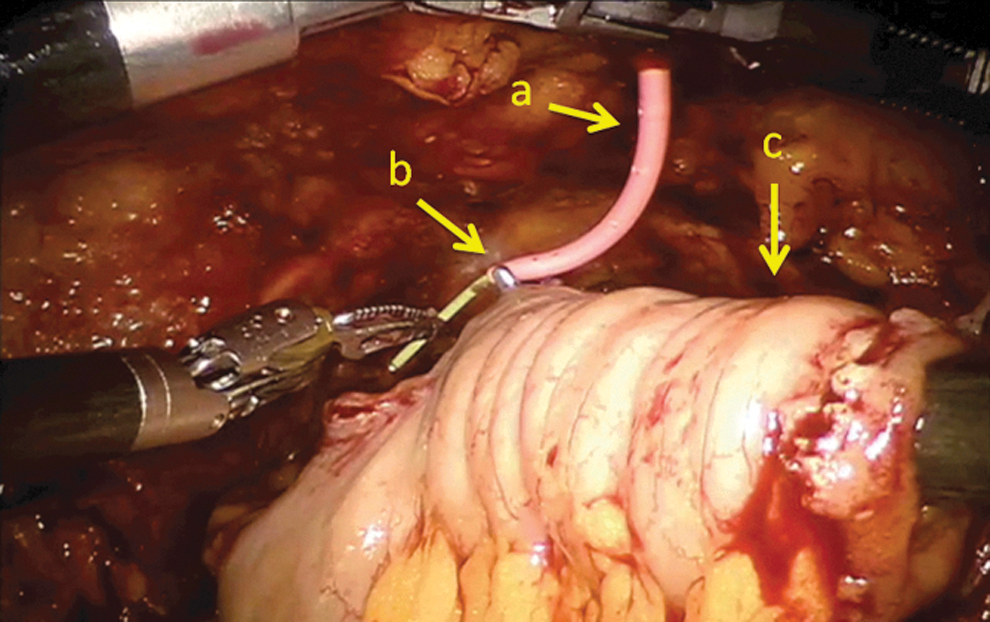
Placement of ureteral stent
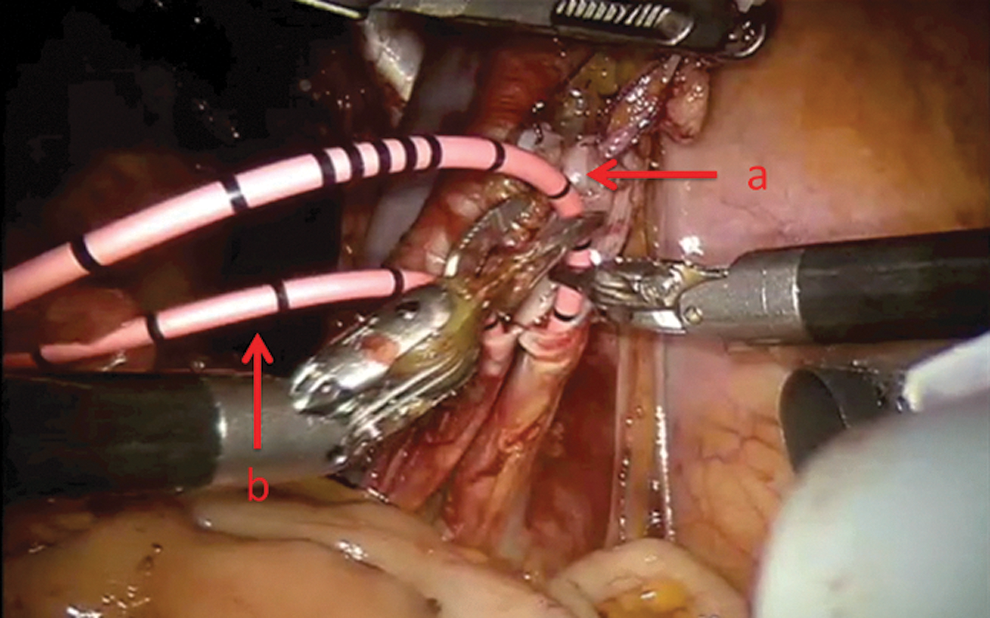
Placement of stent up through the right ureter
Anastomosis between Wallace plate
Closure of the Studer reservoir
The remaining part of the neobladder is then closed with a running 3-0 V-Loc suture, using the 0-degree lens. The balloon of the indwelling catheter is filled with 10 mL. A flush test is performed filling the neobladder with 50 cc of saline to check for leakage (Fig. 10). If leakage is observed, extra sutures will have to be considered. A 21F passive drainage is placed in the small pelvis.
After the neobladder
Postoperative care
Mobilization is strongly recommended at the day of the operation (standing at the bedside). Manual irrigation of the ileal neobladder using saline should be performed intermittently every 8 hours to remove excess mucus. The drain tube is usually removed on POD 2, if the amount of fluid is <200 mL and the creatinine levels of the drainage are not high. The ureteral stents and the urethral catheter are removed 1 and 3 to 4 weeks postoperatively, respectively. One-shot gentamycin (40 mg/mL) IV is administered 1 hour before stent removal. Pain control is achieved with oxicodone 10 mg bid, paracetamol 1 g qid, and IV or subcutaneous morphine when needed.
A dietary ladder with strict calorie intake monitoring is used from POD 1. For patients not willing to eat until POD 5, parenteral IV nutrition is administered.
All patients are meticulously informed and trained for the correct methods and frequency of urination at discharge and at regular follow-up visits.
Management of intraoperative complications
Intraoperative complications can occur, but they also can be managed successfully if recognized appropriately. First, injury to veins, especially the iliac veins, is managed with increase of the intra-abdominal pressure and use of hemostatic agents such as Tachosil® (Takeda Pharmaceuticals, Osaka, Japan) or Floseal® (Baxter, Deerfield, IL), along with application of pressure. On the contrary, injuries to arteries or bowel should be sutured with fine 4-0 or 5-0 sutures.
Leakage to any of the anastomoses should be treated with more sutures, specifically in the area of the leakage, because this will be recognized by the respective flush test.
Misfire of the Endo-GIA can occur. The main problem, though, is bleeding from the mesenteric arteries. Even though it is a sign of adequate blood circulation to the neobladder, it might create problems. Here, we recommend pinpoint coagulation using the bipolar forceps or the monopolar scissors.
Finally, the role of the assistant is crucial for a good operation. Experience is needed in pure laparoscopy and the use of several instruments. The Ligasure® should never been fired if it is close to major vessels, because the heat spillage is high and thermal damage may happen.
Management of postoperative complications
Complications after RARC with totally intracorporeal UD are not uncommon, but the majority of these complications are classified as low grade according to the Clavien classification index. 3 As it shown, the majority of these complications can be managed conservatively with some exceptions, which need surgical intervention.
Table 2 summarizes the potential early and late postoperative complications directly associated to the neobladder. 4 –7 The encountered complications are usually similar to the ones presented in an open procedure.
UTI=urinary tract infection.
Major Published Series
Until now, there have been only 102 cases published of patients undergoing minimally invasive intracorporeal formation of an ileal neobladder. 8 –15 Of them, 91 were performed robotically and 11 pure laparoscopically. Of the 91 robotic cases, 36 (40%) are contributed by Karolinska Institutet. Complication rates and perioperative characteristics of the above series are shown in Table 3.
EBL=estimated blood loss; POD=postoperative day; LAP=laparoscopic
Only two of the prementioned studies, however, were able to present functional results. Continence was defined as 0 to 1 pad use per day and potency as International Index of Erectile Function-5 score >17. Table 4 depicts the extracted data. No safe conclusions or recommendations can be drawn from the above small studies until more prospective studies with larger cohorts will be conducted.
Conclusions
RARC with formation of a totally intracorporeal orthotopic ileal neobladder is here, but is it here to stay? Even though the European Association of Urology Guidelines 2012 still consider this operation as experimental because of the lack of large prospective trials, 16 many centers are reaching the critical volume of 50 RARC per year to be considered as centers of excellence. Thus, it remains to be seen if the future results from larger, probably multicenter studies will establish the value of this extremely challenging operation. It is important for the surgeon to master and follow devoutly all the surgical steps to ensure an optimal outcome.
Footnotes
Acknowledgments
Dr. Tyritzis is a European Urological Scholarship Program 2012 scholar, funded by the European Association of Urology.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.