
Abstract
Background and Purpose:
Management of stones in the ectopic pelvic kidney can be very challenging. Treatment of each patient should be individualized. We describe a new approach that is CT-guided transgluteal percutaneous nephrolithotripsy (PCNL).
Case and Technique:
A 19-year-old male presented with symptomatic right ectopic pelvic kidney stones. He was treated with CT-guided transgluteal PCNL. The patient was stone free at postoperative day 1. No major complications were observed, and the patient was discharged home on postoperative day 2.
Conclusion:
CT-guided transgluteal PCNL is a safe and effective option for selected patients with ectopic pelvic kidney stones.
Introduction
Patients with ectopic pelvic kidneys and small burden stones can be reasonably treated by shockwave lithotripsy (SWL) or ureteroscopy, 1 –4 while for patients with a stone burden of more than 2 cm, PCNL is still the preferred option. PCNL has been mostly performed with a laparoscopy-assisted approach to mobilize the overlying intestinal segments and establish access under direct vision. 5 –8
We describe a novel approach for the management of renal stones in the ectopic pelvic kidney.
Case and Technique
A 19-year-old male presented with lower abdominal pain and gross hematuria. He had undergone open pyeloplasty at the age of 15 years for ureteropelvic junction obstruction in a right ectopic pelvic kidney. Urinalysis revealed microscopic hematuria and sterile pyuria. His serum creatinine level was 82 μmol/L. CT demonstrated three stones in the lower calices of the right pelvic kidney with total stone burden of 2 cm (Figs. 1 –3). Renal radioisotope scans evidenced 42% split function of the right kidney with excellent evacuation after standing up. Retrograde intrarenal access using an actively flexible ureteroscope was successful. Stones were not reachable after insertion of the smallest laser fiber or basket, however, because of lost degree of angulation.

Axial CT scan slide showing 1-mm stone in the right ectopic pelvic kidney with surrounding vascular structures.

Another axial CT scan showing two more stones in the same kidney measuring 6 and 4 mm with major branches of the internal iliac artery surrounding the kidney and adjacent rectum.

Sagittal reconstructed CT slide showing the kidney lying mostly in the bony pelvis with the adjacent surrounding viscera.
Options were discussed with the patient. He was offered laparoscopy-assisted PCNL or CT-guided transgluteal PCNL because the kidney was almost completely lying behind the bony pelvis. CT-guided PCNL was elected. Access was established by an interventional radiologist (Fig. 4) 1 day before the procedure. It was performed under CT guidance while the patient was in a prone position.
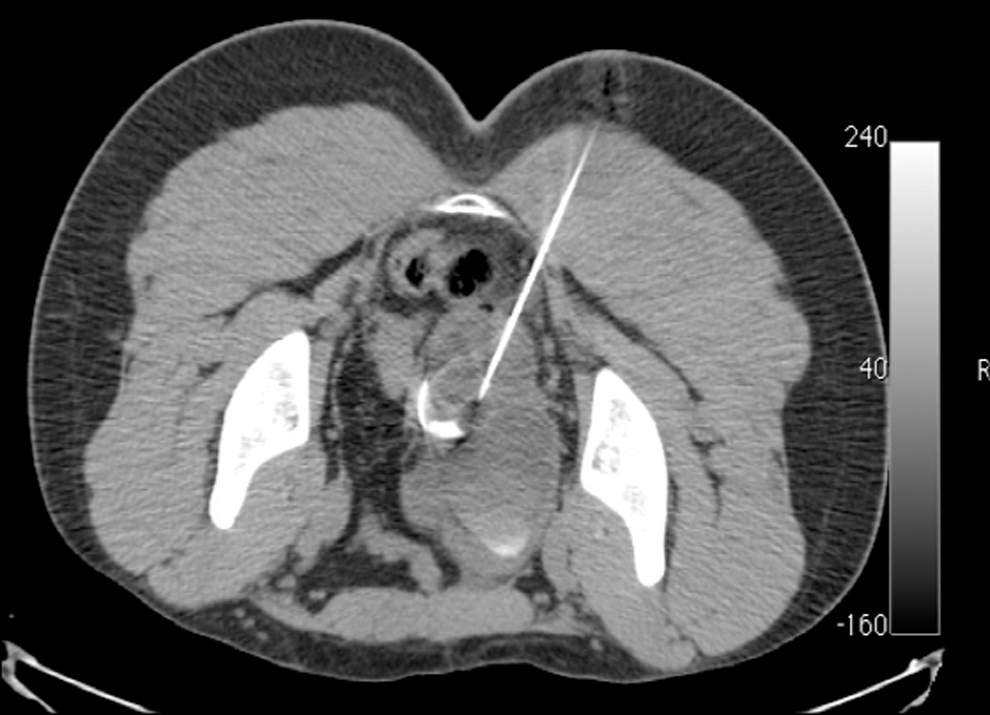
Axial CT scan showing the transgluteal access performed by the interventional radiologist under CT guidance.
To avoid injuring the sciatic nerve as well as the sacral plexus and the superior and inferior gluteal vessels, the puncturing needle must be inserted as close to the sacrum as possible, at the level of the sacrospinous ligament. With this approach, the sciatic nerve will be lying more laterally, while the sacral plexus and the gluteal vessels will be lying more cephalic. Thus, all major structures can be easily avoided. The position of the access was confirmed with antegrade injection of contrast, which filled the pelvicaliceal system of the right ectopic kidney. No immediate complications were noted.
During the procedure, the usual insertion of a 5F end-hole ureteral catheter was performed retrogradely, and then the tract was dilated using single-step dilation with

Single step balloon dilation of the tract.

The kidney after balloon dilation and insertion of a 30F sheath and two guidewires with the introduction of a flexible nephroscope into the pelvicaliceal system antegradely through the transgluteal access.

Postoperative picture showing the 22F Councill-tip nephrostomy tube inserted though the transgluteal access.
The CT scan on postoperative day 1 showed a stone-free kidney. The nephrostomy tube was removed on postoperative day 2, after which excessive leakage of urine from the access site developed. This was managed successfully by insertion of an urethral catheter. The patient was discharged home on postoperative day 2 with an indwelling urethral catheter. The patient was seen on postoperative day 4 in the clinic; he had been dry for more than 24 hours, so the urethral catheter was removed.
Discussion
Treatment of patients with pelvic kidney stones represents a great challenge to urologists. Various treatment options have been reported in the literature, ranging from SWL to laparoscopic nephrolithotomy.
Talic 1 reported on 14 patients with pelvic kidney stones who were treated by SWL. 1 Eighty-two percent of patients who presented for follow-up visits (9 of 11) were stone free at 3 months. Other reports, however, showed less encouraging results, with stone-free rates from 54% to 57%. 2,3 In our case, the stones were radiolucent, and the stone burden was large, thus precluding SWL as an option for treatment.
Retrograde intrarenal access is an alternative option, given the fast advancement of technology. Weizer and associates 4 had a stone-free rate of 75% after ureteroscopy in four patients with pelvic kidney stones. The mean stone burden was 1.4 cm. Although we managed to gain access to the stone-containing calices, the degree of angulation was lost after introducing the smallest instruments, precluding successful completion of the procedure.
The abnormal anatomic relationship between ectopic pelvic kidneys and surrounding viscera makes blind percutaneous access very risky, with high chance of injury, especially to overlying intestinal loops. Thus, most reported cases were laparoscopy-assisted PCNL. 5 –8 Laparoscopy was used to mobilize the bowel and establish transperitoneal renal access under direct vision in a retrograde or, more commonly, antegrade approach.
Laparoscopic pyelolithotomy is another option of treatment in patients with ectopic pelvic kidney stones. Chang and Dretler 9 and Harmon and colleagues 10 reported two cases with successful stone removal. Laparoscopic pyelolithotomy, however, is more appropriate for renal pelvic stones, while in patients with multiple caliceal stones, there is still a potential risk of residual stones.
We believe the laparoscopic approach might jeopardize the vascular supply to successful previous pyeloplasty. We discussed this option with our patient, explaining that risk, and it was agreed not to proceed with laparoscopy.
Direct posterior renal access under fluoroscopic guidance might be possible in certain patients. Watterson and coworkers 11 were the first to report PCNL through the greater sciatic foramen. In their patient, contrast-enhanced CT scan revealed no interposed bowel or vascular structures, and transgluteal access to the kidney was possible under direct fluoroscopic guidance.
In our patient, the scenario was different. The kidney was in close proximity to the rectum and vascular structures, as seen on contrast-enhanced CT scan. Thus, posterior access under fluoroscopic guidance was potentially risky because of the high chance of visceral or vascular injury. We adopted the CT-guided transgluteal approach as a novel alternative for treatment of our patient. The access was established by a skilled interventional radiologist through the greater sciatic foramen, which is a well-established, safe approach used by interventional radiologists to drain deep pelvic abscesses and collections. 12,13 It was first described in 1986. The main complications of this approach are pain in 20% of cases and bleeding, which is an uncommon complication.
Conclusion
Treatment options for patients with ectopic pelvic kidney stones remain individualized and range from relatively simple procedures such as SWL to more complicated approaches, including PCNL and laparoscopy.
CT-guided transgluteal PCNL represents a valid safe option in our patient. It gives the advantages of minimally invasive surgery with short convalescence and reduced postoperative pain, while minimizing the possibility of injuring the surrounding viscera and major vascular structures in comparison with direct fluoroscopy-guided access.
We believe that CT-guided transgluteal PCNL can be added to the armamentarium of management options in selected patients with ectopic pelvic kidney and stones.
Footnotes
Disclosure Statement
No competing financial interests exist.