
Abstract
Purpose:
To compare surgeon-assessed ergonomic and workload demands of magnetic anchoring and guidance system (MAGS) laparoendoscopic single-site surgery (LESS) nephrectomy with conventional LESS nephrectomy in a porcine model.
Methods:
Participants included two expert and five novice surgeons who each performed bilateral LESS nephrectomy in two nonsurvival animals using either the MAGS camera or conventional laparoscope. Task difficulty and workload demands of the surgeon and camera driver were assessed using the validated National Aeronautics and Space Administration Task Load Index (NASA-TLX) questionnaire. Surgeons were also asked to score 6 parameters on a Likert scale (range 1=low/easy to 5=high/hard): procedure-associated workload, ergonomics, technical challenge, visualization, accidental events, and instrument handling. Each step of the nephrectomy was also timed and instrument clashing was quantified.
Results:
Scores for each parameter on the Likert scale were significantly lower for MAGS-LESS nephrectomy. Mean number of internal and external clashes were significantly lower for the MAGS camera (p<0.001). Mean task times for each procedure were shorter for experts than for novices, but this was not statistically significant. NASA-TLX workload ratings by the surgeon and camera driver showed that MAGS resulted in a significantly lower workload than the conventional laparoscope during LESS nephrectomy (p<0.05).
Conclusions:
The use of the MAGS camera during LESS nephrectomy lowers the task workload for both the surgeon and camera driver when compared to conventional laparoscope use. Subjectively, it appears to also improve surgeons' impressions of ergonomics and technical challenge. Pending approval for clinical use, further evaluation in the clinical setting is warranted.
Introduction
The technical challenges of LESS can be difficult even for the experienced laparoscopic surgeon. Flexible instruments have been used to address these problems, and although they lessen the frequency of instrument collisions, they require an additional learning curve to be used properly. The robotic surgical system has also been used in an effort to overcome the limitations of LESS, with the aim of improving ergonomics, but it is also limited by significant robotic arm and instrument collision. 4 –6
Another approach in minimizing the technical limitations of LESS is reducing the number of surgical instruments at the single access port. If one or more of the surgical instruments could be removed from the single-site access platform, instrument collisions could potentially be reduced, thus improving technical ease. Magnetic technology has been studied in connection with this concept. Magnetic anchoring and guidance system (MAGS) devices, comprising magnetic instruments or camera inserted intraperitoneally through a single incision and steered via an external handheld magnet, have recently undergone preliminary experimental and clinical evaluation, 7 –9 and additional reports have highlighted excellent safety and feasibility profiles with use of these devices in the performance of complex surgical procedures. 7,8,10,11
Nevertheless, to date, studies comparing performance profiles of MAGS versus conventional instruments during urologic LESS surgery have not been reported. To this end, we evaluated surgeon performance and task workload demands during LESS nephrectomy in a porcine model performed using a MAGS camera or conventional 5-mm laparoscope. Outcomes for expert and novice surgeons were evaluated. We hypothesized that use of a MAGS camera during LESS nephrectomy would decrease workload demands by improving technical ease.
Methods
Animals and operative procedures
After obtaining approval from our institutional animal care and use committee, 14 female farm pigs (a mean of 31.5 kg) were utilized in this nonsurvival study. For the MAGS camera-assisted LESS nephrectomy, a 2.5-cm transperitoneal incision was made at the level of the umbilicus, and the MAGS camera was inserted into the peritoneal cavity through the incision. The GelPOINT® Access Platform (Applied Medical, Rancho Santa Margarita, CA) with two preplaced trocars was inserted into the abdomen alongside the MAGS camera cable, and a pneumoperitoneum was established. Two 5-mm trocars were used for the majority of the procedure, and a 12-mm trocar was substituted for one of the 5-mm trocars only during transection of the renal hilum using a conventional vascular stapler. MAGS camera-assisted LESS nephrectomy in each case was performed as previously described. 12,13 Articulating instruments (Cambridge Endo, Framingham, MA) as well as conventional rigid laparoscopic instruments were used during the procedure. The same surgical instruments and technique were utilized during conventional LESS nephrectomy, but the MAGS camera was substituted for a conventional 5-mm, 30° laparoscope, which was inserted through a third GelPOINT trocar.
MAGS camera
The latest generation MAGS camera used in this study (Ethicon Endo-Surgery, Inc., Cincinnati, OH), consists of an internally placed 1.5×7-cm tethered metallic cylinder containing the lens, light source, and permanent magnets centered along its long axis, and an external hand-held adjustable magnet (Fig. 1). The two components were coupled across the abdominal wall, allowing the camera inside to be steered to the desired positions. The imaging system consists of a quarter color CCIQ camera, with 656×492 pixels and 400 TV lines contained in an 8-mm cube (Karl Storz Endoscopy, Culver City, CA). The camera lens achieves a 30° downward field of view, mimicking that of a conventional laparoscope. Lighting is provided by an on-board LED light array surrounding the central camera lens. The tether had plug and play compatibility with an off-the-shelf camera box (StorzTelecam SL NTSC 202121-20; Karl Storz Endoscopy).The external handheld magnet, which controlled the magnetically coupled camera, weighed 634 g and measured 82 mm (length)×80.5 mm (height)×50 mm (width).
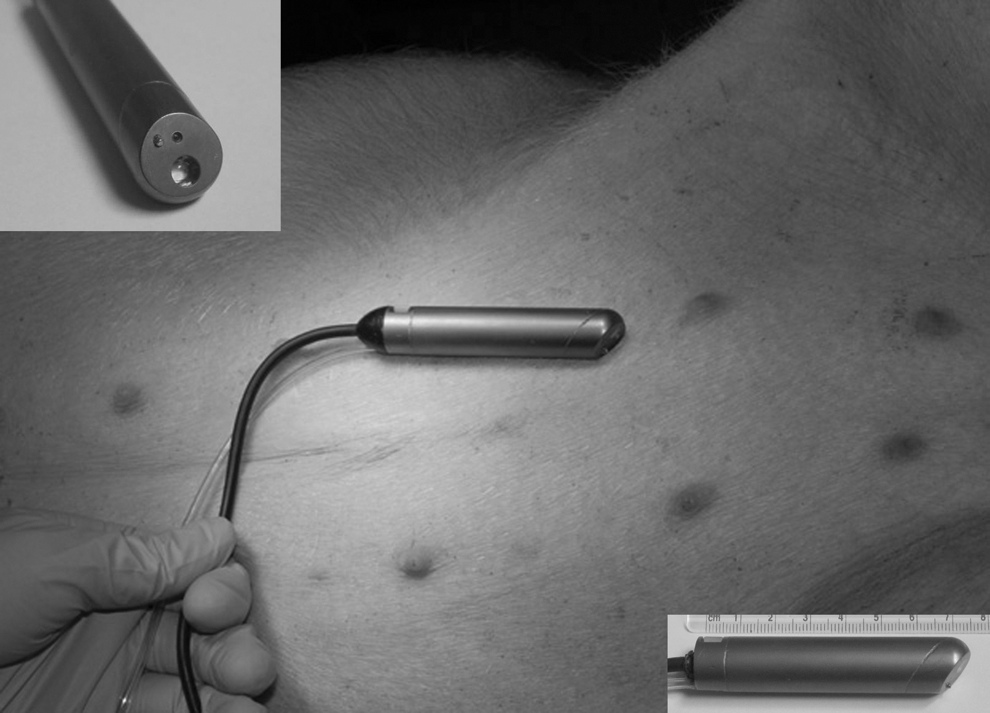
The intracorporeal magnetic anchoring and guidance system camera.
Study participants
A total of seven surgeons participated and were categorized as experts (n=2) or novices (n=5) groups according to the degree of experience with LESS. The surgeons in the expert group each had clinical experience with more than 50 LESS cases, while those in the novice group had no LESS experience. All participants were given a standardized introduction to the MAGS camera and to the LESS nephrectomy procedure. Each participant performed four nephrectomies (two conventional LESS and two MAGS camera-assisted LESS) as surgeons. They subsequently also participated as camera driver for an equivalent number of procedures.
Data acquisition
After each procedure, the participant completed a Surgeon Assessment data sheet rating six parameters (workload, ease of dissection, ergonomics, technical challenge, accidental events, and visualization) on a five-point Likert scale (Appendix A). In addition, surgeons and camera drivers each completed the previously validated six-item National Aeronautics and Space Administration Task Load Index (NASA-TLX) questionnaire, which objectively quantifies the workload imposed during task completion (Appendix B). 14 Time performance metrics were measured for each step of the procedure (Table 1), and collisions were counted by an observer and confirmed by the camera driver and surgeon.
Average scores on a five-point Likert scale as rated by surgeons after performing each surgery.
W=workload; ED=ease of dissection; Erg=ergonomics; TC=technical challenge; AE=accidental event; Vis=visualization; MAGS=magnetic anchoring and guidance system; LESS=laparoendoscopic single-site surgery.
p<0.05.
Statistical analysis
Measured outcomes were compared for MAGS-LESS versus conventional LESS and also for expert versus novice surgeon groups using the Mann–Whitney rank sum test. A two-sided p-value <0.05 was considered statistically significant in each case. All data analyses were processed with SPSS® software, version 12.0 (SPSS, Inc., Chicago, IL).
Results
Median ratings for five of six components of the Surgeon Assessment questionnaire were significantly different for MAGS-LESS compared to conventional LESS (Fig. 2). Specifically, median scores were significantly lower for MAGS-LESS for workload (p=0.02), ergonomics (p<0.001), ease of dissection (p=0.001), technical challenge (p=0.001), and accidental events (p=0.012) (Fig. 2). When comparing experts and novices, median ratings for ergonomics (p=0.019) and technical challenge (p=0.011) were rated significantly lower for MAGS-LESS by experts, whereas ease of dissection (p=0.005), ergonomics (p=0.002), technical challenge (p=0.014), and accidental events (p=0.007) were rated significantly lower for MAGS-LESS by the novice group (Table 1). Mean number of internal and external instrument clashes, was significantly lower during MAGS camera-assisted LESS nephrectomy as compared with conventional LESS nephrectomy (Fig. 3). The NASA-TLX assessed overall workload for the surgeon and the camera driver was lower for MAGS-LESS (Fig. 4). For surgeons, the differences for each subscale score except performance were statistically significant, while for camera drivers, differences for each subscale score except performance and effort were statistically significant. Within the expert group, statistically significant advantages for the MAGS camera were reported for physical demand (p=0.019) and frustration (p=0.017), whereas for the novice group, significant advantages in mental demand (p=0.034), physical demand (p=0.04), effort (p=0.043), and frustration (p=0.037) were reported for the MAGS camera (Table 2).
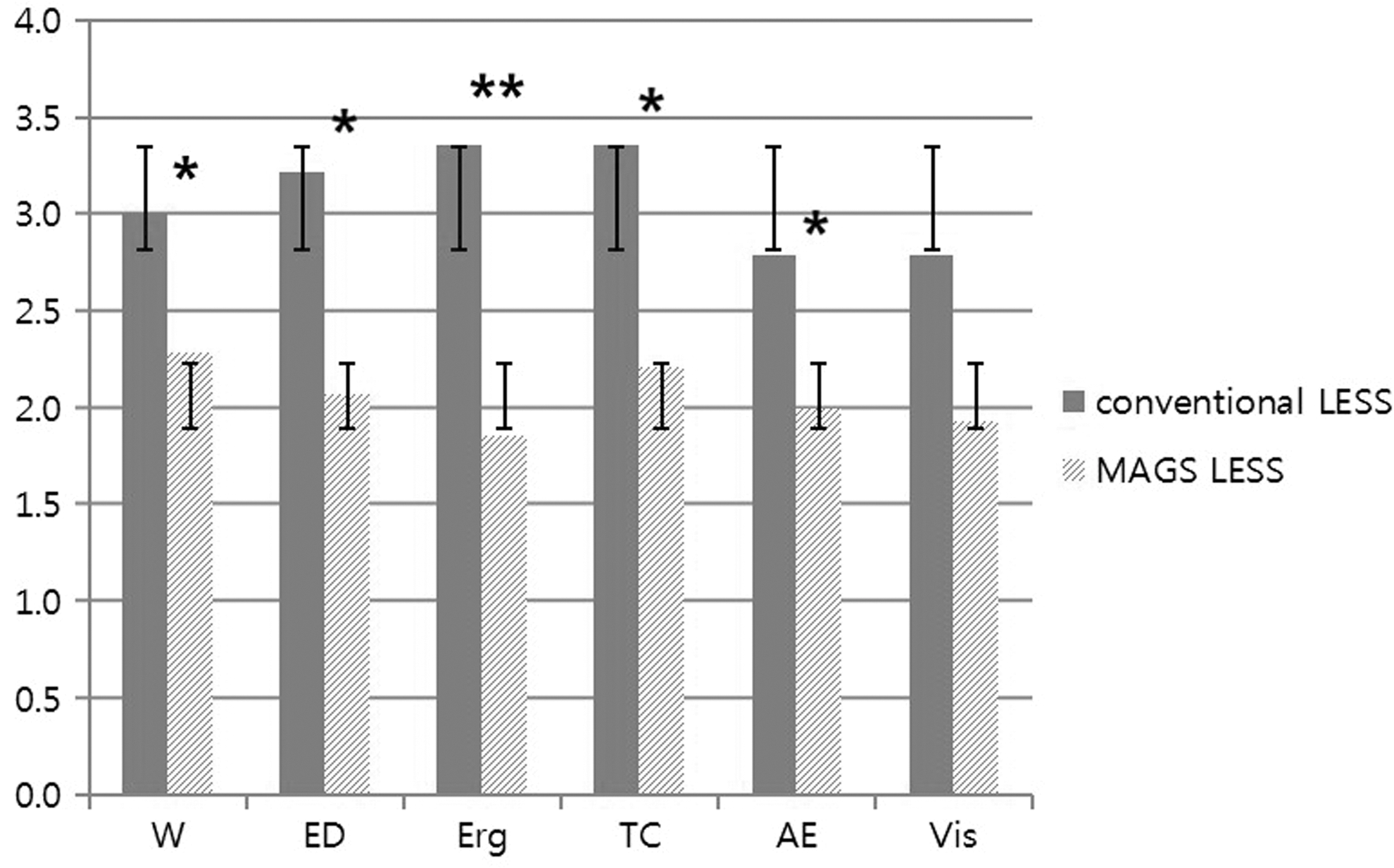
Surgeon assessment measures: average scores on a five-point Likert scale as rated by surgeons after performing each surgery. W, workload; ED, ease of dissection; Erg, ergonomics; TC, technical challenge; AE, accidental event; Vis, visualization. *p<0.05; **p<0.001.
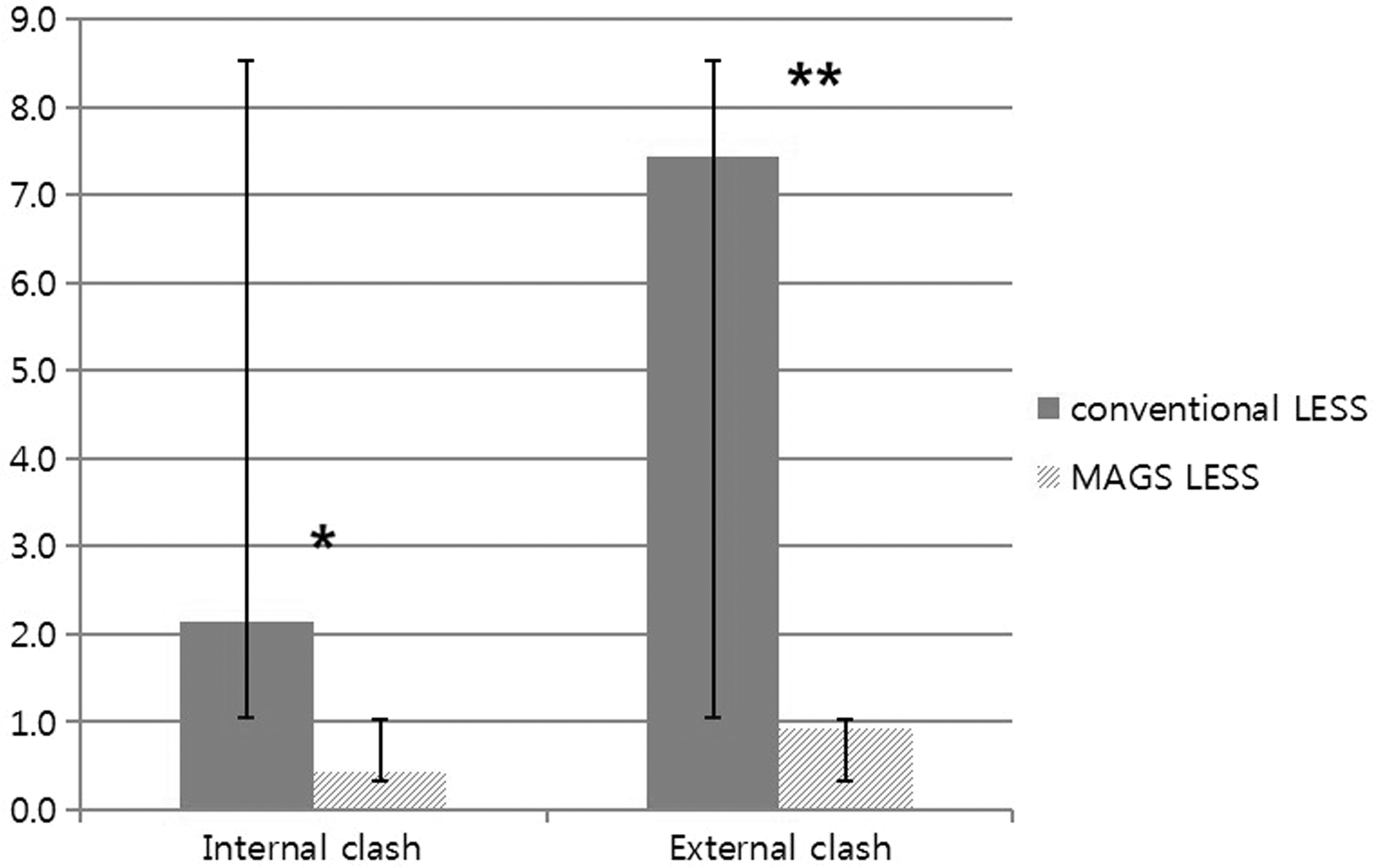
The mean number of instrument clashes. *p<0.05; **p<0.005.

The overall workload of surgeon and camera driver (unweighted sums of NASA-TLX scores). *p<0.05; **p<0.005.
MD=mental demand; PD=physical demand; TD=temporal demand; Per=performance; Eff=effort; Frus=frustration; TLX=task load index questionnaire.
p<0.05.
For conventional LESS, the total procedure time was significantly shorter for the expert group compared with the novice group (p=0.048). For the novice group, MAGS-LESS vs. conventional LESS total procedure time did not significantly differ (36.4 vs. 33.0 minutes, p=0.45). For the expert group, procedure times by approach were also similar (22.0 vs. 23.1 minute, p=0.248). However, time to hilar transection for the expert group was significantly shorter than for novices during both conventional LESS and MAGS-LESS (Table 3). Although surgeons in the expert group performed better than those in the novice group in terms of the time to completion of both surgeries, there were no overall within group differences for MAGS-LESS vs. conventional LESS task-specific times (Table 3).
p<0.05.
Discussion
Since the introduction of video-assisted endoscopic surgery has revolutionized modern day surgery, minimally invasive surgery has become widespread in most of the surgical specialties. 15,16
To date, LESS techniques have been applied to various urologic surgeries in which conventional laparoscopic surgery is indicated. 1 –3,17 However, most reports have focused on feasibility and safety, and are limited to patients with a low body mass index. This is largely because LESS procedures are limited by unfavorable ergonomics, resulting in significant technical difficulty. 17 To solve the problems of instrument collision, loss of triangulation, and unfamiliar working views, several techniques, including use of articulating instruments and adaptation of robotics, have been reported. 7 –9 A separate approach involves use of MAGS instruments, as previously reported by our group. 7 –11 In the present study, we evaluated the impact of MAGS camera use during LESS nephrectomy on the surgical workload, ergonomics, and surgeon performance. Furthermore, by comparing outcomes for expert and novice surgeons, we assessed whether MAGS camera use facilitated adoption and performance of LESS by novice surgeons.
In the nonvalidated Surgeon Assessment questionnaire, which employed a Likert scale to evaluate surgeons' impressions of task difficulty, overall surgeons' assessment in the domains of workload, ergonomics, ease of dissection, and technical challenge favored the MAGS camera over a conventional laparoscope. Furthermore, the magnitude of the differences in the observed ratings suggests that clinically significant differences likely exist. Ergonomics and technical challenges were found by experts and novices alike to be more favorable for the MAGS camera, while novices additionally scored ease of dissection in favor of the MAGS camera. These findings suggest that decoupling the camera from the umbilical portal during LESS raises subjective impressions of improved ergonomics and technical challenge by expert and novice surgeons alike.
The NASA-TLX is a validated multidimensional subjective rating assessment that derives an overall task workload score from a rating on six subscales. 14 This provides a validated means by which the surgeon and/or the assistant workload can be quantified, allowing for comparative assessment. We analyzed the unweighted NASA-TLX because high correlations have been shown between the weighted and unweighted scores. 18 In this study, the surgeon and camera driver overall workload during MAGS-LESS nephrectomy was found to be significantly lower than during conventional LESS. Workload ratings for experts during MAGS versus conventional LESS did not differ from those for novices. Similar findings were reported by Arain et al 19 during bench top, ex vivo testing comparing a conventional laparoscope (LAP), flexible endoscopic camera (ENDO), and a MAGS camera. Surgeon workload was found to be significantly less for MAGS compared with ENDO, while camera driver workload was significantly less for MAGS compared with LAP or ENDO. 19 A decreased surgeon workload may be viewed as a surrogate measure for improved overall ergonomics. The combined findings of these studies suggest that use of the MAGS camera during LESS significantly improves task ergonomics, most likely due to decreased instrument collisions. Indeed, we observed significantly fewer internal and external instrument collisions during MAGS-LESS nephrectomy (Fig. 3). Further investigation in the clinical setting is certainly warranted.
Lastly, we found that mean overall setup time during MAGS-LESS nephrectomy, which included time for intracorporeal deployment of the MAGS camera, was not significantly different than for conventional LESS nephrectomy. Interestingly, the mean total procedure time for the operations was also similar (32.3 vs. 30.1 minute, p=0.75), despite improved ergonomics during MAGS-LESS. This could certainly reflect an impact of the learning curve for this novel LESS platform.
Because this technology works through the maintenance of attraction between 2 magnets separated by the abdominal wall, investigators were concerned about tissue damage resulting from the effect of compression over time. However, recent investigations have demonstrated that the MAGS camera does not cause tissue damage of the abdominal wall and that the strength of the magnetic camera is likely sufficient to span the distance of most human abdominal walls. 20,21
Our study had a few limitations worth discussing. First, there was a low number of experts. However, each surgeon performed a total of four procedures allowing for a reasonable number of repeated measures for meaningful comparison. Although a validated scale, the NASA-TLX is a generalized questionnaire, which is not specifically tailored for assessment of surgery-related tasks. Accordingly, we also used a customized Likert scale to evaluate surgeons' impressions of procedure ergonomics.
Conclusion
MAGS camera-assisted LESS nephrectomy was confirmed to be a feasible and safe procedure in the porcine model. The MAGS camera decreased the NASA-TLX assessed workload of surgeons and camera drivers compared with a conventional laparoscopic camera during LESS nephrectomy, reflecting a better ergonomic profile with the MAGS camera. Subjectively, it appears to also improve surgeons' impressions of ergonomics, visualization, and technical challenge. Further evaluation in the clinical setting is warranted.
Footnotes
Disclosure Statement
Jeffrey A. Cadeddu and Daniel J. Scott are consultants and investigators for Ethicon Endosurgery.
Appendices
Surgeon Assessment Questionaire (5-point Likert scale)
| Workload: | (low/easy) | 1 | 2 | 3 | 4 | 5 | (high/hard) |
| Ease of dissection: | (easy) | 1 | 2 | 3 | 4 | 5 | (hard) |
| Ergonomics: | (comfort) | 1 | 2 | 3 | 4 | 5 | (discomfort) |
| Technical challenges: | (low) | 1 | 2 | 3 | 4 | 5 | (high) |
| Accidental Event: | (low) | 1 | 2 | 3 | 4 | 5 | (high) |
| Visualization: | (good) | 1 | 2 | 3 | 4 | 5 | (bad) |