
Abstract
Background and Purpose:
Inguinofemoral lymphadenectomy (IFLA) is a standard procedure for cancer of the external genitalia. Open lymphadenectomy (O-IFLA) exhibits complication rates of more than 50%. We are demonstrating our extended experience with a modified endoscopic approach (E-IFLA) for groin lymphadenectomy.
Patients and Methods:
Patients with nonpalpable as well as those with palpable nodes who had IFLA were identified. O-IFLA comprised both superficial and deep inguinal lymph node dissection. E-IFLA was performed using a three-trocar approach in the same field. We used a reduced CO2-pressure of <5 mm Hg. A suction drain was always placed. Perioperative data and postoperative outcomes were systematically assessed followed by statistical analysis.
Results:
We performed 62 IFLAs in 42 patients. Twenty-eight procedures were completed endoscopically. Follow-up was 55.8 months (2–87 mos). Mean operative time for O-IFLA was 101.7 minutes (38–195 min), being shorter than for E-IFLA (136.3 min, 87–186 min), P<0.001. Both groups are comparable regarding the number of nodes (O-IFLA 7.2, 2–16 vs E-IFLA 7.1, 4–13) as well as with regard to the number of positive nodes (O-IFLA 1.8 vs E-IFLA 1.6). Secondary wound healing and leg edema were extremely rare events (1/28) after E-IFLA. The overall complication rate was 7.1%. Complications appeared in 55.3% of the O-IFLA-cases. There were no problems related to CO2 insufflation. Local recurrence rates were identical in both groups.
Conclusions:
O-IFLA and E-IFLA are efficient with respect to oncologic safety. E-IFLA is technically more challenging. E-IFLA can avoid secondary wound healing and lymphatic complications. E-IFLA is a safe procedure while a reduction of CO2 pressures optimizes the safety profile. Because cancer control rates remained equivalent during an extended follow-up, oncologic durability could be confirmed.
Introduction
IFLA is not only believed to be diagnostic but also to be therapeutic. 6,7 The procedure is meant to reduce tumor burden while also providing coverage for the femoral vessels to ensure efficient wound healing. 8,9 Up to 60% of patients with penile cancer have enlarged nodes in their groins, and half of these are true metastasis. 1,5 IFLA plays a significant role in penile cancer, because more than 60% of patients are cured by surgery alone. 2,6,7,10
Even though IFLA is widely recognized as being necessary, it is still feared by many surgeons. Open IFLA has been reported to have complication rates of 50% to 100% even in experienced centers. 11 Hence, many surgeons as well as their patients are reluctant to actually undertake traditional IFLA even if it is beneficial. 7
Although penile malignancies are comparatively rare, there have been considerable efforts to minimize the inherent morbidity of lymphadenectomy. These include a dynamic sentinel node technique, modified superficial templates, as well as endoscopic techniques. Bishoff and associates 12 first reported endoscopic IFLA in cadavers and in a single patient. Then Sotelo and colleagues 13 and Tobias-Machado and coworkers 14 presented their results. Since then, several modifications of the technique, including robot assistance, have been described. 15,16 The main highlight of this approach is reduced skin-related morbidity. We have added to this development by using a modified low-pressure set-up. In the underlying study, we present our extended experience with endoscopic IFLA (E-IFLA) in penile cancer as well as in other genitourinary malignancies. Results are further compared with patients who underwent open IFLA (O-IFLA).
Patients and Methods
In a retrospective manner, we identified 42 patients with genitourinary maignancies who needed IFLA as part of a curative treatment regimen. In total, we completed 62 procedures. Indications included penile cancer, testis cancer (in patients post orchiopexy), melanoma, and urethral cancer. Both patients with nonpalpable and palpable nodes were included after a 6-week course of antibiotics. There were no specific contraindications except from coagulopathy and exulcerating tumors. While not an absolute contraindication, large, bulky, matted nodes were a relative contraindication assessed on an individual basis. Informed consent was given in all cases. Ethical approval was obtained before data analysis (#119/2012R). No sentinel biopsy was performed before formal lymph node dissection.
O-IFLA
A conventional IFLA was performed via an oblique inguinal incision. This technique has been highlighted elsewhere. 2,8 The anatomic boundaries were the sartorius muscle laterally, the musculus adductor longus medially, and the inguinal ligament cranially. Both superficial and deep dissection were performed without saphenous vein preservation. The sartorius muscle was rotated to provide vascular coverage. A suction drain was placed in all cases and not removed until the output was 50 mL or less.
E-IFLA
The patient was positioned supine with bilateral thigh abduction (frog-leg position) (Fig. 1). The endoscopy system was placed opposite of the surgeon. Initial access was achieved by an incision made approximately 2 cm distal to the tip of the femoral triangle (Fig. 2). Digital, blunt dissection was used to establish a plane below the Scarpa fascia. A 10-mm Hassan trocar was then inserted, and the working space was insufflated with CO2 at a maximum of 5 mm Hg to reduce CO2-associated complications. CO2 pressures were mostly kept around 2 to 3 mm Hg. The telescope was used to further develop the working space under direct vision. An additional 12-mm trocar was inserted medially and a 5-mm port was placed laterally to achieve sufficient triangulation (Fig. 3). We used a 30-degree lens in all cases.

Patient positioning in a supine frog-leg position. Both ankles are fixed using an elastic bandage.
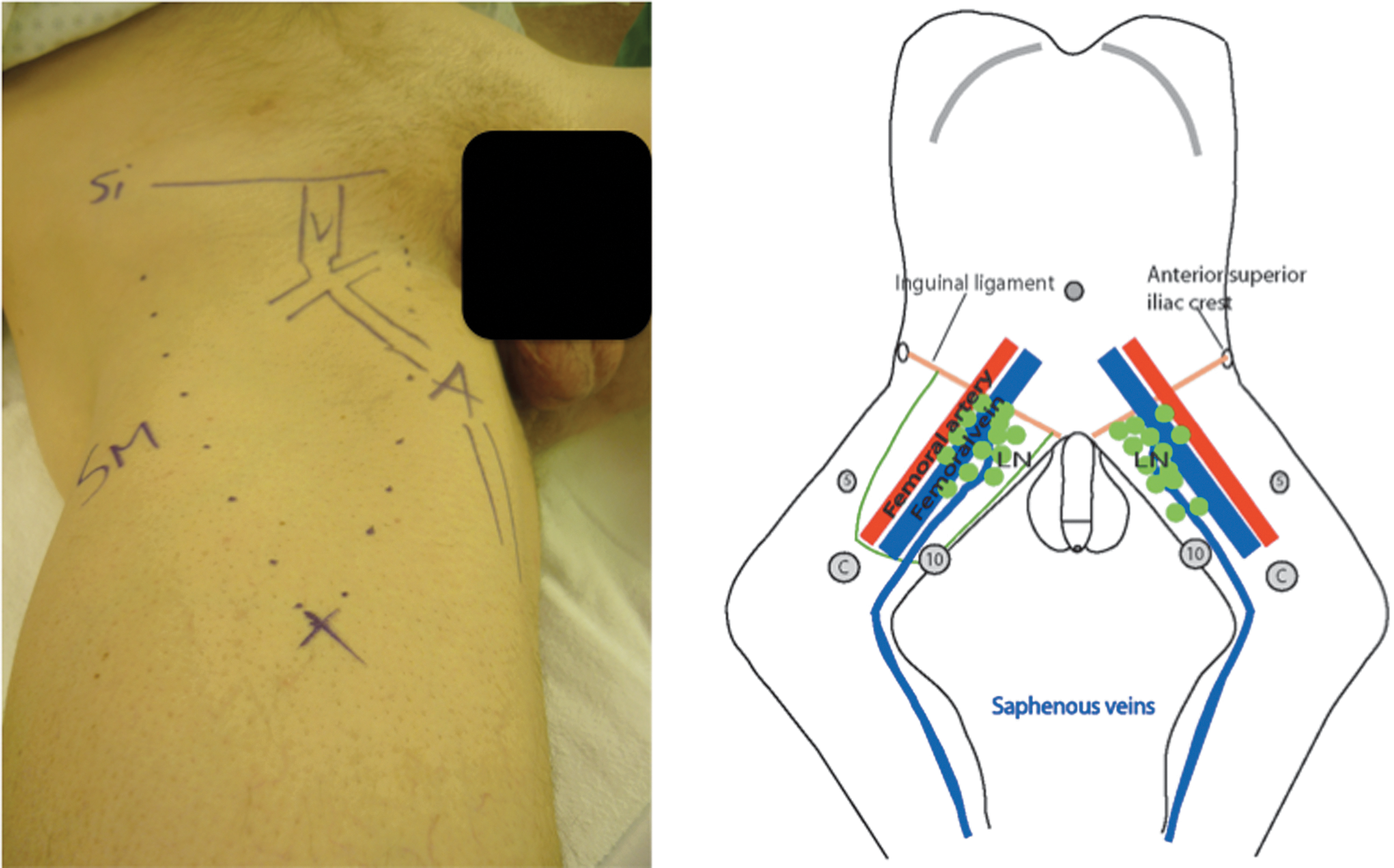
Hybrid image showing the anatomic boundaries and landmarks that are used to aid port positioning. The first port is placed 2 cm distal from the tip of the femoral triangle.
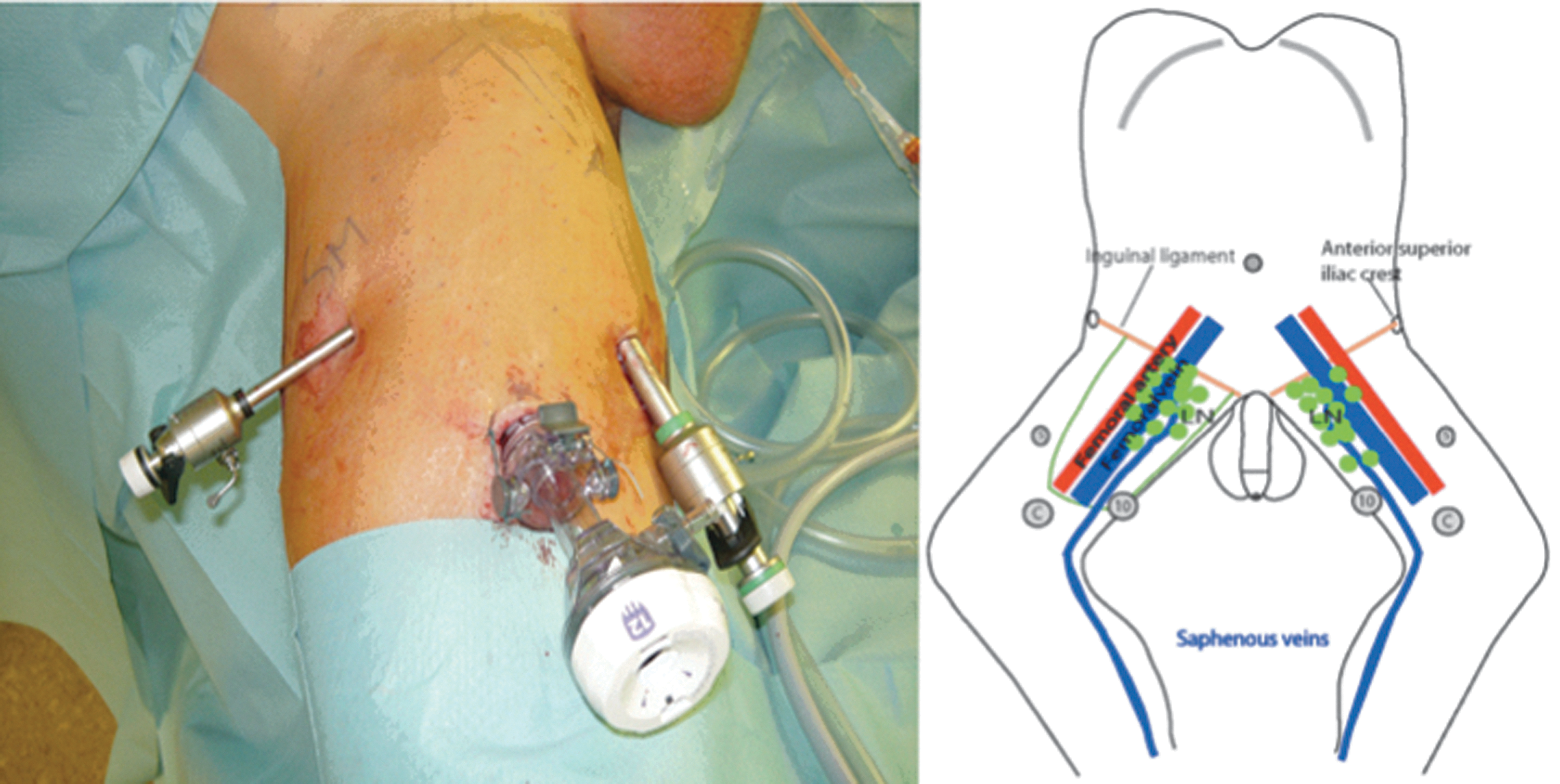
Hybrid image showing the standardized trocar position.
The 10-mm port was used for a Hem-o-lok® (Teleflex Medical, Triangle Park, NC) clip applier and the endobag. Further instruments used were conventional graspers, a bipolar forceps, scissors, and a vessel sealing device (BiCision,® ERBE Elektromedizin, Germany). The latter device ensured appropriate sealing of lymphatics and minor vessels. Transillumination was helped for easy orientation.
Initial dissection involving the superficial nodes starts right underneath the Scarpa fascia (Fig. 4). The anatomic landmarks are identical to those of O-IFLA: The sartorius muscle laterally, the inguinal ligament cranially, and the adductor longus muscle medially. Early identification of the saphenous vein and extensive dissection to the level of the fossa ovalis avoids bothersome bleeding (Fig. 5). All lymph nodes found in the course of the saphenous vein and all those in proximity to the superficial epigastric vessels were removed (Fig. 6).
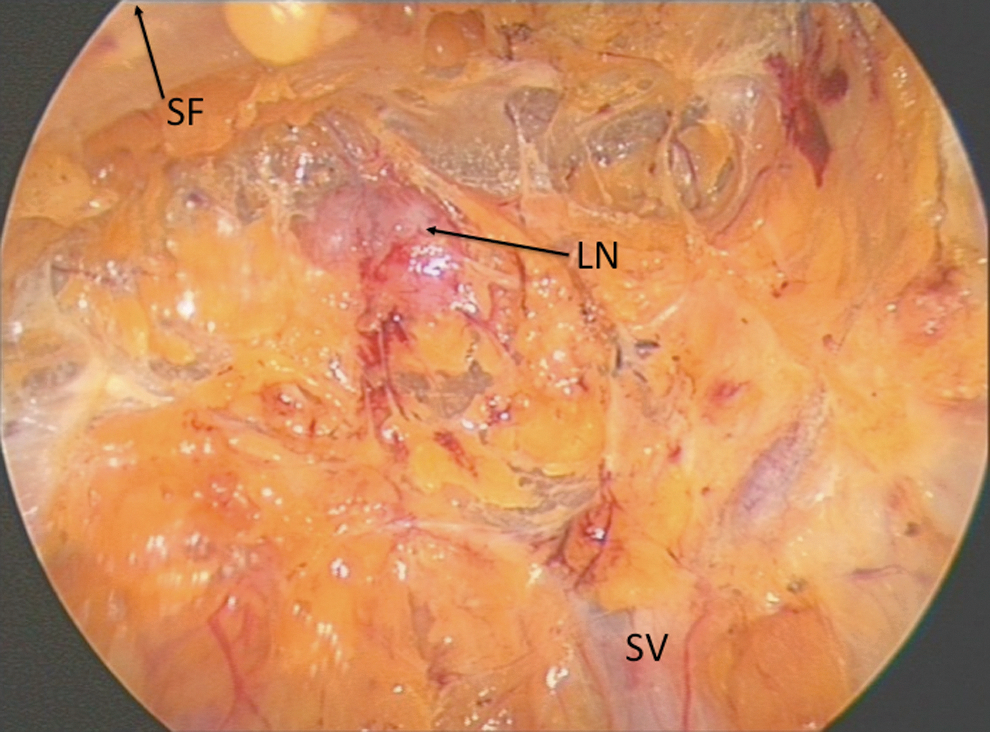
Development of a plane below the Scarpa fascia and dissection of the most superficial nodes. SF=Scarpa fascia; LN=lymph node; SV=saphenous vein.
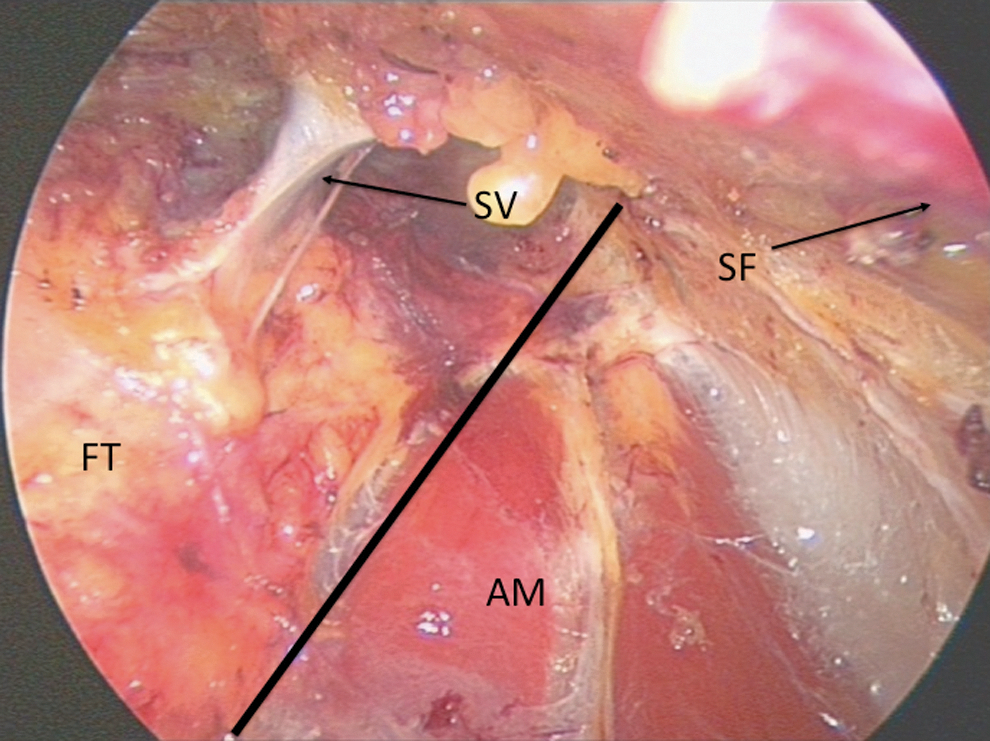
Early identification of the saphenous vein improves orientation in the surgical field. SV=saphenous vein; SF=Scarpa fascia; FT=femoral triangle; AM=adductor magnus muscle; black line marks medial edge of dissection.

The superficial veins draining into the saphenous veins are dissected free. IL=inguinal ligament; SF=Scarpa fascia; FA=femoral artery; SV=saphenous vein; FT=femoral triangle; AM=adductor magnus muscle; SM=sartorius muscle; black lines mark edges of dissection.
The vessel sealing instrument was used to transect the boundaries of the lymph node package. The femoral artery was identified by its pulsation marking the lateral edge of dissection. Lymphatic tissue dissection was then taken to the femoral vessels above the level of the femoral ring. The saphenous vein was transected distally using XL-Hem-o-lok clips (Fig. 7) The saphenous vein branches were controlled using BiCision, while the vein was proximally ligated with another pair of Hem-o-locks (Fig. 8). The fascia lata was opened, and dissection was continued medially of the femoral vein underneath the foramen ovale reaching the inguinal ligament. The node of Cloquet was identified beneath the inguinal ligament (Fig. 9).

Identification of the femoral artery and vein initiated deep dissection. IL=inguinal ligament; FV=femoral vein; FA=femoral artery; SV=saphenous vein.

The saphenous vein is transected and secured with clips. SF=Scarpa's fascia; IL=inguinal ligament; FA=femoral artery; SV=saphenous vein; AM=adductor magnus muscle; black lines mark edges of dissection.
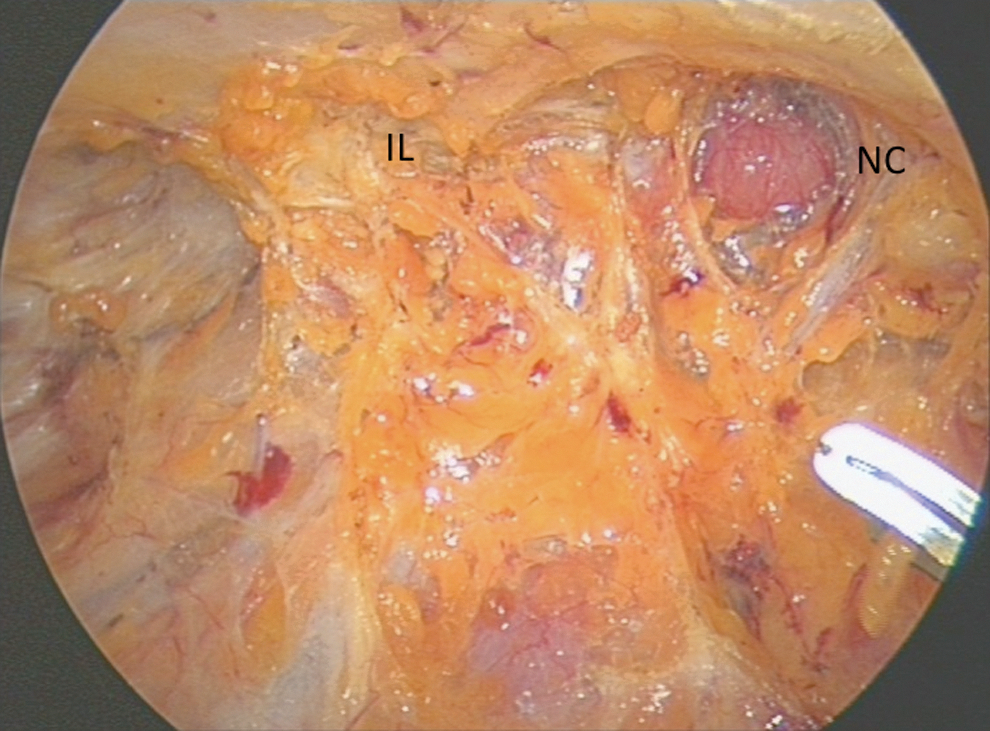
Identification of the Cloquet node marks the superior limit of dissection. IL=inguinal ligament; NC=node of Cloquet.
The specimen was fully mobilized and removed using an endobag. A suction drain was placed using the 5-mm trocar. Compression stockings were immediately placed postoperatively and left for 2 more weeks. Prophylactic intravenous cefuroxime was administered routinely. In the postoperative period, patients were mobilized early and low-molecular heparin was administered. The suction drain was removed with a production below 50 mL.
Analysis
We analyzed operative time, nodal yield, positive lymph nodes, intraoperative complications (Clavien grade), postoperative outcomes, and local recurrence. Statistical analysis for comparative parameters was performed using chi-square and Fisher exact tests. Statistical significance was assumed if P<0.05.
Results
Sixty-two IFLAs were performed in 42 patients. Indications were penile cancer in 27 patients, melanoma in 12, testis cancer in 1, sarcoma in 1, and prostate cancer in 1 patient, respectively. Overall patient age was 17 to 80 years (mean 59.95 years), while there was no difference between the groups (P=0.35). Twenty-eight procedures were completed endoscopically (mean age 62.8 years). The mean follow-up period was 55.3 months (2–87 mos). Overall operative time for O-IFLA was 101.7 minutes (38–195 min), which was shorter than for E-IFLA (136.3 minutes, 87–186 min), P<0.001. Table 1 shows patient characteristics before bilateral IFLA including grade, stage, and vascular invasion.
O-IFLA=open inguinofemoral lymphadenectomy; E-IFLA
We did not encounter intraoperative complications, and all surgeries were completed successfully. Both groups are comparable when looking at the nodal yield (O-IFLA 7.2, 2–16 vs E-IFLA 7.1, 4–13) as well as with respect to the number of positive nodes (O-IFLA 1.8 vs E-IFLA 1.6). Pathologic examination of the affected lymph confirmed their anatomic integrity. Positive nodes were found in 12 patients in the O-IFLA cohort whereas 8 patients were affected in the E-IFLA cohort. These patients subsequently underwent laparoscopic pelvic lymphadenectomy showing no additional nodal metastatses. Lymphatic complications or secondary wound healing were extremely rare events (1/28) after E-IFLA. The overall complication rate was, hence, 7.1 %. One patient had postoperative hemorrhage necessitating reendoscopy (grade III), while the other patient had bilateral lymphoceles necessitating bedside puncture (grade III). There were no problems related to CO2 insufflation.
Complications appeared in 55.8% of the O-IFLA-cases (19/34). Of those, 3had grade II and 16 had grade III complications, with the majority being related to insufficient wound healing in the groin. Lymphatic edema occurred in 15/34 (44.1%) patients. Rates of local recurrence were comparable in O-IFLA (7.7%) and E-IFLA (6.6%).
Discussion
IFLA is typically performed in patients with penile cancer but also for other malignancies of the lower extremities and the external genitalia, such as melanoma. As such, groin dissection is still considered a challenging procedure, mainly because of a considerable complication rate. This has been corroborated even in very contemporary series. 17,18
There have been efforts made to minimze the side effects and morbidity of this operation either by limiting node dissection (sentinel node-technique) or by using an endoscopic approach. Bishoff and associates 12 first described an endoscopic approach, performing it first in an experimental cadaver setting. Open conversion was necessary in their only reported patient because of bulky nodes adjacent to the femoral vessels. Tobias-Machado and colleagues 19 and Sotelo and coworkers 13 performed a study comparing unilateral endoscopic groin dissection to contralateral open surgery. 13,19 They showed comparable nodal yields but decreased complications and morbidity. Meanwhile, robot assistance has been introduced to E-IFLA demonstrating its feasibility and reproducibility. 15
There is increasing evidence to expand the role of IFLA. Naumann and colleagues 20 investigated a group of men typically eligible for surveillance (pT1 moderately differentiated penile carcinoma) who had ultimately undergone groin dissection. They found that 44% of these intermediate-risk patients had metastases. Others reported similar findings in their respective cohorts of patients. 10,21 The survival advantage of lymphadenectomy in patients with impalpable lymph has been demonstrated. The surgical morbidity, however, remains too high. 11,17,18
O-IFLA is performed via a considerable groin incision. It can hence result in skin complications such as necrosis and wound infection. If the resection was extensive, lymphedema, secretion, and lymphocele may be inevitable. This may partly be avoided by limiting the dissection to preserve the saphenous vein. 6,22 Even though morbidity may decrease, these techniques were not able to demonstrate equivalent oncologic control with a 5.5% local recurrence rate in patients with negative simplified dissection during follow-up. 6 Alternatively, sentinel node biopsy according to lymphoscintigraphy is gaining increasing acceptance. 22 Although results were excellent when looking at morbidity, there is a 15% incidence of inguinal recurrence deteriorating with patient prognosis. 23
We are presenting the largest series so far comparing E-IFLA and O-IFLA showing a clear superiority of the endoscopic approach. Perioperative and postoperative outcomes are more favorable while oncologic outcome does not seem to be compromised. Even though long-term assessment is still lacking, node count may be used as an important surrogate to determine the quality of lymph node dissection. Similar observations were made for malignant melanoma. 7,24
There is no difference in the nodal yield between O-IFLA and E-IFLA. The average number of nodes are within the range of a high-standard node dissection when looking at previous dissection on nodal yield and quality of groin lymphadenectomy. Spillane and coworkers 24 have shown that seven or more lymph nodes can be considered a reliable threshold. Here, we reach this level in both the open and the endoscopic technique (more than 70% of the patients had ≥7 nodes removed in the E-IFLA group). Moreover, we performed E-IFLA simultaneously in the majority of our patients, helping to reduce both hospital stay and anesthesia time.
Looking at the morbidity of E-IFLA in our comparative series, we believe that distal femoral incisions allow us to preserve the vasculature of the skin and its lymphatics. Moreover, because the femoral vessels are not exposed, additional coverage by a sartorius muscle flap is not necessary. Small lymphatic vessels were easily identified endoscopically and sealed with a vessel sealing device. Larger vessels were controlled with clips, to reduce lymphatic leakage and to avoid subsequent lymphoceles. These facts may contribute to a decreased risk for leg edema and lymphocele formation. In our modified approach, we use an extremely low insufflation pressure to minimize CO2-related complications, including hypercapnia and emphysema. This is much lower than reported in previous series. 14,19,25 Even the reduced pressure was sufficient to obtain a reliable working space. Moreover, minor bleeding could be identified easily during surgery. Hence, postoperative bleeding risk may be limited using this technique.
In contrast to the aforementioned series, we are now able to look at a longer follow-up to reassess the oncologic efficacy and durability of E-IFLA. During an extended follow-up of up to 6 years, we have not recorded any local recurrence at the respective groin after E-IFLA. The CO2-related spilling of malignant lymph node material does not seem to influence the outcome of E-IFLA. Long-term results with a follow-up of more than 5 years, however, are still not available.
In this series, we have incorporated both penile cancer patients and also other genitourinary malignancies. Therefore, the conclusions drawn may be limited. On the other hand, the node dissection used was identical for all cancers, and E-IFLA may be also applicable to other cancers. Master and colleagues 26 have also shown in a very recent series that the complication rate of endoscopic groin dissection was much lower than in the open approach. They used a standardized reporting system showing minor complications in 27% and major complications in 14.6%, respectively. Hence, the procedure is safe, even in patients with significant comorbidities and a high body mass index. Interestingly, they have demonstrated a higher lymph node yield in their series, which may be attributed to a technical difference compared with our series. They routinely start the plane of dissection superficial to the Scarpa fascia, resulting in higher lymph node yields without severely compromising skin vascularity. In their series, there was only one patient in whom flap necrosis developed. Even a more extensive endoscopic dissection, however, still seems to be safer than any open approach.
Conclusion
The fact that E-IFLA has become a standardized approach is shortening the learning curve for novice surgeons. It is technically feasible even in a high-risk situation and larger palpable nodes. Large, bulky, matted nodes, however, remain a relative contraindication. This is especially true for novice surgeons when experience in the endoscopic technique is limited. The complication rate observed with this technique is lower than in modern open series. Larger prospective studies comparing E-IFLA to the sentinel technique and to a conventional open approach, however, are needed to ultimately assess the value of this novel approach. Finally, the issue of quality of life after inguinal lymhadenectomy has to be addressed. 3
Footnotes
Acknowledgment
This article was presented in part at the World Congress of Endourology 2011, Kyoto, Japan.
Disclosure Statement
No competing financial interests exist.