
Abstract
Purpose:
To evaluate if hematologic parameters and inflammatory markers could predict extravesical tumor and overall survival after radical cystectomy for patients with recurrent high grade T1 or muscle-invasive bladder cancer.
Patients and Methods:
A total of 68 consecutive cases of radical cystectomy performed with curative intent at our institution between April 2005 and October 2011 with preoperative hematologic parameters are included in this analysis. We evaluated preoperative characteristics with univariable and multivariate Cox proportional hazard ratios to assist in risk stratification for overall survival. Relative risk (RR) ratios and 95% confidence intervals (CI) were created. We also identified factors associated with extravesical tumor extension with logistic regression analysis.
Results:
Median overall survival in the total cohort was 25 months (95% CI 13–61). In multivariate analysis, neutrophil/lymphocyte ratio <2.5 (RR 2.49; 95% CI 1.14–6.09), hypoalbuminemia (RR 4.96; 95% CI 2.18–11.67), pT3/4 (RR 7.97, 95% CI 3.16–24.83), and lymph node positive disease (RR 2.62, 95% CI 1.26–5.46) predicted overall survival. These were statistically significant for cancer-specific survival as well. Both elevated neutrophil/lymphocyte ratio (RR 3.18, 95% CI 1.09–9.79) and hypoalbuminemia (RR 3.72, 95% CI 1.12–15.00) were associated with risk for extravesical disease.
Conclusions:
Serum neutrophil/lymphocyte ratio and hypoalbuminemia predict overall and cancer-specific survival in patients undergoing radical cystectomy for muscle-invasive bladder cancer. These parameters also predict risk for extravesical disease. These could be combined with other established preoperative parameters to improve risk stratification and preoperative counseling.
Introduction
There has been a relationship established with bladder cancer development and inflammation. 2 Schistosomiasis, which produces a chronic infection and inflammatory state, is associated with development of bladder cancer. 3 Chronic catheterization produces a chronic inflammatory state, and patients with indwelling urinary catheters have a significantly higher rate of bladder cancer. 4 In case-control series, anti-inflammatory mediators, other than phenacetin, have been associated with a decreased risk of bladder cancer. 5
The neutrophil/lymphocyte ratio (NLR) is established as measure of inflammatory reaction for patients and can provide information concerning risk stratification. In patients undergoing other curative procedures for malignancy, the NLR is associated with overall and cause-specific survival. This includes gastric, 6 hepatic, 7 nonsmall-cell lung, 8 and cervical cancer. 9 In patients in whom muscle-invasive bladder cancer develops, as well as selected patient with nonmuscle-invasive disease, the gold standard for treatment is radical cystectomy with extended pelvic lymphadenectomy. 10,11 Only one other group of investigators has established a relationship between radical cystectomy and NLR, and they identified NLR in predicting cause-specific survival. 12
Based on the relationship between inflammatory response and bladder cancer, and the trend that preoperative NLR predicts outcomes in other surgical cases, we evaluated whether this pattern was repeated in patients undergoing radical cystectomy. Specifically, we investigated whether we could predict overall survival in bladder cancer based on the NLR or other preoperative parameters.
Patients and Methods
Before initiating this analysis, we obtained approval from our Institutional Review Board in recognition of and compliance with the United States Health Insurance Portability and Accountability Act of 1996 guidelines. A retrospective analysis was performed from a prospectively maintained database of bladder cancer patients, and we identified 68 consecutive patients who underwent radical cystectomy with bilateral lymphadenectomy with curative intent between April 2005 and October 2011. Data were compiled prospectively from individual patient medical case notes, electronic patient records (for laboratory results), and pathology reports. Survival status was determined from the date of last follow-up in a hospital outpatient clinic or general practitioner clinic in conjunction with the United States Social Security Death Index accessed on April 19, 2012.
In patients undergoing radical cystectomy, we defined leukocytosis as having a total white blood cell count >109 cells/mL. 13 In addition, anemia was considered a hemoglobin concentration <12.5 mg/dL in women or 13.5 mg/dL in men. 13 Hypoalbuminemia was defined as patients with serum albumin <3.5 g/dL. 14 Thrombocytopenia was all patients with a platelet count <1.5×105/μL, 13 thrombocytosis refers to all patients with platelet counts >5×105/μL, 13 and neutrophil lymphocyte ratio (NLR) was used a priori based on previous publications with an abnormal value defined as >2.5. 12 Patients with a documented history of chronic obstructive pulmonary disease, on pharmaceutical therapy for diabetes, or having a history of a cardiovascular event had these comorbidities included in the survival analysis. All hematologic parameters in patients with neoadjuvant chemotherapy were calculated after conclusion of chemotherapy and before cystectomy. Extravesical extension included all patients with cancer either locally (pT3, pT4) or systemically (node positive) beyond the detrusor.
Categoric variables are presented as percentages and continuous variables as means with standard deviation. Actuarial survival was estimated using the Kaplan-Meier method with differences tested using the log-rank test. Cox proportional hazards regression was used to evaluate individual contribution of factors associated with survival and to compare the stage-adjusted survival. Nominal logistic regression was performed for evaluation of factors associated with extravesical disease. Statistical analysis was performed using JMP 9 (Cary, NC).
Results
From April 2005 through October 2011, 68 consecutive patients with preoperative complete blood cell counts and differentials underwent radical cystectomy with curative intent at our institution. The purpose was both management of bacille Calmette-Guérin (BCG) refractory high-grade disease and muscle-invasive bladder cancer. Extended pelvic lymph node dissection was performed in all cases. Mean age for the cohort was the mean age is 67.4 years, and 55 (80%) of patients were male. Of these, 32 (47%) had a minimally invasive (robot-assisted) procedure. The baseline demographics and preoperative serum laboratory values are outlined in Table 1. Ten (15%) patients received neoadjuvant chemotherapy. Twelve (18%) patients had cystectomy for BCG refractory noninvasive disease. Complete blood cell count with differential was obtained a median of 13 days before their procedure.
SD=standard deviation.
Median overall survival was 25 months (95% confidence interval [CI] 13–61) (Fig. 1). Using Cox proportional analysis, we identified multiple preoperative parameters associated with survival in the cohort, including hypoalbuminemia, elevated serum creatinine (>1.4 g/mL), history of muscle invasion on previous resection, pathologic T3 or T4, node positive disease, and NLR ratio >2.5 (Table 2). Patient comorbidities including diabetes history, chronic obstructive pulmonary disease, or cardiovascular events were not associated with overall survival. While neoadjuvant chemotherapy was associated with improved overall survival, this did not reach statistical significance. All of these except elevated serum creatinine and history of T2 disease remained significant on multivariate analysis.
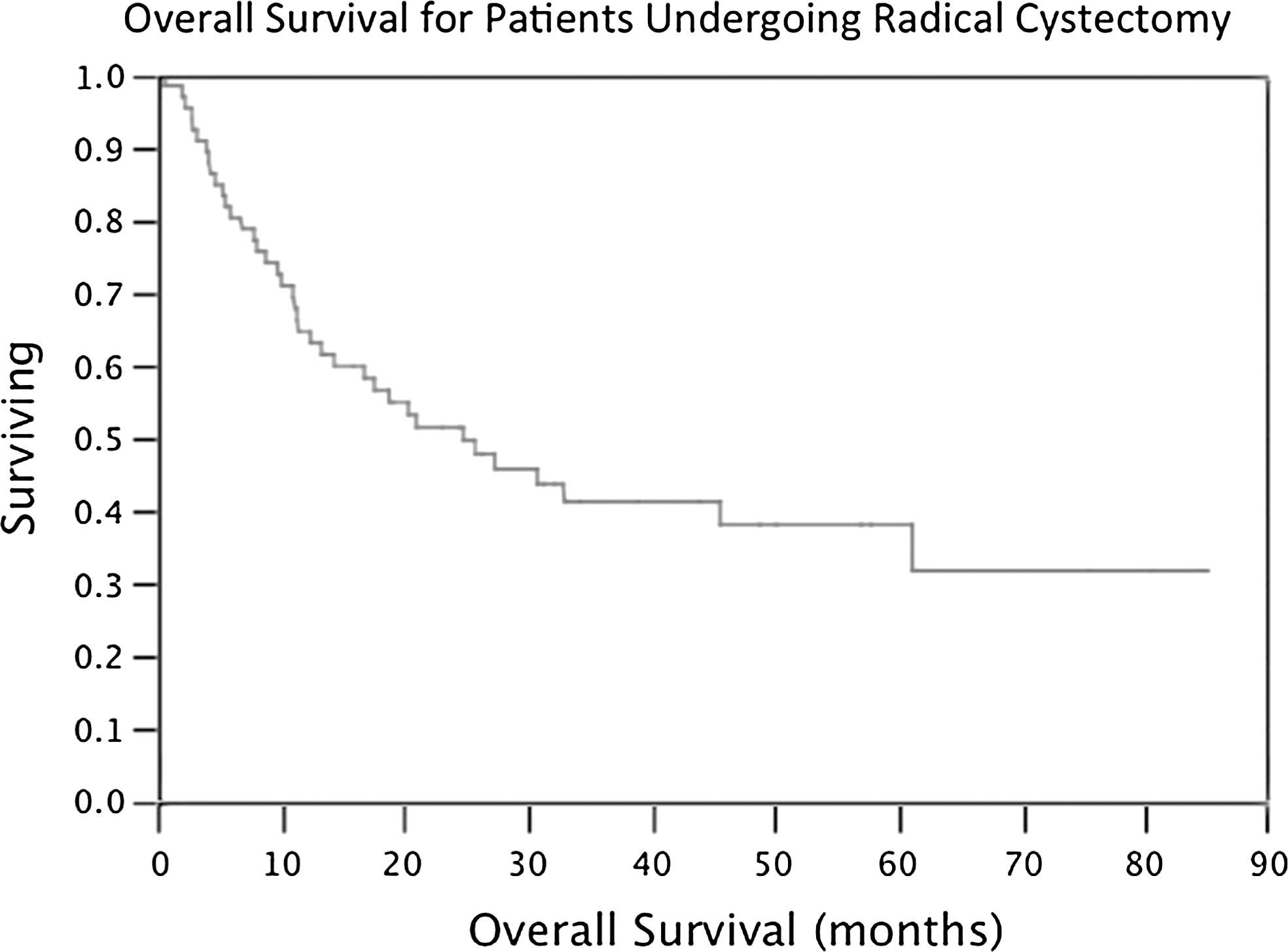
Overall survival in patients undergoing radical cystectomy.
RR=relative risk; CI=confidence interval; BCG=bacilli Calmette-Guérin; CR=creatinine; NLR=neutrophil/lymphocyte ratio; LN=lymph node.
Ten patients had nonmuscle-invasive disease at the time of cystectomy and underwent the procedure for BCG refractory or micropapillary urothelial carcinoma. BCG refractory patients were associated with improved overall survival on the multivariate analysis, but with inclusion on the multivariate analysis, this was no longer statistically significant. Use of robot-assisted surgery was not associated with improved overall survival (relative risk [RR] 1.24, 95% CI 0.82–1.87). Neither lymphocyte count below median (P=0.25) nor neutrophil count above the median (P=0.67) independently predicted overall survival in this cohort. Twenty-five patients included in this study died of bladder cancer. Exclusion of the 10 patients who had neoadjuvant chemotherapy did not affect the statistical significance of any parameter associated with overall survival in the Cox proportional hazard multivariate model.
An NLR of >2.5 was associated with decreased cancer-specific survival as well, with a mean 23 months vs 36 months (log rank 0.04). Using a multivariate analysis with the same variables used as in the overall survival, we found that NLR <2.5, RR 2.68 (1.01–8.59), hypoalbuminemia RR 8.10 (2.63–27.59), pT3 RR 19.61 (5.00–135.6), and nodal disease RR 5.11 (1.94–14.94) remained the only statistically significant predictors of cancer-specific survival as well.
In the cohort, we also found that the patients who had a NLR >2.5 had a significantly higher likelihood of extravesical bladder cancer (RR 3.20, 95% CI 1.14–9.38) (Table 3). Of all the other preoperative variables tested, only hypoalbuminemia was also associated with extravesical disease, and both of these remained significant on the multivariable analysis. Thrombocytopenia or thrombocytosis was not associated with survival or extravesical disease in this cohort.
RR=relative risk; CI=confidence interval; CR=creatinine; NLR=neutrophil/lymphocyte ratio.
Discussion
Radical cystectomy with extended lymphadenectomy remains the standard of care for the treatment of patients with muscle-invasive and select nonmuscle-bladder cancer who are thought to be good surgical candidates. 10 It provides durable long-term survival with acceptable perioperative morbidity. Even at high-volume centers with experienced surgeons, however, a significant portion of patients will succumb to their disease within 5 years of their procedure. 10,11,14 Our observations highlight many of the findings that are well-established in patients with bladder cancer—namely, the importance of risk stratification.
Hypoalbuminemia is a well-established negative prognostic indicator for patients undergoing almost any surgical procedure. 15 In bladder cancer, it is well established that decreased albumin is associated with worse outcomes, and this is typically attributed to its role in identifying nutritional status. 16 Albumin can be influenced by outside factors including inflammation and stress, however. In patients with elevation in acute phase reactants including C-reactive protein (CRP), albumin levels are markedly decreased. Because cancer causes an inflammatory response, it limits endogenous albumin production and thus helps to explain why these patients perform poorly at the time of cystectomy.
Anemia is an established consequence of bladder cancer and can predict responses to multiple therapies. In patients undergoing radical cystectomy, Thrasher and colleagues 17 found survival was significantly reduced in patients with a preoperative hemoglobin concentration ≤12 g/dL. For patients undergoing treatment with external beam radiation for muscle-invasive bladder cancer, local control was improved in patients without pretreatment anemia. 18 Joynson and researchers 19 did not find local control was inferior in anemic patients; however, there was improved overall and metastases free survival in patients who were not anemic. In patients with metastatic urothelial carcinoma, anemia had the strongest relationship of all variables in predicting overall survival for those receiving vinlufine for platinum chemotherapy failures. 20
It is well established that inflammation is associated with cancers throughout the body, and bladder tumor in particular. 2 The evidence for inflammation and development of squamous-cell carcinoma of the bladder is well established. Chronic indwelling Foley catheters, chronic urinary tract infections, and schistosomiasis have all been well established. The connection between inflammation and urothelial carcinoma, the predominant subtype seen in developed countries, is not as clear-cut. Anti-inflammatory therapy has been evaluated in case control studies in the United States, and this has shown a decreased incidence of bladder cancer. In fact, in regular analgesic users, a 19% decrease in bladder cancer was noted. 5 In a pooled analysis of three large prospective trials, other authors have confirmed this effect, although their research suggests that this association may be limited to smokers. 21
In addition, inflammatory markers have been shown to predict outcomes in patients undergoing management of urothelial carcinoma. In patients undergoing chemotherapy and radiation for muscle-invasive bladder cancer, Yoshida and associates 22 found a strong relationship between C-reactive protein levels, a surrogate for inflammation, and overall survival. In fact, in their cohort, normalization of CRP after therapy also predicted overall survival. 22 Gakis and coworkers 23 noted an elevated CRP predicted worse overall survival in patients undergoing radical cystectomy. Similarly, Gondo and colleagues 12 found that in their cohort of patients undergoing radical cystectomy, elevated NLR or CRP portended inferior disease-specific survival at 5 years. 12
Preoperative evaluation of inflammatory markers has assisted in treatment recommendations in other malignancies. In advanced rectal cancer, NLR predicts response to neoadjuvant chemotherapy and has been recommend for subsets of these patients. 24 In esophageal carcinoma, NLR predicts response to neoadjuvant chemotherapy as well. 25 The urologic community has been receptive to large trials based on individual or tumor characteristics for bladder cancer, including recently a large adjuvant chemotherapy trial based on p53 status of the primary tumor. 26 Future trials with NLR determining randomization may provide improved outcomes in this cohort of patients.
Previous studies evaluating NLR and bladder cancer evaluated this in relation to disease-specific survival. One of the strengths of this article is that we have shown that NLR is associated with overall survival in addition to bladder cancer-specific survival in this cohort. In fact, it is as important as previous well-established markers such as hypoalbuminemia, and this relationship is independent of lymph node status or extravesical disease on final pathologic analysis. Even when taking into account well-established risk factors for poor survival including node positive disease or pT3 disease, an elevated NLR remains a statistically significant predictor of survival. These factors were more important to overall survival in this cohort than comorbidities, including cardiovascular event history, chronic obstructive pulmonary disease, and diabetes mellitus.
We believe this is the first study in patients with bladder cancer to identify NLR as a possible risk identifier for patients with extravesical disease. Based on randomized trials, the patients who benefit the most from neoadjuvant chemotherapy are those who have extravesical disease. The SWOG trial had a benefit of 41 months in median survival for patients with pT3/T4 disease who received neoadjuvant chemotherapy compared with those randomized to radical cystectomy alone. 27 Despite level 1 evidence encouraging its use, neoadjuvant chemotherapy remains underutilized in patients with bladder cancer, even at high-volume academic institutions. 28,29 In our cohort, only 10 (15%) of patients received neoadjuvant chemotherapy. Identification of patients at high risk for extravesical disease could assist in preoperative counseling and possible encouragement of neoadjuvant chemotherapy.
Several limitations of our study need further discussion. Only 15% of patients received preoperative chemotherapy, so these findings might not be applicable to other institutions. In addition, because neutropenia is a known side effect of chemotherapy, it is possible that these patients confound the results. Another concern in determining survival is using the Social Security Death Index to validate patient status. As a tertiary referral center, the majority of the patients who have procedures performed at this institution return to their primary urologist for follow-up, and therefore it is necessary to supplement our hospital records with additional information. The Social Security Death Index has reported sensitivities and specificities as high as 100%, 30 and therefore we believe using this database does not significantly alter our findings.
Systemic inflammatory response to urothelial carcinoma is seen in patients with aggressive bladder cancer and portends poor prognosis. Future investigations into these relationships, including measuring proinflammatory cytokines, may provide further insight into the carcinogenesis and progression to extravesical or systemic disease. These provide interesting and potentially targetable areas for future systemic therapies before surgical management.
Conclusions
Patients with elevated NLR before radical cystectomy have worse overall survival than patients without markers of systemic inflammation. NLR is also associated with extravesical disease and may provide assistance in risk stratification for patients suspected of harboring advanced disease.
Footnotes
Disclosure Statement
No competing financial interests exist.