
Abstract
Background:
To evaluate the effects of hyaluronic acid (HA) and carboxymethylcellulose (CMC) on the recurrence of urethral stricture after treatment with endoscopic internal urethrotomy (EIU).
Methods:
A total of 120 patients underwent EIU for urethral stricture. Recruited patients were randomly divided into two groups: group A and B. Patients in group A (60 patients, experimental group) received HA/CMC instillation and patients in group B (60 patients, control group) received lubricant instillation after internal urethrotomy. Each patient was evaluated at 4 weeks (V1), 12 weeks (V2), and 24 weeks (V3) after the surgery. The effectiveness of HA/CMC instillation was evaluated based on the International Prostate Symptom Score/Quality of Life, peak urine flow rate, voided volume and postvoiding residual urine volume. The visual analogue scale (VAS) pain score and degree of satisfaction were also determined for each participant.
Results:
Among 120 initial participants, 53 patients in group A and 48 patients in group B had completed the experiment. VAS pain scores were 0.67±0.76 and 3.60±1.52 (p<0.001), and degrees of satisfaction were 0.28±0.50 and 0.80±0.81 in group A and group B at 1 month after surgery (p=0.001). The recurrence of urethral stricture was observed in five cases (9.4%) in group A and 11 (22.9%) in group B (p=0.029).
Conclusions:
HA/CMC instillation during EIU may decrease the incidence of urethral stricture recurrence. In addition, the use of HA/CMC was effective in reducing pain during the early postoperative period without an adverse effect.
Introduction
The anionic polysaccharide HA is a major constituent of the extracellular matrix and is thus found in the connective tissue, skin, cartilage, and synovial fluid. It is a hydrophilic and nonimmunogenic macromolecule that easily coats and lubricates mucus membranes. These physical properties of HA enable it to reduce or prevent trauma at the site of surgery. 9 CMC is derived from cellulose by the carboxymethylation of glucosidic hydroxyl groups and is another type of anionic polysaccharide. CMC is significantly more hydrophilic than cellulose and is used as a filler, viscosity agent, lubricant, or stabilizer of pharmaceutical products. 10 Consequently, the combination of HA and CMC (HA/CMC) has been used to prevent adhesions from forming after surgery. 11,12 Prospective studies testing the effectiveness with which HA/CMC applied during surgery can prevent urethral restricture have not been performed. In the present study, we tested the effectiveness with which HA/CMC prevents restricture of the urethra after EIU treatment.
Patients and Methods
Subjects and study design
A total of 120 patients who were treated for urethral stricture by EIU between January 2010 and June 2011 were invited to participate in the present study. This study is a multicenter, randomized controlled, single-blinded study involving seven medical institutions. The study was approved by the institutional review board.
Inclusion criteria were (1) a urethral stricture observed by retrograde urethrography and (2) patients who were willing and able to participate in the present clinical study. Patients who (1) had undergone EIU in the past to treat urethral stricture, (2) had undergone any other transurethral surgeries, (3) had undergone radical prostatectomy for prostate cancer, (4) had 1.5 cm or more urethral stricture, (5) had a neurogenic bladder, or (6) had a urinary tract infection were excluded from the study.
The patients who met the inclusion criteria were randomized by simple block randomization to either (1) the experimental group (group A, 60 patients who received HA/CMC instillation) or (2) the control group (group B, 60 patients who received an instillation of lubricant at the urethra after EIU).
The primary endpoint was the recurrence of urethral stricture 24 weeks after surgery. The secondary endpoints were voiding symptoms, degree of satisfaction, and pain.
At the beginning of the study (V0), information regarding the duration of illness and the medical history was collected. Retrograde urethrography was also performed during V0 to measure the length of the urethral stricture and to identify the stricture site. Patients were evaluated 4 weeks (V1), 12 weeks (V2), and 24 weeks (V3) after surgery. Failure was defined as the need to repeat surgical intervention due to the lack of improvement in voiding symptoms. In addition, surgical failure was confirmed by retrograde urethrography. Constrictive uroflow curves or a maximum flow rate ≤10 mL/second, as determined by uroflowmetry, were considered to indicate urethral stricture recurrence. Recurrence in patients showing constrictive uroflow curves or a maximum flow rate ≤10 mL/second by uroflowmetry was confirmed by urethroscopy and retrograde urethrography as soon as possible. Peri- and postoperative complications such as wound infections, bleeding, and extravasation were recorded.
Surgical technique
The patient was placed under general or spinal anesthesia and EIU was performed at the 12 o'clock position by using a 21 Fr. Storz urethrotome with a straight cold knife. After urethrotomy, an 18 Fr. Foley catheter was inserted. Upon pulling the Foley to block the bladder neck, 5 mg of HA/CMC (marketed as Guardix-sol®, Hanmi Medicare, Seoul, Korea) or 5 mg of lubricant (chlorhexidine gel) was instilled by using an 18-gauge tube catheter between the urethral lumen and the Foley catheter. After instillation, gauze was used to maintain the traction of the Foley catheter, which enabled to blockade the bladder neck (Fig. 1). To minimize absorption of the HA/CMC gel by the gauze, the gauze was tied and the Foley catheter was placed such that it faced upward and was fixed on the abdomen. Moreover, the patients were kept on bed rest in a supine position, while traction was maintained on the Foley catheter. One day after surgery, gauze traction was removed. The Foley catheter was removed 2 weeks after EIU.

Instillation of hyaluronic acid (HA)/carboxymethylcellulose (CMC) on urethra using 18-gauge catheter
Assessment of efficacy and safety
To evaluate the ability of HA/CMC to prevent urethral stricture recurrences, the International Prostate Symptom Score (IPSS), peak urine flow rate (Qmax), and postvoiding residual urine volume (PVR) were determined at every visit. Retrograde urethrography was performed routinely at V2. The degree of patient satisfaction was recorded on a scale ranging from 0 (extremely satisfied) to 3 (extremely dissatisfied). The visual analogue scale (VAS) pain score was assessed on a 10-point Likert scale and the Quality of Life (QoL) score was also determined. The safety of HA/CMC treatment was assessed at V1, V2, and V3 on the basis of the patient's history, a physical examination, and the presence or absence of adverse effects.
Statistical analysis
The recurrence rate was evaluated by per protocol analysis based on the number of patients who completed the study. Preoperative characteristics, including the site and length of urethral stricture, were evaluated by intent-to-treat analysis. Voiding symptoms, Qmax and PVR, were compared by using the Student's paired t-test. The chi-square test was used to analyze the recurrence rate, causes, and locations of urethral stricture. The patients who had no recurrence were compared to those who had recurrence in terms of voiding symptoms, pain scale, and degree of satisfaction. SPSS software v.18.0 was used for statistical analysis, and a p-value <0.05 was considered to be statistically significant.
Results
Analysis of the intention-to-treat population revealed that groups A and B did not differ significantly in terms of the location and length of urethral stricture (Table 1).
Student t-test.
Chi-square test.
BMI=body mass index; IPSS=International Prostate Symptom Score; QoL=Quality of Life; PVR=postvoiding residual urine volume.
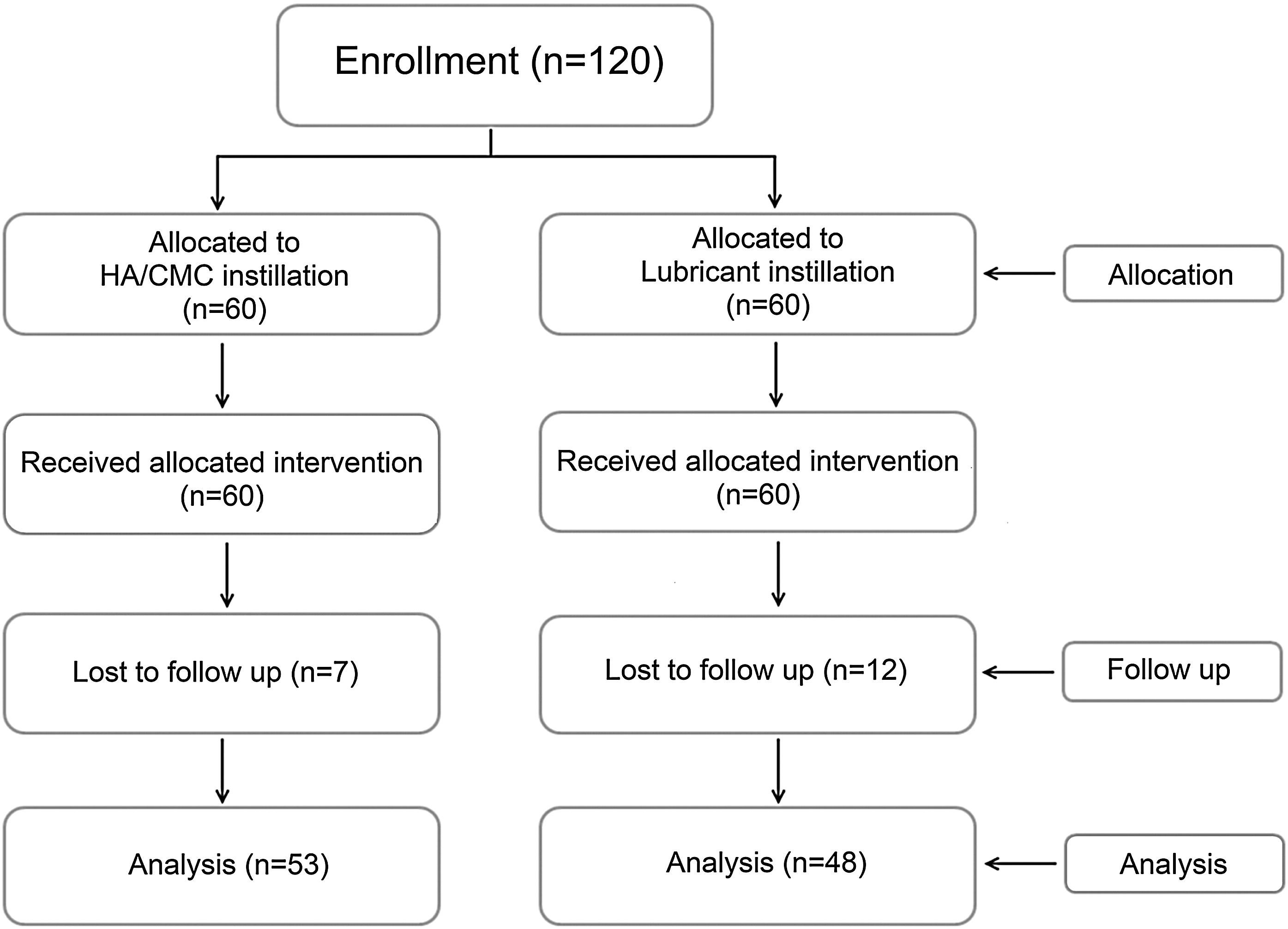
Seven group A (HA/CMC) and 12 group B (lubricant) patients were lost to follow-up. Thus, 53 group A and 48 group B patients completed the follow-up period. The postoperative outcomes of this per-protocol population were analyzed as follows (Fig. 2).
This 26-week study involved a 2-week screening period and a 24-week treatment phase.
As shown in Table 1, six group A (11.32%) and seven group B subjects (14.58%) showed no improvement of symptoms, which was interpreted as failure of the surgery (p=0.473). Urethral stricture recurrence was observed in five group A (9.4%) and 11 group B cases (22.9%) (p=0.029) (Table 1). Table 2 showed the baseline characteristics of patients deemed to have experienced surgical failure and recurrence groups. The urethrogram performed at V2 showed that patients who did not experience recurrence or failure had no narrowing.
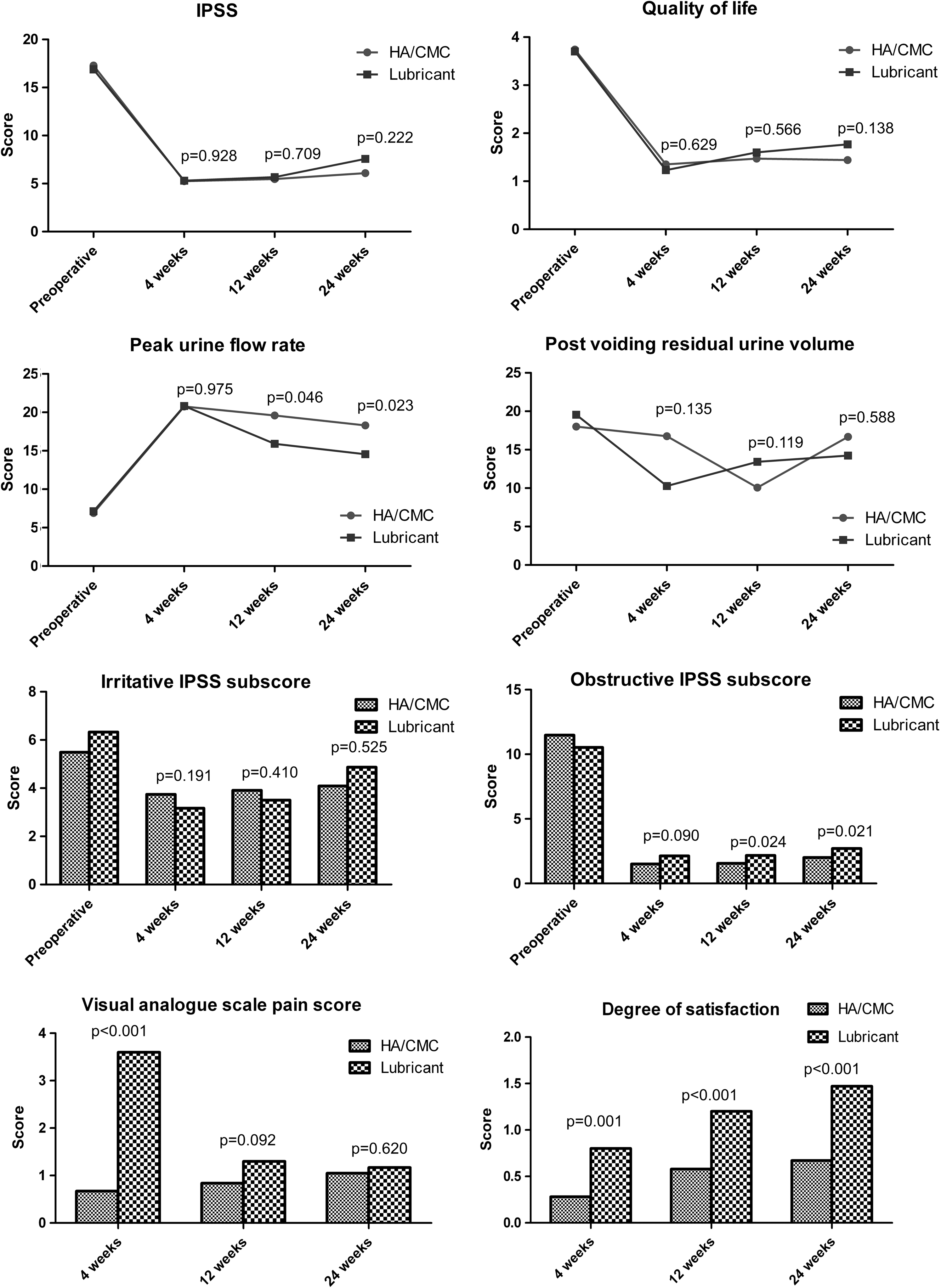
The VAS pain scores of the group A and B patients were 0.67±0.61 and 3.60±1.52, respectively, at 4 weeks after surgery (p<0.001), and the degree of satisfaction in groups A and B was 0.28±0.23 and 0.80±0.71, respectively (p=0.001). Twelve weeks after surgery (V2), the degree of satisfaction in groups A and B was 0.58±0.53 and 1.20±0.81, respectively (p<0.001). Twenty-four weeks after surgery (V3), the degree of satisfaction in groups A and B was 0.67±0.60 and 1.47±1.07, respectively (p<0.001). At V2, the Qmax values were 19.60±8.99 mL/second for group A and 15.91±5.14 mL/second for group B (p=0.046), and the PVR values were 10.08±8.42 and 13.43±9.22, respectively (p=0.119). The obstructive IPSS subscores were 1.56±1.18 and 2.17±5.67 for groups A and B, respectively (p=0.024). QoL scores were 1.47±1.05 for group A and 1.60±0.93 for group B (p=0.566). The group A and B Qmax values at V3 were 18.31±8.37 mL/second and 14.55±5.67 mL/second, respectively (p=0.023). PVR values were 16.67±26.54 in group A and 14.23±10.64 in group B (p=0.588), and their obstructive IPSS subscores were 2.00±1.22 and 2.70±1.26, respectively (p=0.021). QoL scores were 1.42±1.03 for group A and 1.77±0.94 for group B (p=0.138). However, the two groups did not differ significantly in terms of total IPSS scores at V1, V2, or V3 (Fig. 3).
Comparison of voiding symptoms after EIU of patients who did not recur or failed.
Postoperative complications, including urethral bleeding, extravasation, chordee, incontinence, and infection, were not seen. Burning sensations or irritation of the urethra due to HA/CMC were also not observed.
Discussion
The present study showed that the intraurethral instillation of HA/CMC during EIU significantly reduced the recurrence of urethral stricture after EIU. Moreover, 24 weeks after surgery, the experimental group had a better voiding symptom than the control group. Thus, HA/CMC was effective. It also had no noticeable side effects and helped to lessen the pain after surgery.
EIU is the primary treatment option for urethral stricture because of its simplicity and effectiveness. However, the success rate of EIU is low (about 40%) and the recurrence rate is high. 13 Although the mechanisms behind urethral stricture recurrence after EIU are not yet understood clearly, fibrosis and adhesion of epithelial and subepithelial spongy tissues during healing are likely to be involved. 14 Holm-Nielsen et al. reported that the post-EIU recurrence rate of urethral stricture was 23%–80%. 15 In contrast, the recurrence rate of the control group in the present study was 22.9%. This disparity may reflect the fact that the present study had a shorter follow-up period than the previous study. Nevertheless, compared to the control group in our study, the post-EIU recurrence rate of urethral stricture in the experimental group was significantly reduced (9.4%).
Of the many techniques that have been used to reduce the recurrence rate, laser has several advantages over conventional surgery, including the ability to control bleeding (which improves working visibility) and the ability to remove fibrotic tissues by vaporization during incision of the urethra. However, despite laser being associated with a high success rate and a low recurrence rate, laser does not differ significantly from conventional methods in terms of long-term outcomes. 5,16
Postoperative self-catheterization is sometimes suggested as a method that can reduce the recurrence rate. However, one study found that it did not significantly reduce the recurrence of urethral stricture as compared to the control group. 6 With regard to other methods that may reduce recurrence, use of an antifibrotic angiotensin-converting enzyme-inhibitor gel after performing EIU has been suggested to reduce urethral stricture recurrence possibly by inhibiting fibrosis. 7 In addition, injection of a steroid at the stricture point during EIU was recently reported to postpone, but not reduce, urethral stricture recurrence. 8 The physiological properties of corticosteroids suggest that they may decrease scar formation by reducing the synthesis of collagen, glycosaminoglycans, and inflammatory mediators. 17 (Table 3).
Extracellular matrix regulation plays a prominent role in this process, and it has been reported that sodium hyaluronate may reduce unwanted scar tissue by 50% or more. 18 Moreover, histological analysis in an animal study by Hong et al. revealed that the group treated with HA/CMC exhibited fewer fibrous tissue attachments at the adhesion tissue after surgery. 19
In the human body, several natural barriers, including the peritoneum, omentum, and amnion, serve to prevent adhesion between neighboring tissues. When surgery breaches these barriers, a synthetic physical barrier can be introduced to separate the surface of injured tissue from the surrounding tissues, thereby reducing adhesion of the injured tissues to the nearby organs. 20 HA/CMC is a fluid synthetic sol-gel barrier with a viscosity of 2500–3500 cP, similar to that of honey. 19 In the present study, the idea to use HA/CMC to reduce post-EIU urethral stricture recurrence was based on previous studies showing that the instillation of synthetic solutions as tissue barriers during EIU inhibits scar formation. 10,19
In the present study, the patients who did not have stricture recurrence had significantly better Qmax values, IPSS obstructive subscores, and postoperative pain. HA/CMC effectively coats the wound surfaces and maintains this activity for a long time because of its high viscosity. HA/CMC instillation during EIU may reduce postoperative urethral narrowing because it can prevent fibrosis and scar formation during healing of the urethrotomy wound. The fact that the patients treated with high-viscosity HA/CMC experienced significantly less postoperative pain than the lubricant-treated patients can be attributed to the extended presence of a lubricating barrier between the urethra, the urethrotomy wounds, and the Foley catheter.
Many different lubricants are used for urethral catheterization. The chlorhexidine gel is widely used for this procedure. 21 However, there are no studies of the effects of lubricants on the recurrence of urethral stricture. Future studies should look at the impact of different lubricants on the recurrence of urethral stricture after EIU.
The limitations of the present study include a short follow-up period and the absence of postoperative histological examinations of the experimental and control groups. We did not exclude the benign prostatic hyperplasia patients. The heterogeneity of the urethral stricture sites may be a limitation of the current study. And the absence of a power calculation can be a limitation. However, the present study is significant because it is the first prospective and randomized controlled study of the ability of HA/CMC to reduce the recurrence of urethral stricture after EIU treatment. The long-term effects of HA/CMC instillation during EIU should be confirmed by extended follow-up, and the histological effects should be delineated by animal experimentation.
Conclusions
The instillation of HA/CMC into the urethra during EIU decreased the incidence of urethral restricture after surgery. Use of HA/CMC also reduced postoperative pain effectively without significant side effects.
Footnotes
Acknowledgment
This study was sponsored by Hanmi Medicare, Seoul, Korea.
Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.