
Abstract
Objective:
To describe the first series of robot-assisted laparoscopic radical prostatectomy (RALP) using the ALEXIS™ trocar device when removal of the specimen is necessary for intraoperative frozen-section pathology.
Materials and Methods:
Consecutive RALP using the ALEXIS were prospectively catalogue. Perioperative data, including preoperative oncologic diagnosis, operative time, estimated blood loss (EBL), size of incision for umbilical trocar, complications related to trocar, and length of hospital stay, were analyzed.
Results:
One hundred twenty-eight patients were analyzed. The mean operative time was 216 minutes, mean time to trocar placement was 4 minutes, and mean EBL was 172 mL. The incision size for a trocar was 2–3 cm in 117 patients and 1 incisional hernia was observed. The mean hospital stay was 3 days and mean follow-up was 4 months.
Conclusion:
The ALEXIS trocar provides an easy and fast intraoperative removal of the specimen for frozen pathology during RALP, even for large prostates. Safe and cosmetic results with a low intraoperative complication rate are acquired with the wound retractor.
Introduction
RALP offers several advantages, compared with traditional open methods, including decreased blood loss, shorter hospital stay, and less perioperative morbidity. 2 –6 Recently, a systematic review suggests that RALP is advantageous in terms of perioperative outcomes and both urinary continence and potency recovery in comparison with Radical Retropubic Prostatectomy. 7 However, the fundamental goal of a RALP is to render the patient free from cancer, whereas preserving his current functional status. 8,9
In an effort to improve oncological and functional outcomes, multiparametric magnetic resonance imaging (mp-MRI) in a staging protocol can be used to help nerve and continence sparing surgery and to detect minimal extracapsular disease. 10 In addition, intraoperative frozen-section (IFS) analysis of the neurovascular tissue-adjacent circumference enables a rapid, but comprehensive histologic surgical margin (SM) assessment. IFS may allow the surgeon to intraoperatively demonstrate the oncologic safety of a nerve-sparing (NS) procedure or indicate a secondary wide resection converting to a definitive negative SM. 11,12 However, IFS during radical prostatectomy is still controversial. One point of criticism is that IFS prolongs operation time and consumes resources. 12 –14
We report our technique and the first series of RALP using the ALEXIS™ trocar to provide an easy and fast technique extraction of the specimen from the abdominal cavity for IFS.
Materials and Methods
Study design
All consecutive cases of localized prostate cancer, which underwent RALP using the ALEXIS port device (Applied Medical) at our center between April 2012 and September 2012, were analyzed. Data were prospectively entered in an institutional review board-approved Robotic database and retrospectively reviewed.
Clinical staging was done as per TNM staging and cases with clinical T1-2 (tumor clinically confined to the prostate), N0, M0 were considered for NS RALP. Two patients slightly suspected at MRI of T3 were included. All patients were submitted for an MRI preoperative in a staging protocol to optimize NS. NS was performed as a systematic approach in this group of patients; the suspicion of extracapsular tumor extension preoperatively was an exclusion criteria. We do not perform an NS procedure and IFS in patients with a clear extraprostatic extension. IFS was performed to analyze oncological margins and the requirement about re-resection of neurovascular bundles.
The ALEXIS trocar was inserted as the first trocar (optics port), supraumbilicus, and was used to remove the specimen from the abdominal cavity during the surgery. All surgeries were performed by three surgeons according to our institutional surgical standard and performed using the anteroretrograde technique according to Patel 15 with the da Vinci S model (Intuitive Surgical, Inc.). We routinely performed the posterior reconstruction of the striated sphincter modified by Patel et al. 16 in robotic surgery.
Perioperative data, including preoperative oncologic diagnosis, operative time, estimated blood loss, size of incision for umbilical trocar, complications related to the trocar, conversion to conventional laparoscopic or open surgery, and length of hospital stay, were recorded. The operative time was measured from the skin incision to skin closure and time to insert the ALEXIS.
Port placement and closure technique
The ALEXIS port device has three components: a wound retractor, a cap, and a 12-mm trocar (Fig. 1). The wound retractor is used to amplify the incision and fix the cap.

The ALEXIS™ trocar device: wound retractor and cap.
A 2–3-cm vertical midline supraumbilical skin incision was carried down through the peritoneum. The fascia incision was slightly larger at 3–4 cm; the muscle and peritoneum were bluntly stretched, usually with retractors. The wound retractor was inserted through the incision, the cap was adapted (Fig. 2), and the first 12-mm trocar was inserted for the robotic scope (Fig. 3). During the procedure, the prostate is removed through the ALEXIS and typically requires less than 1–2 minutes (Fig. 4). It is not necessary to undock the patient-side cart.
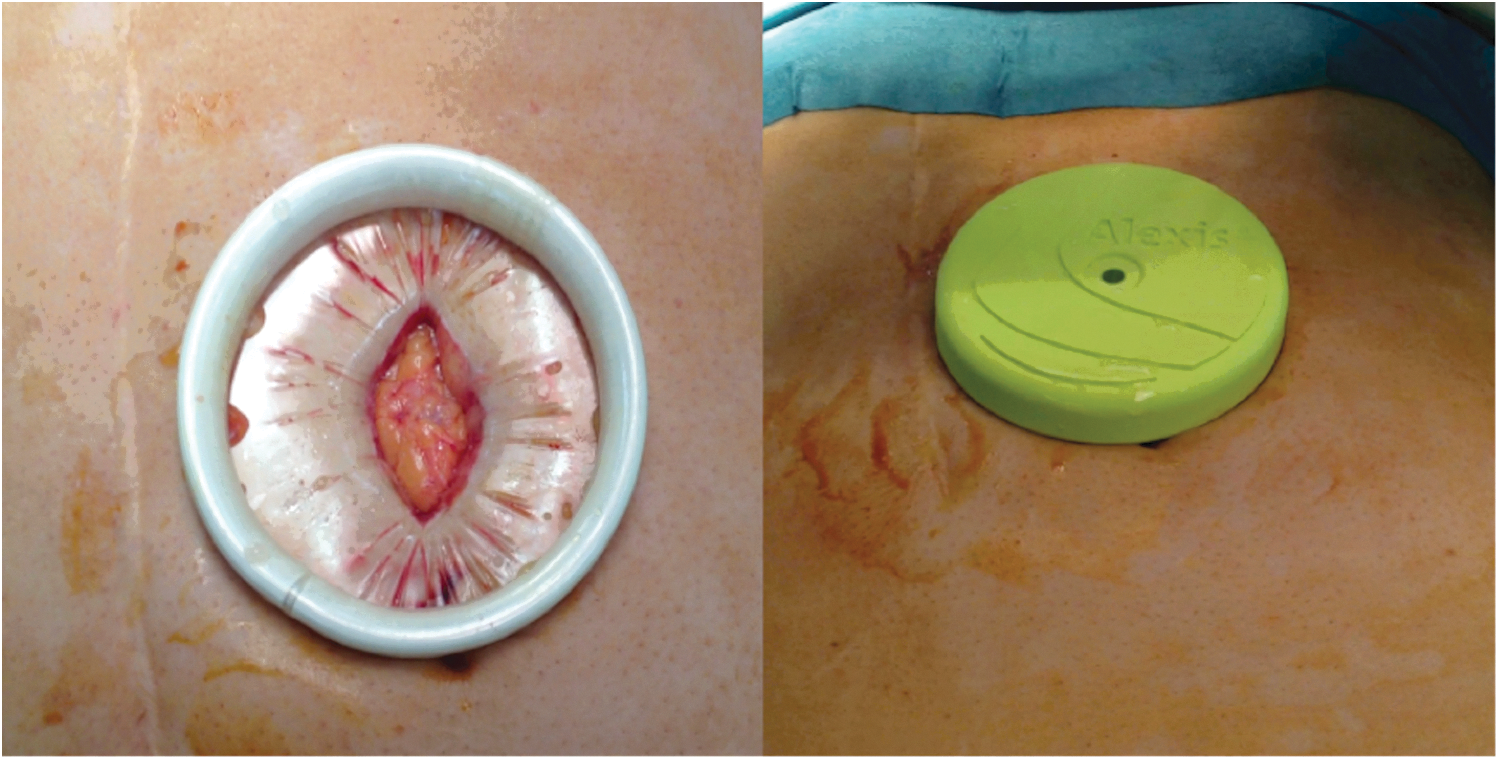
The ALEXIS wound retractor inserted through the incision and the cap adapted.

The first 12-mm trocar was inserted through ALEXIS for the robotic scope.
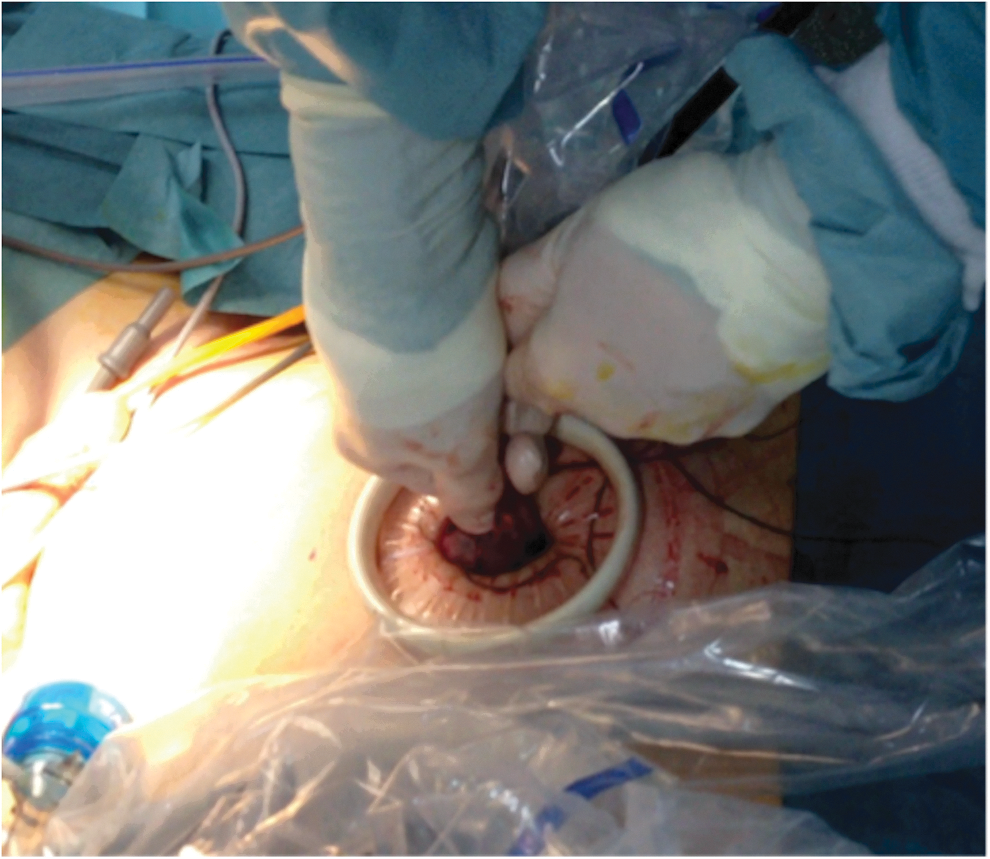
The specimen being removed through ALEXIS.
The fascia was closed vertically with a running and absorbing #1 polyglactin (Vicryl™; Johnson & Johnson Medical, Ltd.) suture, placing the needle deep to the fascia, but superficial to the rectus muscle. No attempt was made to approximate the peritoneum or midline muscle. The skin incisions were reapproximated in a subcuticular manner (Fig. 5).
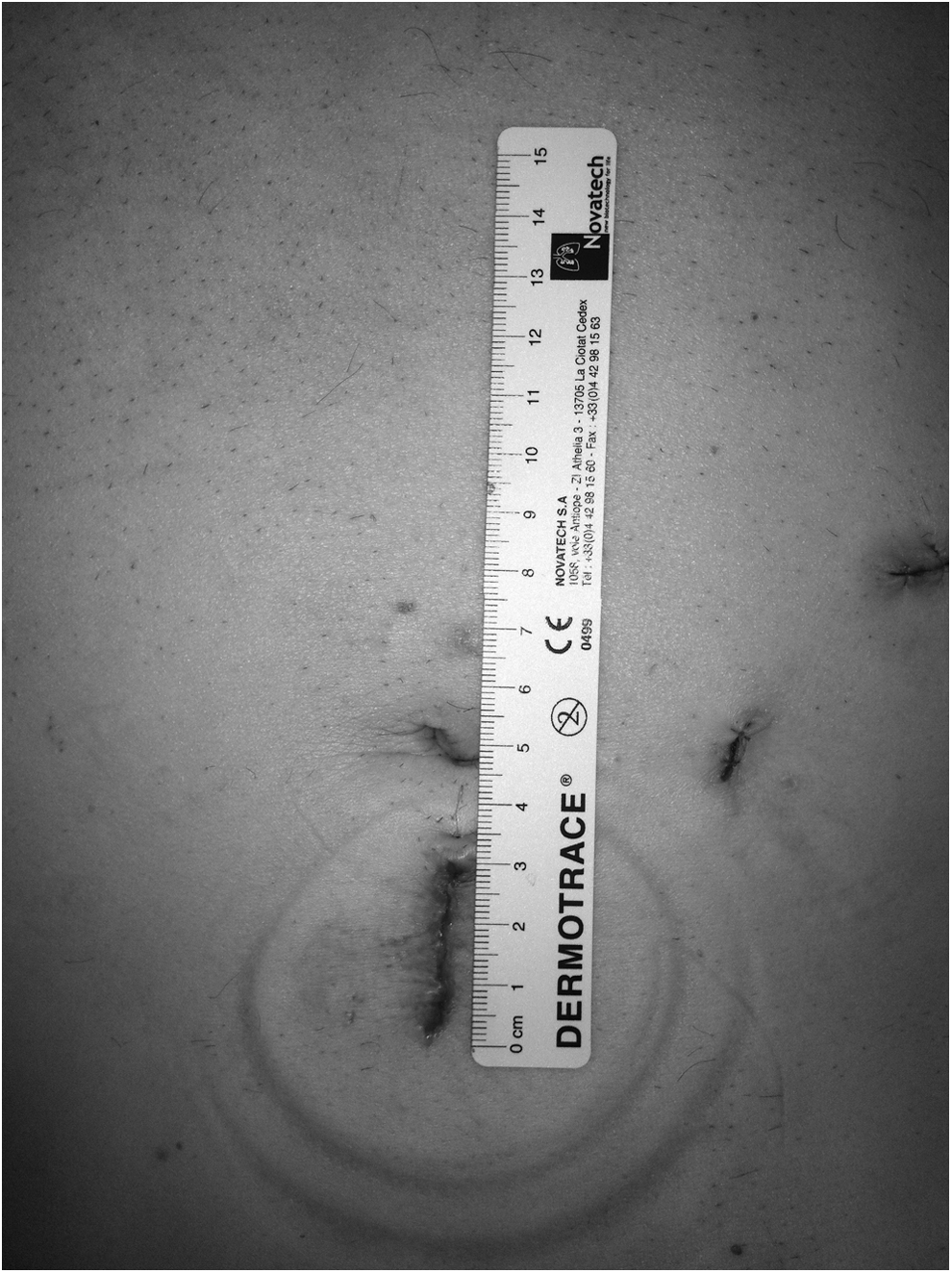
A 2–3-cm vertical midline supraumbilical skin incision.
Results
The study included 128 consecutive patients who underwent RALP using the ALEXIS port at our center (from April 2012 to September 2012).
The demographic details and perioperative data are given in Tables 1 and 2.
PSA=prostate-specific antigen; BMI=body mass index; pts=patients.
EBL=estimated blood loss; IH=incisional hernia.
The size of incision to insert the ALEXIS was correlated to the volume of the prostate gland. A 2–3-cm incision was satisfactory when the prostate gland was smaller than 70 g. Otherwise, a 3–4-cm incision was required if the prostate was larger than 70 g. No significant hematoma related to this trocar was noted. An analytical analysis of postoperative pain was not performed; however, no patient needed any opiate drugs and no discharge was conditioned by incisional pain.
A positive SM at final pathology was identified in 21 (16.4%) patients; and IFS demonstrated a positive SM in 24 patients (18.7%). After re-resection of neurovascular bundles and adjacent tissue, 14 (10.9%) patients were negative at the final margin status. The IFS was decisive to reduce the positive SM status in 10.9% of the patients, and 10 (7.8%) patients remained at positive SM at final pathology after re-resection. There was discrepancy between IFS and final pathology in 11 (8%) patients, with a negative SM at IFS and final pathology showing a positive SM.
All surgeries were successfully performed robotically and no conversion to conventional laparoscopic or open surgery was necessary.
Discussion
The ALEXIS port device has been described for laparoendoscopic single-site surgeries (LESS). Series of robotic surgeries using a homemade single port with a wound retractor and surgical gloves have also been described in the literature. 17,18 We present the first series, to our knowledge, of RALP using ALEXIS.
IFS analysis of the whole neurovascular tissue-adjacent circumference can result in a significant increase of NS and a significant reduction of positive SM in RALP. Moreover, patients with a positive SM could be converted to a prognostic more favorable negative SM state by secondary resection of the ipsilateral neurovascular tissue. 11,12 We believe that the goal of IFS is to detect patients with no ECE on MRI, but presenting with a positive margin on IFS, enabling a posterior re-resection with a negative SM at final pathology. In our study, the IFS was decisive to reduce the positive SM status in 10.9% of patients. However, 7.8% of patients demonstrated a negative SM on IFS and a positive SM at final pathology. This discrepancy between IFS and final pathology probably can be caused by the technical difficulties and limitations of the analysis in the frozen section. Although we believe that IFS may improve the oncological prognosis according to margin status, the final pathology is still the gold standard for margin status analysis.
The surgical time may increase when regular robotic trocar is used because interruption of the robotic surgery and an extended incision is necessary to remove the specimen and then suture the wound to make it compliant to the optical trocar. We decided to use this trocar because it can provide easy and fast extraction of the specimen from the abdominal cavity. Even a larger prostate can be easily removed because the wound retractor acquires amplification of the incision diameter. No internal or external collision with the remaining robotic trocars was observed when using this device.
This trocar showed multiple advantages: (1) it is easy to use and can be simply accommodated to the abdominal wall even in overweight patients; (2) the wound retractor allows a very fast passage of the specimen through one small incision; (3) the two rings of the wound retractor can prevent subcutaneous emphysema, port-site infection, and bleeding 17,19,20 ; (4) the supraumbilical incision is minimized, with decreasing the postoperative pain and the rate of surgical site hernia development.
The perioperative results in the present study were comparable to those of RALP series with standard trocar placement. In terms of placement time and complications related to the ALEXIS, no difference was noted comparing to regular robotic umbilical trocar series in the literature. 7,21
Regarding costs, in our study, the Alexis system was not compared to any other method. However, the cost of the wound retractor plus an Applied™ trocar is less than the cost of several other 12-mm trocars from other manufacturers. We believe that using only the retractor and cap, with a regular robotic trocar, does not add a significant cost to the procedure. For this reason, Alexis can be very helpful when a fast removal of specimens for IFS is necessary without adding cost.
As minimally invasive procedures, robotic surgery demonstrates advantage in terms of aesthetic results comparing to open surgery. 22 One advantage of ALEXIS is to minimize the incision to extract the prostate than a regular RALP because of the amplification of the wound retractor. Even in obese patients, the wound retractor permits a smaller incision and a satisfactory trocar fixation. In our series, most patients (69.5%) were overweight and obese, and ALEXIS provides an easy insertion and fixation of the port device in this group. In most cases, a 2–3-cm incision was absolutely sufficient to extract the prostate. Schlomm et al. 11 related in a recent series of RALP an extended 3-cm umbilical incision as satisfactory to extract the prostate for IFS. Our patients were fully satisfied with the appearance of the scars. However, no questionnaire about aesthetic satisfaction was applied. The extraction of the surgical specimen through the supraumbilical incision allows for a better cosmetic result without an additional incision.
The incisional hernia (IH) rates after RALP is an important postoperative complication. 23 The rates and predisposing factors have not been well characterized. In several large RALP series, the IH rate was estimated at 0.2%–3%. 15,24 Fuller et al. 23 demonstrated in a cohort of prospective 250 RALP that closure of linea alba with a nonabsorbable suture using an interrupted technique may help to minimize the incidence of this morbid complication. Beck et al. 25 followed up 900 patients who had undergone RALP and noted that a greater body mass index (BMI) and a larger prostate size significantly increase the risk of hernia development. In addition, transverse incisions were related to a significant reduction rate of IH compared to vertical incisions. In our series, IH was observed in one patient (0.8%). This patient was not obese with BMI 20 and presented a fascial suture dehiscence in early postoperative time. Although our series has a short follow-up, the IH incidence may be underestimated. In case of vertical incision being more aesthetically acceptable by the patients, we believe that a vertical incision in the skin and a transverse incision in the fascia layers may contribute to reduce the incidence of IH.
In the present study, we have successfully shown that RALP using the ALEXIS port device is feasible and safe, and has provided acceptable operative outcomes and an alternative technique when IFS is indicated.
Footnotes
Disclosure Statement
No competing financial interests exist.