
Abstract
Purpose:
To assess the efficacy and safety of laparoendoscopic single-site adrenalectomy (LESS-A) and conventional laparoscopic adrenalectomy (LA) as a systematic review and meta-analysis of current evidence.
Methods:
We conducted a thorough search for comparative studies that compared LESS-A and conventional LA in the following databases: MEDLINE, EMBASE, and the Cochrane library. Studies were reviewed independently and rated by Newcastle-Ottawa Quality Assessment Scale. The operative time, estimated blood loss in operation, the time to resume oral intake after surgery, postoperative hospital stay, and the visual analog pain scale (VAPS) score were included for analysis to compare the efficacy, while the complications together with the analgesia use were included for analysis to compare the safety.
Results:
Nine studies with 171 LESS-A cases and 272 conventional LA cases were identified. Although operative time was longer in LESS-A (mean difference [MD] 15.46, 95% confidence interval [CI] 11.18 to 19.74), estimated blood loss (MD 4.72, 95% CI 12.08 to 21.52) and the time to resume oral intake (MD −0.04, 95% CI −0.19 to 0.11) were similar; LESS-A presented a shorter postoperative stay in hospital (MD −0.60, 95% CI −0.86 to −0.35) and lower VAPS score (MD −1.21, 95% CI −1.44 to −0.97). Besides, the risk of minor postoperative complications (risk ratio [RR] 1.74, 95% CI 0.78 to 3.87) was similar. The postoperative analgesia demand in total (RR 0.65, 95% CI 0.52 to 0.81) together with the analgesia usage lasting more than 24 hours after surgery (RR 0.35, 95% CI 0.21 to 0.58) were associated with lower risk in LESS-A, however.
Conclusions:
Based on current evidence, the operative time seems to be longer in LESS-A; however, operative blood loss and complications are similar. In addition, LESS-A presents a shorter hospital stay after surgery and more acceptable perception of pain than conventional LA.
Introduction
Although the randomized controlled trial (RCT) is considered to be the most rigorous assessment for comparing the outcomes of different medical interventions, it is too difficult and also very costly to set up a well-designed RCT with enough samples. 9 Several nonrandomized comparative series have been published in attempt to compare the outcomes of LESS-A with conventional LA in recent years; however, these results are inconsistent and, furthermore, their reported patient samples are still not large. 7,8,10 –16 Therefore, it is still unclear whether LESS-A is a truly less invasive and more feasible minimally invasive approach compared with conventional LA.
Fortunately, to evaluate different surgical approaches, systematic reviews of well-designed comparative studies are also feasible, and meta-analysis could also present a qualitative analysis for included data; the combined results are similar to those of contemporaneous RCTs. 17 Thus, we performed a systematic review of current publicized studies to compare the perioperative outcomes of LESS-A and conventional LA to assess the efficacy and safety of the two procedures, to see whether one of the two procedures is superior, or whether they are similar. A meta-analysis would also be performed if the extracted resource could be analyzed.
Materials and Methods
Search strategy and study selection
We searched for published comparative studies that compared the outcomes of LESS-A and conventional LA up to October 31, 2012 in the following online databases: MEDLINE, EMBASE, and the Cochrane Central Search library. We retrieved citations using combinations of the medical subject heading (MeSH) terms “adrenalectomy,” “laparoscopy” for the MeSH search, and we also used the keywords “laparoscopy,” “adrenalectomy,” “single-site,” “single-incision,” and “mono-port” for the freedom search. Every possible combination was taken into consideration. Articles in languages other than English were also included if data were extractable. Case reports, meeting records, and review articles were all excluded. All studies included should contain the baseline characteristics of patients, and original data for dichotomous and continuous variables should be provided or calculable from the data source; simple abstracts without complete information were also excluded because the quality was difficult to assess. When patients' data were reported more than once by the same institution, the most informative and recent article was included in our analysis. Three individual researchers (QH, YG, and CS) identified all studies that appeared to fit the inclusion criteria for full review. Senior investigators (KX and GX) made the final decision regarding inclusion or exclusion of a study.
Data extraction and analysis
The study selection progress is shown in Figure 1. At last, nine studies were selected for meta-analysis. All studies included were nonrandomized observational studies, and all the demographic data and histopathologic data presented by these studies are listed in Table 1 and Table 2.
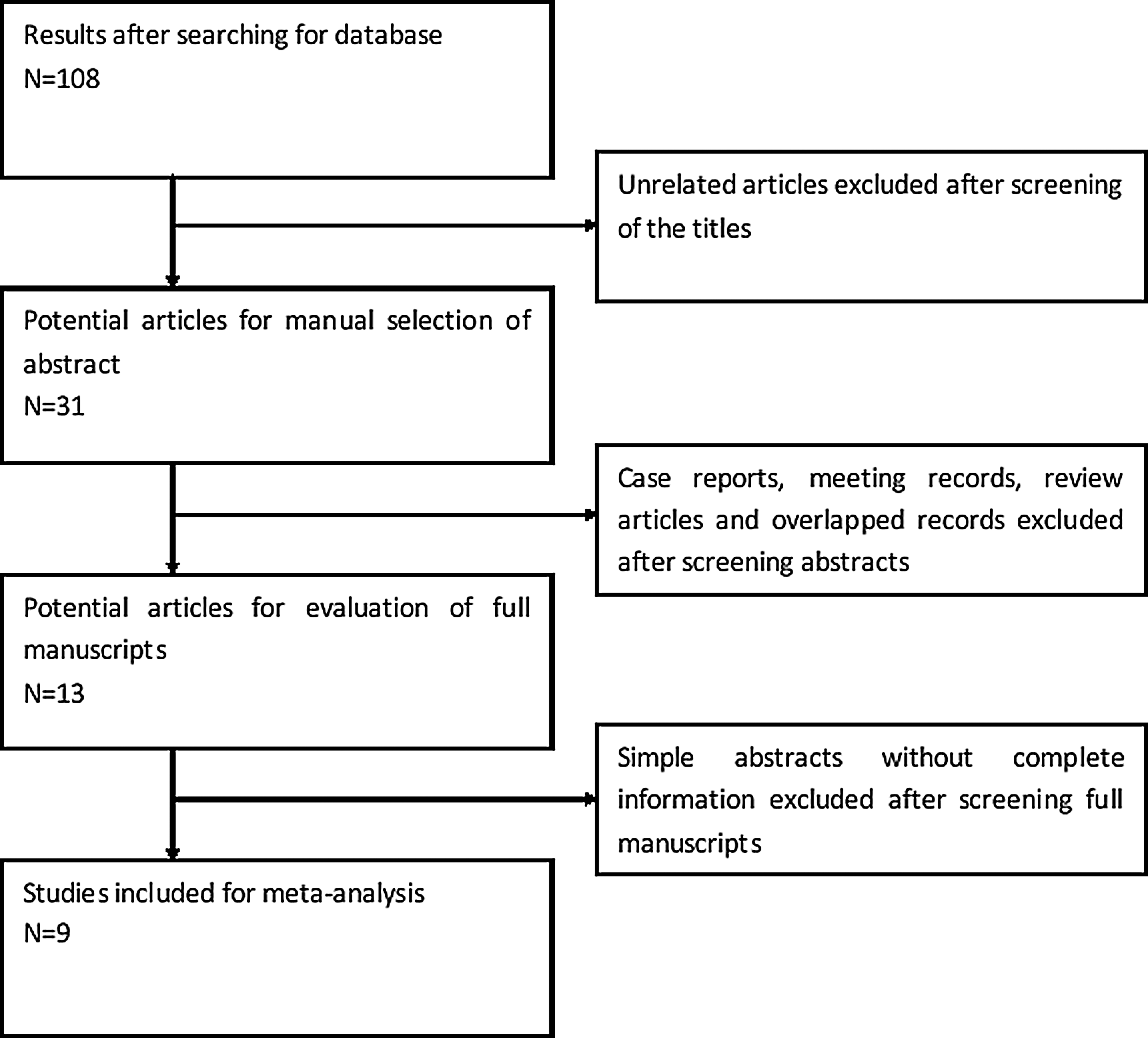
Flowchart of study selection.
LESS-A=laparoendoscopic single-site adrenalectomy; LA=laparoscopic adrenalectomy; BMI=body mass index; PAS=previous abdominal surgery; NR=not reported.
Significant difference exists
LESS-A=laparoendoscopic single-site adrenalectomy; LA=laparoscopic adrenalectomy; CS=Cushing syndrome; NR=not reported.
Reported as functional adenoma in total.
Medullary hyperplasia also included.
Cushing disease also included.
The primary objective of this review was to compare the efficacy of LESS-A and conventional LA; specific outcomes included were operative time, estimated blood loss in operation, the time to resume oral intake after surgery, postoperative hospital stay, and the visual analog pain scale (VAPS) score for assessing the perception of pain. Our secondary objective was to compare the safety of the two different laparoscopic procedures, and the complication materials were included for analysis. The complications were divided as intraoperative complications and postoperative complications, and the latter also contained minor and major complications that were classified according to the Clavien-Dindo classification system. 18 In addition, the analgesia use after surgery and the analgesia demand lasting over 24 hours were also reviewed as an aspect of safety.
For dichotomous parameters, such as complications and analgesia demand, the risk ratio (RR) was determined along with the corresponding 95% confidence interval (CI), and the Mantel-Haenszel fixed model was used for meta-analysis. 19 Heterogeneity between studies was measured by Cochrane chi-square test and also quantified with I 2 metric. The scale of I 2 ranges from 0 to 100%, with a higher value denoting a greater degree of heterogeneity. The Begg funnel plots were conducted to identify potential publication bias, and an asymmetric plot suggested a possible publication bias. If publication bias existed, then meta-analysis would be abandoned.
Continuous parameters, such as operative time, blood loss, oral intake restarting, postoperative hospital stay, and VAPS score for pain assessment, were compared with a parameter of mean difference (MD), and the Inverse-Variance fixed model was used for meta-analysis. 20 Similar to dichotomous variables, heterogeneity and publication bias were also tested. All data were extracted according to Cochrane Handbook (V 5.1.0), and Review Manager (RevMan 5.0.24) was used for all analyses. 21 All statistical tests performed were two-sided and declared at a P=0.05 significant level.
Assessment of quality and level of evidence
All studies included were nonrandomized, and none was a RCT. According to The Oxford 2011 Levels of Evidence, all studies included could be considered as a level of evidence at 3. 22 We used the Newcastle-Ottawa Quality Assessment Scale for cohort studies to assess the quality of studies. 23 This scale contains eight items, categorized into three dimensions including selection, comparability, and outcome. A maximum of one star could be awarded for each item, while the item of comparability allows two stars. The total score ranges from 0 to 9, with a higher score in a higher quality study; the assessment of included studies is shown in Table 3.

Results
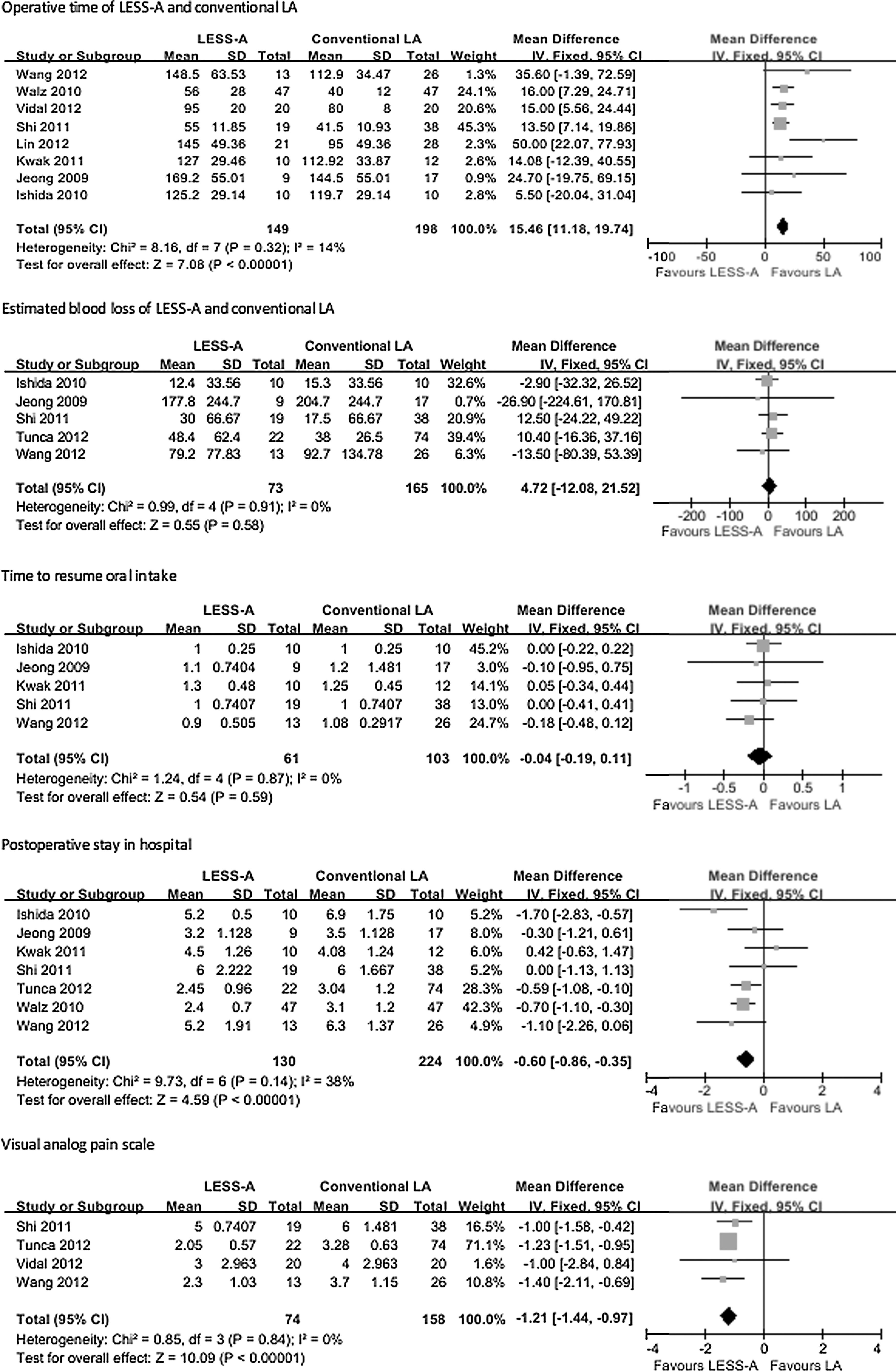
The primary objective was to compare the efficacy of the two laparoscopic procedures; no heterogeneity or publication bias was found between studies, and the Mantel-Haenszel fixed model was used. Although the operative time of LESS-A was significantly longer than that of conventional LA (MD 15.46, 95% CI 11.18 to 19.74, P<0.00001), the postoperative hospital stay after surgery was significantly shorter in LESS-A compared with conventional LA (MD −0.60, 95% CI −0.86 to −0.35, P<0.00001), and the VAPS of LESS-A was also lower (MD −1.21, 95% CI −1.44 to −0.97). Neither the estimated blood loss in operation (MD 4.72, 95% CI −12.08 to 21.52, P=0.58) nor the time to resume oral intake after surgery (MD −0.04, 95% CI −0.19 to 0.11, P=0.59), however, were shown to have significant differences between the two groups.
The secondary objective was to compare the safety of LESS-A and conventional LA. There were few intraoperative complications and major postoperative complications over grade III based on the Clavien-Dindo classification system, so meta-analysis was abandoned. Only minor postoperative complications as well as the analgesia usage after surgery and the analgesia demand lasting over 24 hours were included for analysis. Similarly, no heterogeneity or publication bias was found between studies, and the Inverse-Variance fixed model was used. There was no significant difference about minor postoperative complications between LESS-A and conventional LA (RR 1.74, 95% CI 0.78 to 3.87, P=0.18); however, the analgesia use after surgery (RR 0.65, 95% CI 0.52 to 0.81, P=0.0001) and the analgesia demand lasting over 24 hours (RR 0.35, 95% CI 0.21 to 0.58, P<0.0001) were both shown to have a significantly lower risk associated with LESS-A.
All results of meta-analysis are presented as forest plots with Tables 4 and 5, individually.

Discussion
Laparoscopy brings an enormous revolution of ideas and technique to surgical practice, particularly in the realm of urology, and adrenalectomy acts as one of the most successful illustrations of laparoscopy. 24 Recently, the development of laparoscopy has led to several novel laparoscopic techniques, such as LESS. 25 As a novel treatment for adrenal lesions, potential improvements of LESS-A, including increased comfort, improved pain control, and quicker convalescence, attract more practice. 26 Current series, however, are all of small sample sizes of patients, and the results of comparison of LESS-A and conventional LA are still inconsistent. As a result, we present a systematic review and meta-analysis of current evidence of LESS-A and conventional LA to compare the safety and efficacy.
Previous studies have compared LESS with conventional laparoscopic surgery, also in urology, such as nephrectomy, which shares similar structure of dissection with adrenalectomy, and no significant advantage of LESS has been achieved. 27,28 Canes and colleagues 29 and Tugcu and coworkers 30 are of the opinion, however, that LESS surgery could bring about faster convalescence than conventional laparoscopic surgery. Based on our results, the operative time seems to be longer in LESS-A; this seems to be easily understood because of the much narrower space for operation, the inadequacy of exposure, and the interference of different instruments. 7 The estimated blood loss in operation and the time to resume oral intake, however, are similar in the two groups. In addition, the postoperative hospital stay after surgery is significantly shorter and the VAPS score is lower in LESS-A. At the least, we could believe that LESS-A is technically feasible and comparable to conventional LA, while the shorter postoperative hospital stay and the lower VAPS score are really inspiring, which may imply that LESS-A could give improved tolerance and increased acceptance.
As the clinical experience increases, adrenalectomy, especially LA as the gold standard surgical treatment for adrenalectomy, is a feasible and safe operation with a relatively low risk of complication. In our review, only a case with an intraoperative complication of bleeding from the splenic laceration in the study of Jeong and associates, 12 and two cases of hypocortisolism and one case of Addisonian crisis as major postoperative complications in the study of Walz and colleagues 13 are reported. Because there are few positive reports, meta-analyses were abandoned, while no significant difference was found between the two surgical procedures concerning these two kinds of complications in publicized studies.
The average rates of minor postoperative complications of LESS and conventional LA reported in studies included in our review are 5.8% (10/171) and 3.3% (9/272). Meta-analysis shows that the risk of minor postoperative complications, which are grade I or II according to Clavien-Dindo classification system, is similar, but the analgesia use after surgery together with the analgesia demand lasting over 24 hours are both lower in the LESS-A group. These all imply that LESS-A is safe and an alternative for conventional LA. Besides, although not of significant difference, most studies except Lin and coworkers 10 present a lower complication rate in LESS. Whether the overall complications together with the subgroup analyses are similar needs more RCTs with larger sample sizes of patients to confirm.
Although several operative variables are similar between LESS and conventional LA, we could still believe that LESS provides shorter postoperative hospital stays and lighter feeling of pain after surgery, which may be associated with fast convalescence; thus, LESS still has its distinctive advantage over conventional LA. There are still some limits in our analysis, however. First, all studies included in our review are nonrandomized observational studies, which could either exaggerate or underestimate any actual differences. 31 As a result, the quality of our review could be affected directly. Second, LESS-A is a more recent technique, and there is obviously increased time for each surgeon to grasp this surgery well compared with conventional LA; then, the effect of the learning curve is really a important factor.
Most studies are from high-volume centers where the LESS-A and conventional LA are performed in the same period; however, the quality of these studies with a historical control group is lower, which would naturally decrease the quality of our review.
Finally, our analyses lack for subgroup analyses, because we know different kinds of adrenomas could affect outcomes of operations affirmatively, although histopathological data showed no significant difference in each study. 32 We believe that more RCTs with larger sample sizes would give us a more robust comparison.
Conclusions
Based on current evidence, operative blood loss and complications are similar in LESS-A and conventional LA; however, LESS-A presents faster convalescence after surgery and a more acceptable perception of pain than conventional LA.
Footnotes
Disclosure Statement
No competing financial interests exist.