
Abstract
Background and Purpose:
Radiofrequency ablation (RFA) has been considered as an important therapy for small renal lesions. The main limitation of RFA, however, is the lack of pathologic confirmation of complete tumor eradication. A single center, open label, randomized pilot study was designed to evaluate whether contrast-enhanced ultrasonography (CEUS) with Sonovue, performed in real time could allow us to determine the end point during laparoscopic radiofrequency ablation (LRFA) and the clinical outcome of this method.
Patients and Methods:
Ninety-six patients undergoing LRFA were randomly assigned to CEUS or a control group; finally, 38 and 40 patients with a pathologic diagnosis of renal-cell carcinoma completed a 3-month follow-up. CEUS was conducted in real time during the procedure to determine the end point in the CEUS group. The primary outcome was the incomplete ablation rate according to a radiographic image at 3 months after the procedure. The secondary outcome included the local tumor control rate and disease-free survival rate.
Results:
There were no differences in the incomplete ablation rate and disease-free survival rate between the two groups. Within a median 16-month follow-up period, three incomplete ablations and two local recurrences according to a radiographic image were found in the control group. Meanwhile, there was no incomplete ablation or recurrence but one lung metastasis in the CEUS group. The local tumor control rate was 87.5% (35/40) in the control group vs 100% (38/38) (P=0.073) in the CEUS group.
Conclusion:
In patients undergoing LRFA, there were no differences in the incomplete ablation rate and local tumor control rate between the CEUS group and the control group in our study despite a nonsignificant trend in favor of CEUS. CEUS may have the potential to provide more effective renal tumor ablation. These novel data support the need for a larger study of CEUS during LRFA surgery.
Introduction
The main limitation of RFA is that pathologic confirmation of complete tumor eradication is lacking. Although the radiofrequency (RF) systems provide impedence or temperature feedback, they are not always accurate. Instead, the adequacy of ablation is confirmed by the absence of enhancement on follow-up imaging. 6 The most accurate assessment of therapeutic response of RFA is mostly thought to rely on CT after RFA on follow-up. 7,8 Any lesion that enhances more than 10 Hounsfield units (HU) on contrast-enhanced CT imaging is considered to be untreated RCC and re-treatment is needed. 9
Therefore, a critical technical challenge in all ablation therapy for renal tumors is to find a method to monitor the completeness and precision of the ablation zone. Effective real-time imaging would provide valuable information about whether the entire tumor was ablated at the time of the procedure, thus potentially improving success rates of RFA and decreasing the need for additional surgery.
Although CT can be used to guide the procedure, real-time monitoring is not possible with CT imaging. The reason is that additional contrast agent cannot always be given because of toxicity limitations, and also this technique involves significant radiation exposure when CT is used. MRI can be used instead of CT, but the chief limitations are the cost and use of nonmagnetic instruments, as well as special shielding. On the other hand, although conventional gray-scale ultrasonography has become extremely useful for directing real-time placement of RF electrodes, it cannot provide enough information on the degree of tumor necrosis after RFA, and it has been proved to be unreliable when used during RFA as a means of measuring the zone of coagulation necrosis. 8,10
Contrast-enhanced ultrasonography (CEUS) using Sonovue is able to detect blood flow through small vessels. 11 Contrast ultrasonography has been described as a useful adjunct in diagnosing focal lesions and assessing treatment efficacy, especially for tumors of the liver and kidney. 12,13
Previous studies reported that monitoring renal RF lesions using CEUS in real time achieved success in a porcine model. 14,15 The aim of the present study is to assess whether CEUS is effective in determining the end point during LRFA.
Patients and Methods
Consecutive eligible patients were recruited for this randomized, open-labeled, prospective, clinical trial from March 2008 to June 2012 in our institution. Patients with newly diagnosed renal tumor were included in this study if one of the following criteria was met: Chronic renal insufficiency, presence of solitary kidney, advanced age (≤85 years), significant medical comorbidity, bilateral renal carcinoma, refusal of conventional therapy. Exclusion criteria included the following: Patients not able to tolerate the laparoscopic procedure, patients with previous renal surgery or history of any inflammatory conditions of the operative kidney, patients not able to accept long follow-up, patient refusal of this new kind of procedure.
Preoperative contrast-enhanced CT for tumors was performed. Patients with renal insufficiency or contrast agent allergy underwent gadolinium-enhanced MRI. The study protocol was approved by the Institutional Ethics Committee. Written, voluntary, informed consent was taken from all the patients.
All of these patients were randomly assigned, using a computer-generated, random-sequence grid maintained by the principal investigator, to two treatment groups in a 1:1 ratio: CEUS group or control group that used a combination of ultrasonography and laparoscopic visualization to determine the end point during laparoscopic RFA (LRFA).
There were 107 patients who were assessed for eligibility, of whom 96 were actually recruited and randomly assigned to the CEUS group (n=48) or the control group (n=48). Finally, 78 patients with a pathologic diagnosis of renal-cell carcinoma (RCC) completed a 3-month follow-up (Fig. 1).
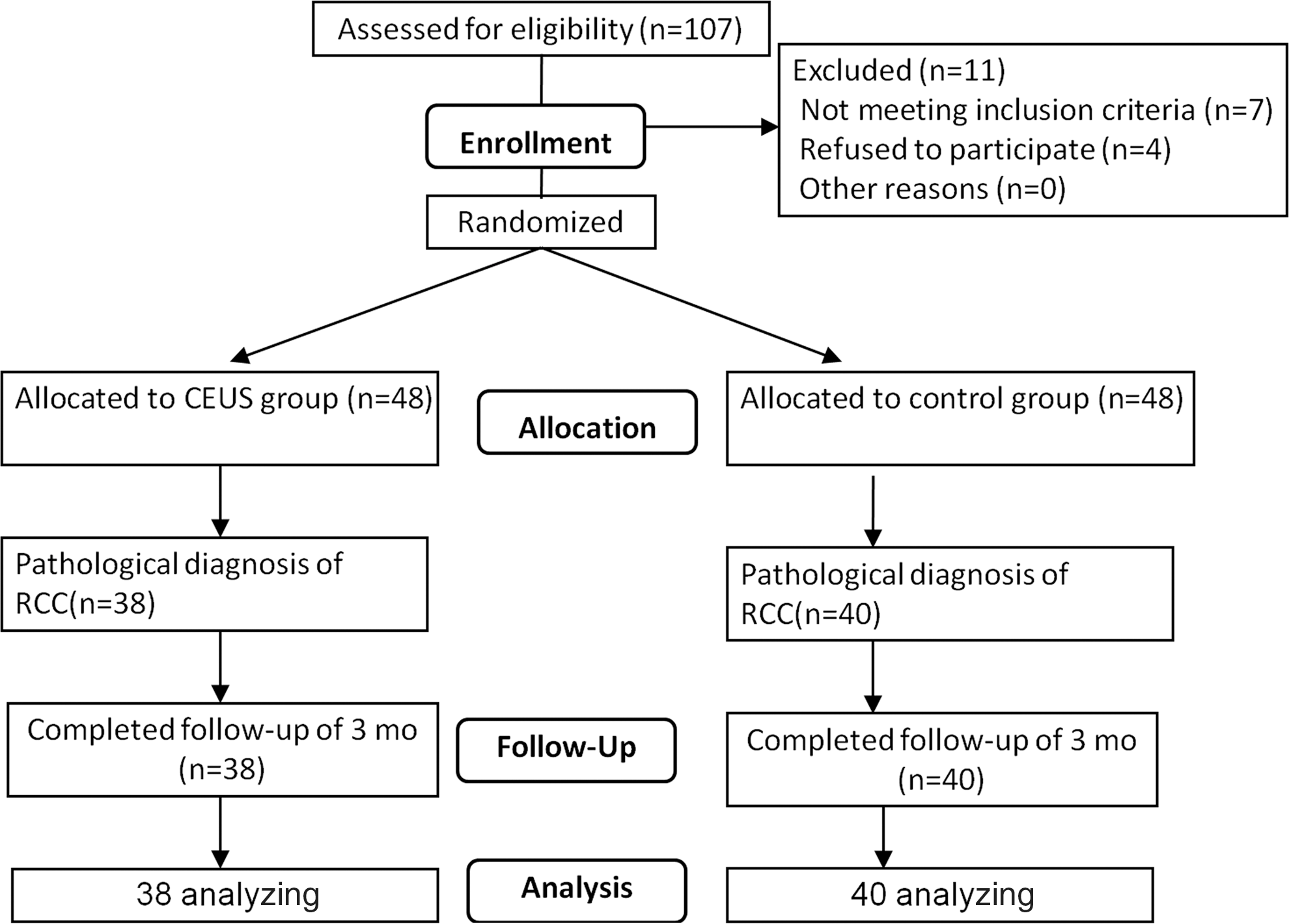
Consolidated standards for reporting trials diagram.
The tumor growth pattern data were also evaluated. Endophytic tumors were defined as demonstrating at least 60% of tumor volume contained within the renal parenchyma. Centrally located and parahilar tumors were classified as endophytic for analysis. Exophytic tumors demonstrated greater than 60% of tumor volume protruding beyond the renal capsule contour, and mesophytic tumors had approximately equal distribution of exophytic and endophytic components. 10
RFA
A transretroperitoneal or transperitoneal approach was used in each cases. After locating the tumor according to the preoperational CT or MRI image, the perinephric fat was reflected off the renal surface to identify the tumor with intraoperative ultrasonography, and then the kidney was manipulated so that the probe entered the lesion at a proper-angle so that the lesion could be ablated in minimum cycles. A cool-tip RFA system (Valleylab, Boulder, CO) with impedance-controlled pulse current from a 200 W generator was used for ablation. The electrode was kept at 15° to 20°C by means of internal cooling with chilled water delivered from a peristaltic pump.
RFA was performed for a cycle of 12 minutes per lesion according to the manufacturer's recommendations. The criteria of incomplete ablation of the CEUS group was the presence of residual enhancement within the treated lesion. Extra cycles were applied at the surgeon's discretion if ablation was considered incomplete on visual evaluation in the control group, and in the CEUS group according to the criteria. Then, the tumors were biopsied using laparoscopic scissors after ablation for histopathology examination. 16 Patients were blinded to treatment allocation.
The choice of a single (2- or 3-cm active tip) or cluster (three-prong, 2.5 cm active tip) needle electrode depended on tumor size and location of the lesion. Overlapping ablations were performed by repositioning the electrode to ablate the entire tumor.
CEUS
Within the whole study, the evaluation and precise localization of the lesions to be treated were performed by using the Pro Focus 2202 ultrasonography device (BK, Denmark) with real-time gray-scale contrast tuned imaging. Probe 8666-Rf was chosen for CEUS examination, using 4.5–7.5 MHz, with the mechanical index to be 0.18. During the procedure, the probe was placed on the surface of the tumor. If the intraoperative ultrasonographic image was not clear enough, water would be used as medical ultrasonic couplant. A dose of 2.4 mL of ultrasonic contrast agent in the form of microbubbles (SonoVue, Bracco, Milan, Italy) was injected intravenously as a rapid bolus, through an 18-gauge catheter placed in an antecubital vein, followed by a 5-mL saline flush. All CEUS examinations were recorded on a hard disk system.
The study protocol involved CEUS before and immediately after the ablation therapy was performed by the same operator (by LX). The second CEUS was performed when clinicians determined that the adequacy of ablation was enough to cover the entire tumor using conventional gray-scale ultrasonography. Successful treatment was defined when no focal and/or irregular enhancement within the treated lesion during the dynamic study was detected, whereas treatment failure was defined by the presence of residual enhancement within the treated lesion. Additional ablation would be added under this condition.
Follow-up and outcome measures
Contrast-enhanced CT or gadolinium-enhanced MRI was performed at 1 month, 3 months, 6 months postoperatively and every 6 months thereafter. Any lesion that enhanced more than 10 HU after contrast material administration or enhancement after intravenous gadolinium on contrast-enhanced MRI in 1 and 3 months postopratively was considered to be incomplete ablation. Recurrence was defined as any new enhancement (10 HU) after a nonenhancing scan after 3 months. At regular intervals, patients were reevaluated with contrast-enhanced CT or MRI in addition to a complete serum metabolic panel evaluation and chest radiography. The length of time, measured in months, from the procedure to the most recent follow-up scan, was recorded.
The primary outcome was the incomplete ablation rate according to radiographic image at 3-months after the procedure. The secondary outcome included the local tumor control rate and disease-free survival rate.
Data analysis
For continuous variables, the Student t test was used for those variables reported as mean (plus or minus standard deviation) and the Wilcoxon rank-sum test for the variables reported as median with interquartile ranges. For categorical variables, the chi-square test and the Fisher exact test were used. Differences were considered to be statistically significant if P<0.05. Statistical analysis was performed using SPSS, version 18.0 (SPSS, Chicago, IL).
Results
Table 1 shows baseline characteristics. There was no difference in the details of demographic and perioperative data between patients in both treatment groups. In all 96 patients, 78 (81.3%) had RCC, 14 (14.6%) had angiomyolipoma, one (1.0%) had oncocytoma, and 3 (3.1%) did not have a diagnosis.
CEUS=contrast-enhanced ultrasonography; SD=standard deviation; BMI=body mass index; ASA=American Society of Anesthesiologists.
During the procedure, in the CEUS group, the second CEUS in real time after the RFA session identified the absence of focal enhancement in 44/48 patients (Fig. 2) and the presence of residual enhancement at the ablated area suggestive for residual tumor in 4/48 patients (Fig. 3). These four patients received an additional ablation after the monitoring of CEUS in real time because of residual tumor. Of these four tumors, two were ≥4 cm and two were between 3.5 cm and 4 cm; three were of the endophytic growth pattern. Among these four patients, one patient was a 79-year-old man with high comorbidity who had a 6.0 cm tumor in the left kidney. The finding on the pathological examination was oncocytoma. There were no adverse events observed in the CEUS group.
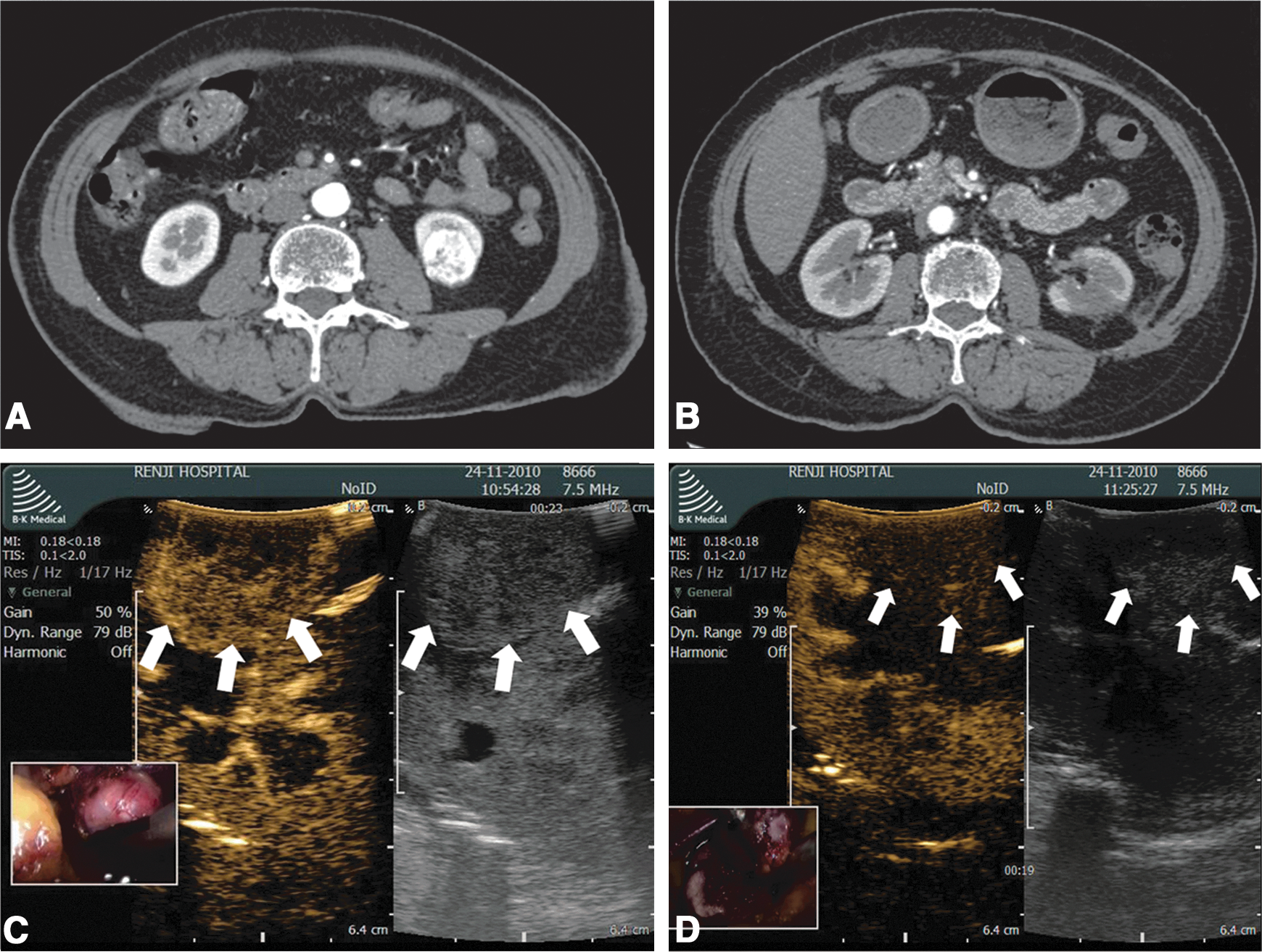
A 70-year-old woman with renal-cell carcinoma (RCC) in the left kidney.
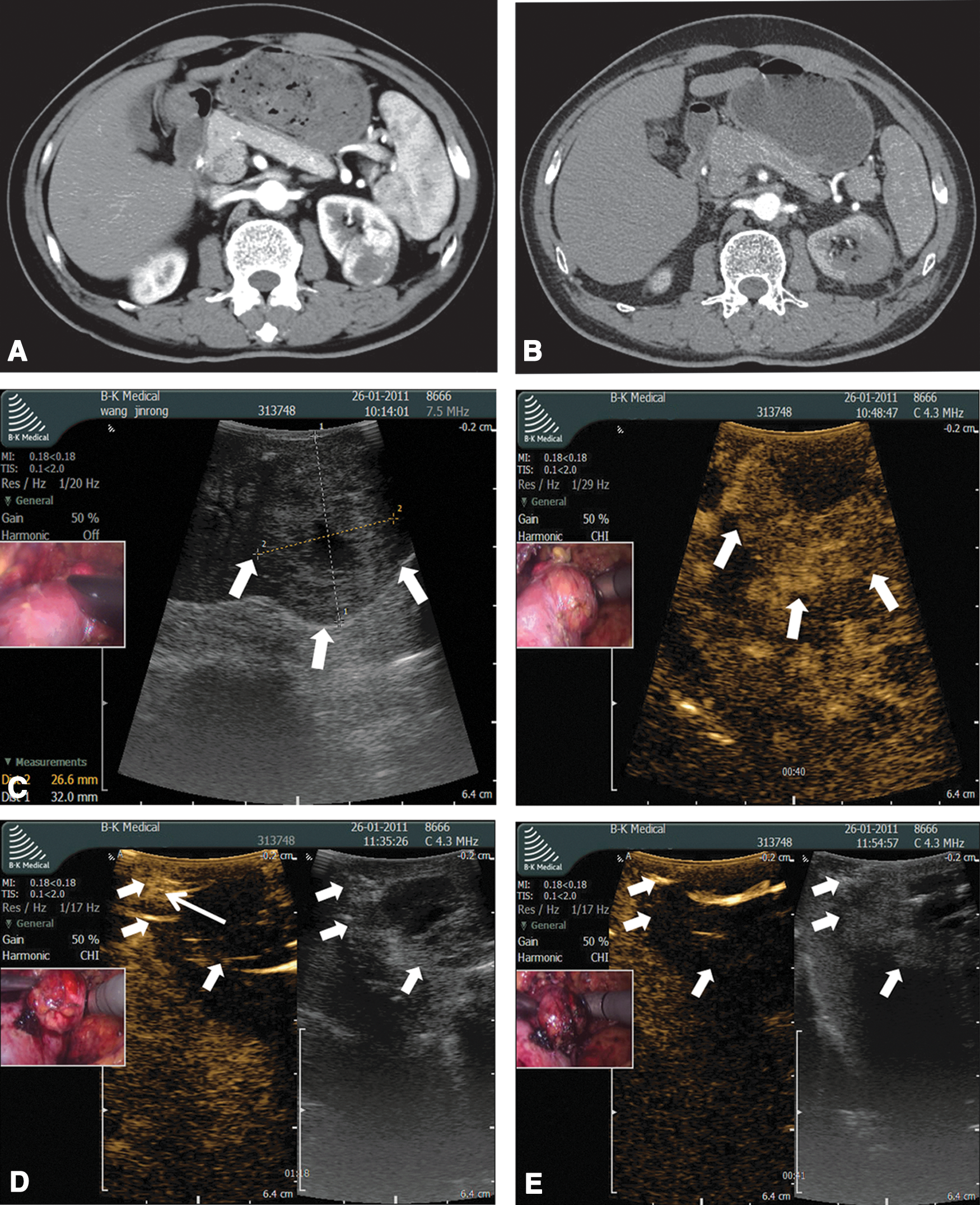
A 69-year-old man with RCC in the left kidney.
Follow-up
There were 78 patients with a pathologic diagnosis of RCC who completed 3-month follow-up. There were no statistical differences in the incomplete ablation rate between the two groups according to the 3-month radiographic image (Table 2). Thirty-eight patients had successful ablation in the CEUS group (n=38), while 37 patients had successful ablation in the control group (n=40). In three patients, residual enhancement at the margin was found on CT examination in 1-month and 3-months after LRFA (Table 3). One patient chose to receive additional radical nephrectomy 1 month later, and surgical pathology results revealed residual clear-cell RCC. The other two patients of advanced age chose active surveillance without further intervention, and during the following 36 and 12 months, both of them exhibited no tumor growth and were free of metastatic disease.
Fisher exact test.
CEUS=contrast-enhanced ultrasonography; SD=standard deviation.
ASA=American Society of Anesthesiologists; OPN=open partial nephrectomy; RN=radical nephrectomy.
Within the median 16-month follow-up period, three incomplete ablations and two local recurrences according to the radiographic image were found in the control group. Meanwhile, there was no incomplete ablation or local recurrence but one lung metastasis in the CEUS group. The local tumor control rate was 87.5% (35/40) in the control group vs 100.0% (38/38) (P=0.073) in the CEUS group. The two patients with local recurrence in the control group all chose open partial nephrectomy. One patient was confirmed with recurrent disease and the other showed no cancer cells. Both of them remained with no evidence of recurrent disease at the following period.
The disease-free survival rate was 87.5% (35/40) in the control group vs 97.4% (37/38) (P=0.226) in the CEUS group. There were no significant differences in disease-free survival rates between the two groups.
All 78 patients survived in the follow-up phase that ranged from 3 to 54 months. One patient was lost to follow-up 24 months after the procedure in the CEUS group.
Discussion
Our study demonstrated that with the help of real-time CEUS monitoring, four incomplete ablations were found (4/48, 8.3%) during procedure. In our series, there were no differences in the incomplete ablation rate and disease-free survival rate between the two groups. Within the median 16-month period (range: 3–54), three incomplete ablations and two local recurrences according to the radiographic image were found in the control group. Meanwhile, there was no incomplete ablation or recurrence but one lung metastasis in the CEUS group. The local tumor control rate was 87.5% (35/40) in the control group vs 100.0% (38/38) (P=0.073) in the CEUS group.
Advantages of CEUS in real time
Clinical success for the treatment of patients with RCC has been generally thought to be ablation of the entire tumor and surrounding tissue (security margin). Therefore, it is essential to assess the treatment effectiveness accurately and recognize residual lesion during RFA, especially for tumors of large size (>3 cm). Because the covered area of a single (2- or 3-cm active tip) or cluster (three-prong, 2.5 cm active tip) needle electrode is limited, overlapping ablations are needed when the size of the tumor is more than 3 cm. In our study, we chose CEUS as our real-time monitoring method.
Ultrasonography enhanced by gas-filled microbubble contrast agents allows depiction of regions of tissue perfusion and has been described as a useful adjunct in diagnosing renal pseudotumors, 17 confirming successful ablation of liver tumors and evaluating therapeutic response on RCC treated by RFA. US contrast media are not nephrotoxic and can be used safely, even in patients with impaired renal function, so it can be administered multiple times to achieve optimal treatment guidance to assess treatment results and need for immediate re-treatment. 18,19 A previous study reported that monitoring of renal RFA lesions using CEUS in real time achieved success in a porcine model. 14 Slabaugh and associates 14 showed that CEUS measurements of RFA lesions in real time approximated that found on gross and microscopic measurements of tissue ablation (cell death). The good agreement between real-time CEUS and follow-up CT results in our series also suggested that the use of CEUS in real time could determine whether the lesion was completely ablated.
Follow-up results of RFA of renal tumors
Gervais and colleagues 20 reported a 90% percutaneous RFA success rate for 100 renal tumors at a 2.3-year follow-up, whereas only 75% were completely ablated during the initial treatment. Hegarty and coworkers 21 provided data on 82 patients who underwent percutaneous RFA at a median follow-up of 12 months; the recurrence-free rate was 88.9%. Ji and colleagues 22 reported the intermediate-term results of LRFA on 106 renal patients; there were one incomplete ablation and one local recurrence, and the local tumor control rate was 98.1% (104/106). Our control group showed a similar incomplete ablation rate and local tumor control rate. In our CEUS group, however, 100.0% patients had lesions completely ablated, and the local control rate was 100.0%. Therefore, our results may indicate that the use of CEUS may provide a new method that can potentially determine the end point of RFA.
Indications of CEUS in real time
As for tumors larger than 3 cm and of endophytic growth pattern, the incomplete rate of RFA increased significantly. Gervais and associates 20 reported series of RFA for renal tumors has shown a re-treatment rate as high as 44% for tumors between 3 and 5 cm in greatest diameter and concluded that both small size and noncentral location were independent predictors for complete ablation. Using intraoperative real-time temperature monitoring of the ablative process could help to determine treatment end points and decrease the incomplete ablation rate, even for tumors between 3 and 5 cm in greatest diameter and central renal tumors. 10,23
The main limitation of this method, however, is that the added information from several peripheral thermistors does not yield information about the entire periphery. Four in five patients with incomplete ablation or local recurrence in the control group in our study were larger than 3.5 cm and of endophytic pattern. According to previous study and our experiment, CEUS may potentially provide a new modality to best determine the end point of RFA, and indications of real-time CEUS during RFA may include tumor size larger than 3 cm and the endophytic tumors, which need overlapping ablations to cover.
Active surveillance
Abouassaly and coworkers 24 observed that during a median 24 months of active surveillance in 110 elderly patients with a diagnosis of enhancing renal masses (median age: 81 years; median Charlson Comorbidity Index: 2), no patients died of renal tumor, while 34 (31%) patients died because of other reasons, and 43% patients exhibited no tumor growth. Another study 25 showed similar results; in 212 patients with renal cortical neoplasms who underwent active surveillance (median age: 71 years; median Charlson Comorbidity Index: 3), only one (0.5%) cancer-related death was reported, but a total of 14 patients died of another medical condition during a median 35 months of follow-up. In our study, two elderly patients (aged 79 and 85 years) with incomplete ablation chose active surveillance, and both exhibited no tumor growth and were free of metastatic disease until now. Regarding previous research and our study, active surveillance for incomplete ablation and local recurrence of RFA appears to be a reasonable option for older patients with multiple medical comorbidities and a limited life expectancy.
Our findings are subject to the limitations of a single institution design. Moreover, because it was a small scale study, no statistical differences were obtained in this study. A larger scale clinical trial is really needed to draw a conclusion as to whether CEUS has an effect in decreasing the incomplete ablation rate and local tumor control rate.
Conclusion
In patients undergoing LRFA, there were no differences in the incomplete ablation rate and local tumor control rate between the CEUS group and the control group in our study despite a nonsignificant trend in favor of CEUS. CEUS may provide surgeons the potential to decrease the incomplete ablation rate and to increase the local tumor control rate during LRFA. These novel data support the need for a larger study of CEUS during LRFA surgery.
Footnotes
Acknowledgments
The design and conduct of the project was supported in part by Award Number SHDC12010104 from Shanghai Hospital Development Center, by Award Number PWZxkq2010-03 from Bureau of Health of PuDong, by Award Number 81072097 from National Natural Science Foundation of China.
Disclosure Statement
No competing financial interests exist.