
Abstract
Purpose:
To assess the incidence of difficulty in complete dissection between the right adrenal gland and the liver at the time of laparoscopic surgery for adrenal tumor and to elucidate its cause histopathologically.
Patients and Methods:
Thirty-six patients underwent laparoscopic right adrenalectomy between 2004 and 2011 at our institution. Two reviewers independently assessed difficulty in dissection for the 36 nonedited video records of laparoscopic right adrenalectomy in blinded fashion. Twenty-seven records were evaluable for the judgment of difficulty in dissection between the lower surface of the liver and the right adrenal gland. On the other hand, the gross and microscopic relationship between the right adrenal gland and the surface of the liver was investigated in 32 cadavers.
Results:
Incomplete resection of the adrenal gland was found in 11 of 27 (40.7%) patients. Difficulties in dissection because of adhesions between the liver and the adrenal gland were apparently recognized in 5 of 27 (18.5%) patients. Pathologic assessment for cadavers revealed that capsules between these two organs are partially fused in 10 of 32 (31.3%) cases. Histopathologically, intermingling of parenchymal cells (infiltration through the fibrous capsules) was observed in nine (28.1%) cases.
Conclusions:
The tight adhesion between the lower surface of the liver and the adrenal gland because of intermingling of parenchymal cells of both organs is a major cause of incomplete resection of right adrenalectomy. Surgeons have to keep this fact in mind during right adrenalectomy to avoid unnecessary adverse events.
Introduction
The difficulty in dissection between the right adrenal gland and the liver has long been recognized as adrenohepatic fusion (AHF) by hepatic surgeons. AHF had been considered to be a very rare condition, however, until Honma 1 estimated in 1991 the prevalence of AHF to be 10% based on an autopsy investigation. From the current laparoscopic surgeons' point of view, this estimation seems still lower than it actually is. Once we encounter AHF, adrenal laceration or hepatic injury followed by massive bleeding might occur.
The aim of this study is to assess the incidence of difficulty in dissection between the right adrenal gland and the liver during the operation and the contribution of AHF to this difficulty by both reviewing unrevised video records of the operation. The incidence and histopathology of AHF were also investigated in cadavers.
Patients and Methods
This study consists of two examinations. The first is a retrospective video evaluation of laparoscopic right adrenalectomies to assess the grade and frequency of difficulty in dissection. The second is a cadaveric examination (in different patients) of the plane between the liver and right adrenal gland to uncover underlying histopathologic mechanisms.
Video review
Seventy-nine patients underwent laparoscopic adrenalectomy for adrenal neoplasms between 2004 and 2011 at our institution. Affected glands were right in 36, left in 41, and bilateral in 2. All of these operations were performed by two expert operators who were certificated for urologic laparoscopic surgery by the Japanese Society of Endourology. Laparoscopic right adrenalectomies were performed by the transperitoneal anterior approach, which is described elsewhere. Vessel sealing devices (LigaSure™ blunt tip) is usually used for dissection around the adrenal gland. Two certified senior urologic surgeons who have more than 50 adrenalectomy experiences independently reviewed the 36 nonedited videos of laparoscopic right adrenalectomy in a blinded fashion. They reviewed nonedited videos all through the operative procedures.
Twenty-seven (75%) records (10 males, 17 females, mean age: 51.8 years) were evaluable for assessment of difficulty in dissection between the right adrenal gland and the liver. The difficulty of dissection includes laceration of the adrenal gland and tear of the adrenal gland or liver capsule during dissection between the two organs.
Patient age, sex, tumor location type, and pathologic features of the adrenal tumor are shown in Table 1. Tumor location types were classified into three types (Fig. 1). Tumors located in the upper pole, in the middle portion, and in the lower pole of the adrenal gland were defined as types 1 and 2, respectively. The type of multiple small tumors was classified as type 3. Pathologic features of the 27 tumors were nonfunctioning tumor (14 cases), pheochromocytoma (6 cases), primary aldosteronism (4 cases), Cushing syndrome (2 cases), and metastatic adrenal cancer (1 case), respectively.
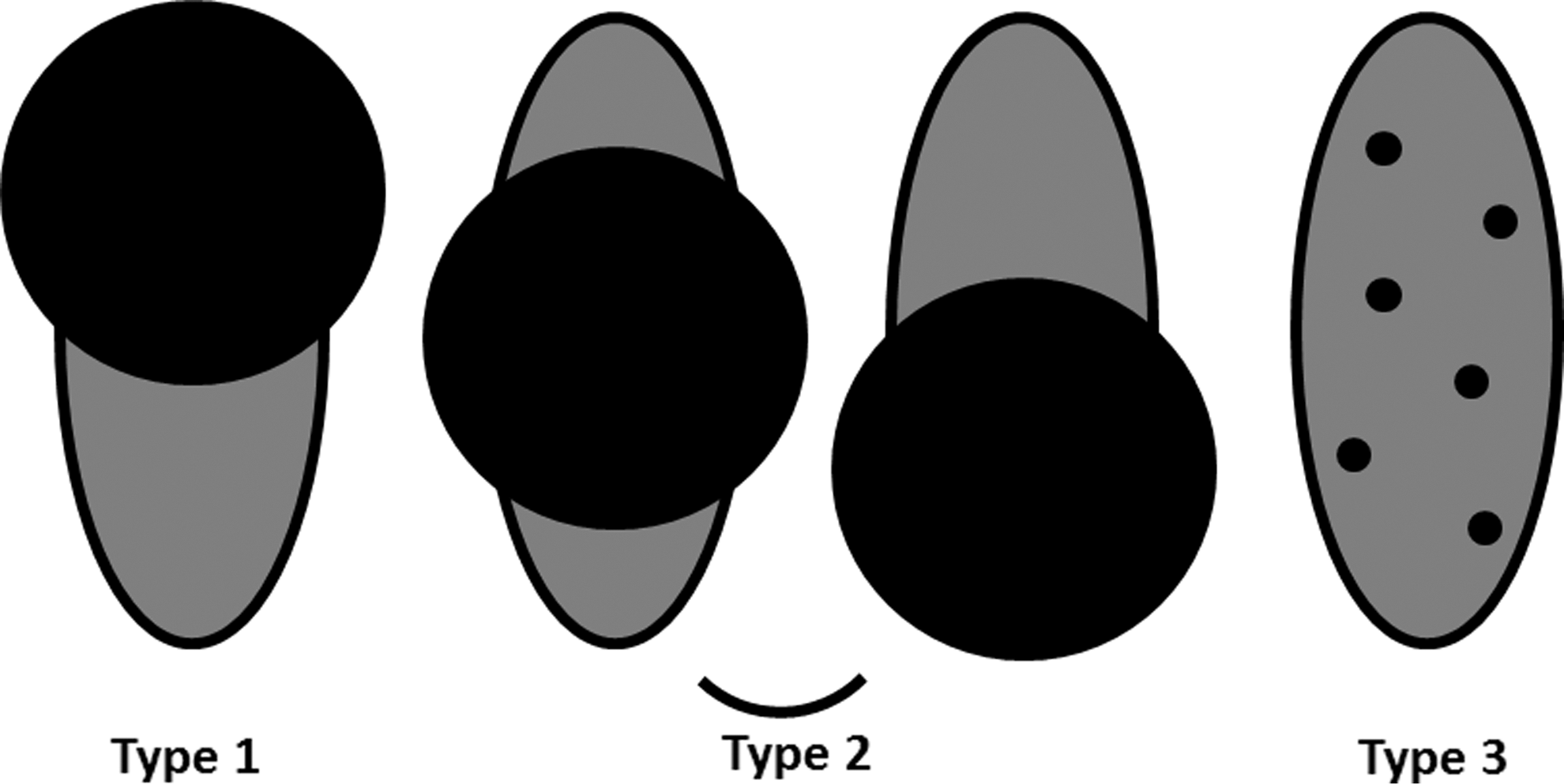
Types of tumor location. Adrenal tumor types were classified into three types according to location of the tumor in the adrenal gland: (1) Tumor in the upper pole; (2) tumor apart from the liver; (3) multiple small tumor foci.
AHD=adrenohepatic dissection; UC=uncountable split time.
Cadaveric examination
Gross and microscopic histologic relationship between the right adrenal gland and surface of the liver was pathologically investigated in 32 cadavers. Twenty-three were donated cadavers for medical education in Kagawa University, while 9 were autopsy bodies in an affiliated hospital and our institution (5 and 4 cases, respectively). This cadaveric study was approved by the Institutional Review Board of Kagawa University Faculty of Medicine (approved #H24-8).
Histopathologic analysis
Careful en bloc dissection of the right adrenal gland and right hepatic lobe of the cadavers was performed. After the formalin fixation, each specimen was cut in 4-mm thicknesses and embedded in paraffin block. Hematoxylin and eosin-stained glass slides were made routinely. The slides were examined by a pathologist (SS). To confirm intermingling of the parenchymal cells of the right adrenal gland and the liver, immunohistochemical (IHC) staining was also performed. The IHC staining was performed with the labeled streptavidin biotin method, using the auto staining system (Ventana XT system Benchmark, Roche Diagnostics Japan, Tokyo) and commercially available reagents (I-VIEWDAB universal kit, Roche Diagnostics Japan, Tokyo). Tested antibodies were CK7 (clone OV-TL12/30, mouse, monoclonal, Leica), CK AE1/AE3 (clone AE1/AE3, mouse, monoclonal, DAKO), synaptophysin (clone 27G12, mouse, monoclonal, Nichirei), chromogranin A (rabbit, polyclonal, DAKO), inhibin alpha (R1, mouse, monoclonal, DAKO), and hepatocyte (OCH1E5, mouse, monoclonal, DAKO).
Histologic AHF (hAHF) is histopathologically defined when the fibrous capsule between the liver and the right adrenal gland is partially fused or absent with intermingling of parenchymal cells. Distinguished from hAHF, histologic adrenohepatic adhesion (hAHA) is defined as tight fibrous capsule attachment between two organs without parenchymal cells intermingling. The hAHF was further classified into three subtypes as follows: Type a is extension of adrenocortical cells into the liver; type b is extension of hepatocytes and/or bile duct epithelial cells into the adrenal gland; and type c is bidirectional intermingling, as shown in Figure 2.
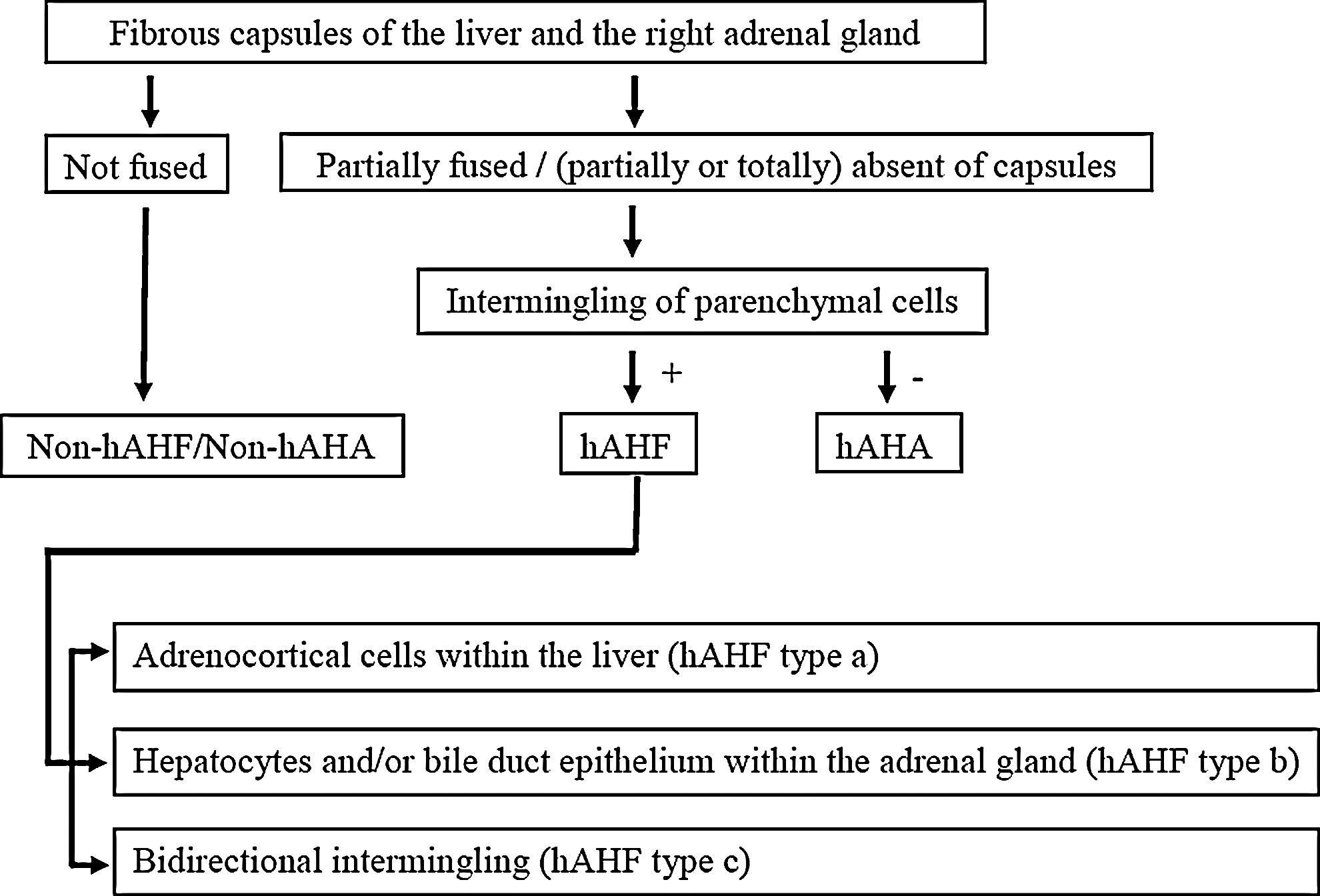
Schematic diagram for classification of adrenohepatic fusion subtypes. Histologic adrenohepatic fusion (hAHF) is histopathologically defined when the fibrous capsule between the liver and the right adrenal gland is partially fused or absent with intermingling of parenchymal cells. Distinguished from hAHF, histologic adrenohepatic adhesion (hAHA) is defined as tight fibrous capsule attachment between two organs without parenchymal cells intermingling.
Results
Adrenal laceration, difficulty in dissection
Judgment as to feasibility of adrenohepatic dissection by the two reviewers was identical except for one case in which one reviewer could not judge completeness of dissection. Consequently, incomplete resection associated with laceration of the right adrenal gland was recognized in 11of 27 (40.4%) operation records, although accurate judgment was impossible for one record as shown in Table 1. No hepatic parenchymal injury was observed in this series. Tumor location was type 2 in all of the 11 cases.
Difficulties in dissection because of adhesion were apparently recognized in 5 of 27 (18.5%) patients. All of the five cases were categorized into tumor location type 2 (Table 1). Laparoscopic right adrenalectomy was completed without measurable bleeding (<5 mL) in 11 (40.4%) patients, while a relatively large amount of bleeding (100 mL or more) was encountered in five (18.5%) patients. The median operative time was 215 minutes (range 100–449 min), the median amount of bleeding was 64 mL (range immeasurably small−400 mL). The large bleeding was observed in three of five cases in which adrenohepatic dissection was difficult.
There was no statistical association of total pneumoabdomen time or split time for adrenohepatic dissection with the presence or absence of adhesion, complete or incomplete resection, age, and sex. In addition, tumor size did not affect the difficulty of dissection (median tumor size (cm) with attachment (n=5) vs without (n=22): 3.4 vs 2.7, P=0.209).
Histopathology of hAHF/hAHA
Dissection of the right adrenal gland from the lower surface of the liver was feasible in about two-thirds of cadavers/autopsy bodies. Dissection, however, was sometimes difficult because of the tight attachment of the adrenal gland to the liver, as shown in Figure 3. Thorough histopathologic examination to clarify the anatomic relationship between the right adrenal gland and liver was performed in all cadaver/autopsy bodies. In 22 of 32 specimens, fibrous capsules of the liver and that of the right adrenal gland were not fused with each other microscopically. Between the liver capsule and the adrenal gland capsule, there was coarse fibrous tissue or adipose tissue (Fig. 4a). On the other hand, capsules between these two organs were partially fused in 10 of 32 cases (hAHA/hAHF). Moreover, intermingling of parenchymal cells (hAHF) was observed in nine (28.1%) cases (Figs. 4b–g and Table 2).

Gross appearance of coronal section in a patient with adrenohepatic fusion. Tight attachment between right adrenal gland and surface of liver was observed. Intermingling of parenchymal cells was microscopically confirmed. A=adrenal gland; L=liver; arrows=adrenohepatic fusion.
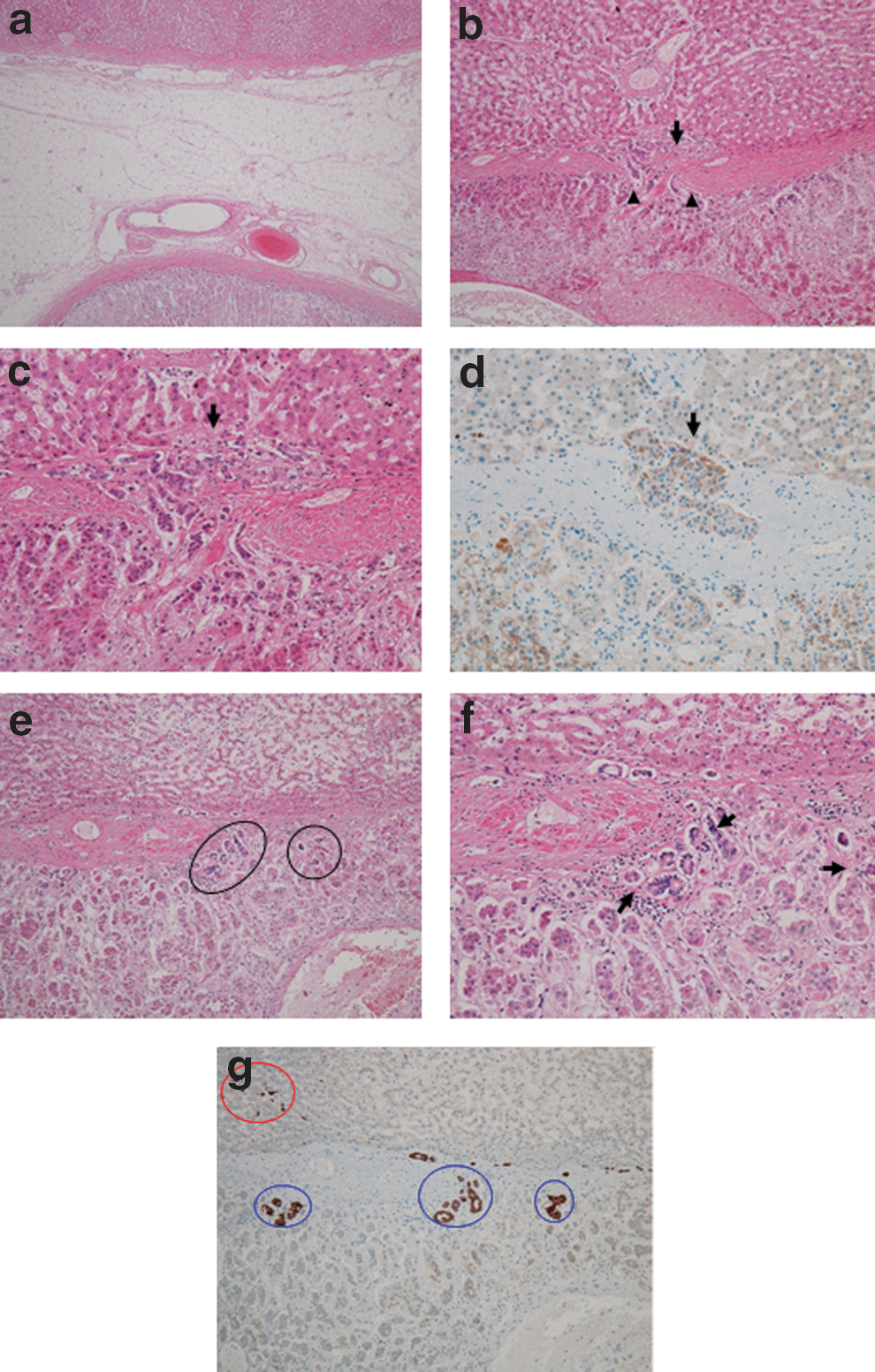
Histologic pattern of adrenohepatic fusion. (a) Nonhistologic adrenohepatic fusion/histologic adrenohepatic adhesion (hAHF/hAHA); each organ has a distinct fibrous capsule, and those capsules are not fused. Between them, there are adipose tissue and vessels. (b) hAHF type a; partial absence (between arrow heads) of the intervening fibrous capsule between the liver and the right adrenal gland; adrenocortical cells growing into liver tissue (arrow). (c) Higher magnification of b. Close contact (arrow) of the adrenocortical cells and hepatocytes is seen. (d) Inhibin alpha stain highlights adrenocortical cell nests (arrow) grow into liver tissue over the fibrous capsule. (e) hAHF type b; bile ducts (encircled) grow into adrenocortical tissue over the fibrous capsule. (f) Higher magnification of d. Close contact of bile ducts and adrenocortical cells (arrow) is seen. (g) Cytokeratin 7 highlights both bile ducts in liver tissue (red circle) and in adrenal cortex (blue circle).
Some cases of hAHF showed partial absence of fibrous capsule, and there was close contact between liver parenchymal cells and adrenocortical cells. Others showed that each parenchymal cell infiltratively extended into the other organ through the fibrous capsules without partial absence the capsule. As for the intermingling pattern, eight cases were type a, and only one case was type b. IHC stain confirmed intermingling of each parenchymal cells (Fig. 4d, g). No specific hepatic condition (ie, chronic hepatitis or cirrhosis) related hAHF/hAHA was observed in our cases.
Discussion
The present study clearly demonstrates that AHF is not so rare a condition as supposed in the past. Moreover, in most of the adhesive cases, fibrous capsules of both the liver and the adrenal gland were partially lacking, and the parenchymal cells were intermingling (hAHF). hAHF/hAHA is supposed to be the major cause of laceration/incomplete resection of the right adrenal gland during right adrenalectomy.
In 1968, from postmortem examination, AHF was detected in only in 3 of 115 (2.6%) consecutive procedures. 2 The incidence rate of AHF, however, seems to be higher than this postmortem examination. In 1991, Honma 1 reported that hAHF was found in 63 of 636 (9.9%) autopsy cadavers. The present study, analyzing both operative video records and cadaveric examination, further supports that AHF is not so rare a condition; moreover, its incidence is assumed to be higher than the Honma estimation.
The right adrenal gland is located beneath the “bare area” of the liver where hepatic parenchyma is not covered by the peritoneum. The present results indicate that the right adrenal gland is not infrequently adhesive to the lower surface of the liver. Surgeons, therefore, should pay special attention when dissecting the right adrenal gland from the liver, because injury of the adrenal gland often results in obstinate bleeding.
Interestingly, hepatocellular carcinoma (HCC) metastasizes to the right adrenal gland twice as frequent as to the left adrenal gland. 3 –5 Moreover, 5-year overall survival after adrenalectomy in patients with adrenal metastasis from HCC is reported to be 34%, 4 which is more favorable than that (24%) in patients with adrenal metastasis from other organs. 6 In particular, HCC patients who had only right adrenal metastasis showed better survival. 7 Metastasis of HCC to the right adrenal gland occurs via multifactorial processes. The present study, however, suggests that direct extension to the right adrenal is not an infrequent phenomenon. The better survival so far reported in HCC patients with right adrenal rather than left adrenal metastasis may be partly explained by the difference in the metastatic process.
The present histopathologic analysis indicates that there is no boundary between the liver and the right adrenal gland in up to 30% of persons. Rather, there exist mutual invaginations. Several cases in which intrahepatic or intermingling adrenocortical tumors at the bare area of the liver mimic hepatocellular carcinoma were reported. In such cases, it was difficult to diagnose preoperatively. 8,9
hAHF/hAHA, therefore, is defined as intimate attachment between the right adrenal gland and the liver in fusion or absence of distinct fibrous tissue separating the organs. hAHF can be discriminated from hAHA with existence of parenchymal cell intermingling between the two organs. From a surgical point of view, recognition of the existence of the “tight attachment” is the most important issue. The clinical impact of hAHF/hAHA, however, has neither been fully discussed nor paid special attention by surgeons.
During the adrenal operation, when we encounter difficulty in dissection between the right adrenal gland and the liver, the issue of hAHF/hAHA should be kept in mind. In the case of difficult dissection, further dissection should rather be avoided to prevent substantial sequels of massive bleeding or liver injury, because most adrenalectomies are, fortunately, conducted for nonmalignant tumors. In the present study, however, there was no statistical difference in the amount of bleeding and operative time. One possible explanation is that we did not complete the resection when we encountered persistent attachment between the adrenal gland and surface of the liver.
There are some limitations to this study. First, the number of patients in this study is relatively small for the accurate assessment of incidence. Second, because ages of our study participants were relatively high, the incidence of hAHF/hAHA in younger generation remains unclear.
Conclusions
The present study suggested that tight attachment between the lower surface of the liver and the right adrenal gland is not so rare a condition. Moreover, histopathologic investigation of the present study indicates that intermingling of parenchymal cells of each organ is the major cause of the tight attachment. Surgeons have to keep this issue in mind and pay careful attention during right adrenalectomy to avoid unnecessary adverse events.
Footnotes
Disclosure Statement
No competing financial interests exist.