
Abstract
Background and Purpose:
Percutaneous nephrolithotomy (PCNL) is the gold standard treatment for patients with renal stones larger than 2 cm. In this article, we aim to describe our modified technique with the patient in a complete supine position for PCNL (csPCNL).
Patients and Methods:
A total of 117 patients (120 renal units) who underwent csPCNL for large stones from November 2008 to November 2011 were prospectively evaluated. One surgeon worked in two different institutions and performed all operations. All patients underwent CT preoperatively, and the stones were classified according to the Guy score. Patients were placed in the supine decubitus position with the posterior axillary line located just outside the border of the surgical table, and the flank was extended to increase the space between the last rib and the iliac crest. The csPCNL was performed without a rolled towel under the flank, and the patients remained in the same position during the entire procedure. Success was evaluated based on CT findings at the end of follow-up.
Results:
There was no failure of access. The median operative time was 100 (20–240) minutes. The immediate and final success rates were 72.5% and 90.4%, respectively. The complication rate was 16.8% (12.7% of Clavien I or II and 4.1% of Clavien III or IV). There were no colon injuries or deaths. The median hospital stay was 48 (24–840) hours.
Conclusion:
Modified csPCNL is a safe and effective procedure with excellent outcomes and a low rate of major complications. It provides a good area for renal puncture and surgical instrumentation.
Introduction
Technical difficulties, such as a small area for renal puncture and difficulty with nephroscope manipulation, mainly to access the upper pole, have been related to the supine position. 9 Some modifications in patient positioning have been proposed to solve these difficulties and improve surgical outcomes and ergonomy. Different supine positions have been described, but few data regarding the benefits and disadvantages of these positions exist. 4,10,11 The best supine position is not well established and remains a subject of debate and study. 12
We aim to describe our modified technique, which was developed to overcome these difficulties related to traditional or modified Valdivia positions, 3,11 and to report our surgical outcomes.
Patients and Methods
Study population
A total of 117 consecutive patients (120 renal units) who underwent PCNL in a complete supine position (csPCNL) from November 2008 to November 2011 were prospectively evaluated. The procedure was explained to all patients who signed a consent form. The inclusion criteria were renal stones larger than 2 cm, multiple stones, or failure with other treatments. Exclusion criteria were age under 18 years, concomitant ureteral stones, or coagulopathies. One surgeon (FCV) working in two different institutions performed all surgeries using the same technique. The surgeon had previous experience with PCNL in the prone position and modified Valdivia PCNL 11 but had no previous training with csPCNL.
All patients underwent noncontrast CT preoperatively, and the stones were classified according to the Guy stone score 13 (Guy's I–30.8%, II–31.7%, III–22.5%, and IV–15%). Surgical complications were graded according to the modified Clavien score. 14 Preoperatively, all patients received a prophylactic third-generation cephalosporin during the anesthesia induction or therapeutic antibiotics according to urine culture initiated 7 days before surgery. Patients with staghorn stones started oral antibiotics 7 days before surgery, even with negative urine culture results.
Operative technique
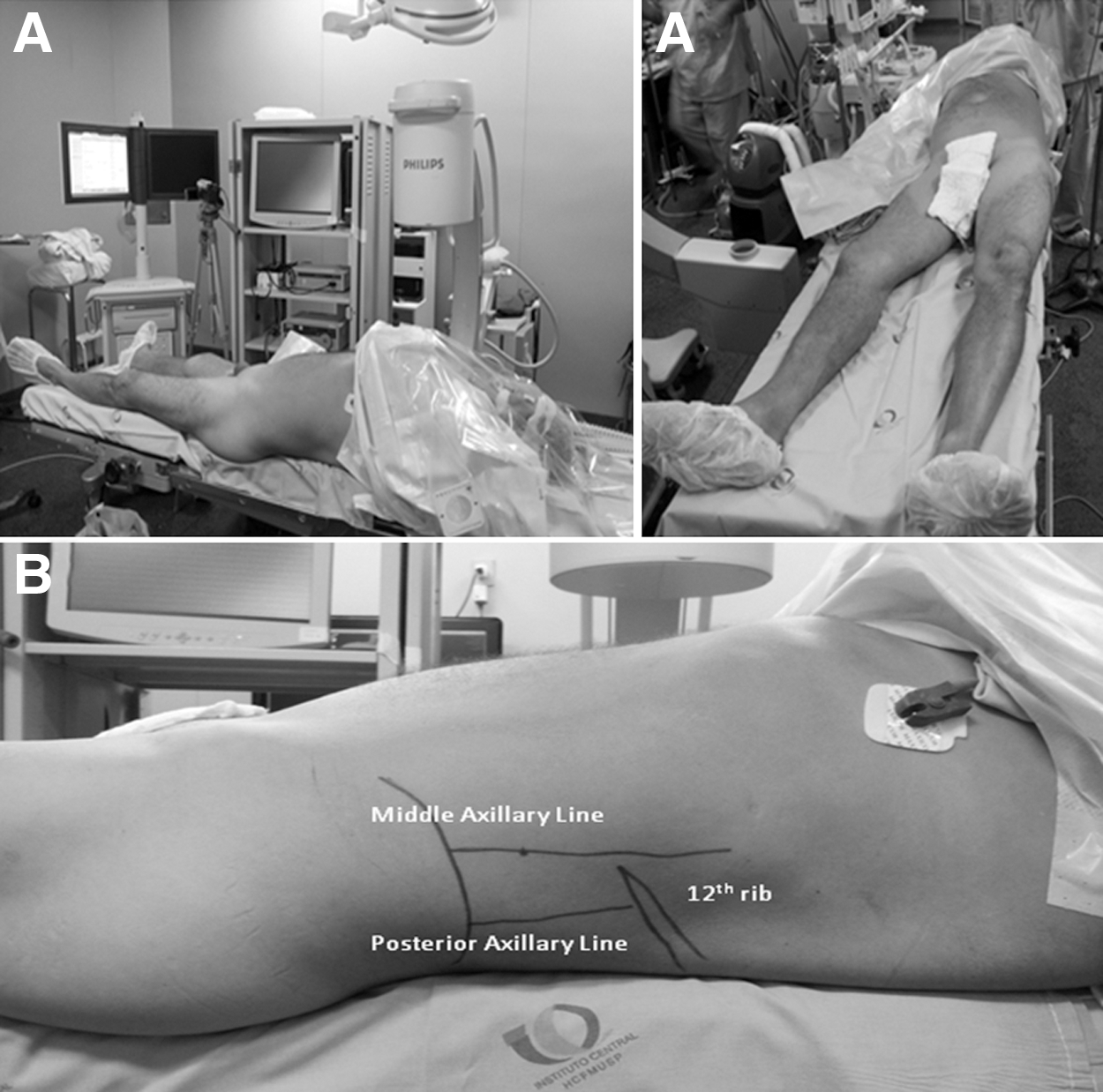
All csPCNLs were performed without a rolled towel under the flank, and the patients remained in the same position during the entire procedure. The patient was placed in the supine decubitus position with the posterior axillary line located just outside the border of the surgical table, and the flank was extended to increase the space between the last rib and the iliac crest. The ipsilateral arm was positioned over the thorax, and the legs were kept straight and positioned slightly apart (Fig. 1A). The surgical table was turned approximately 5 degrees to the contralateral side to move the patient's gravitational center medially and to avoid displacements. The last rib, middle and posterior axillary lines, and the iliac crest were marked for orientation during the puncture (Fig. 1B).
Under general anesthesia, the patients were draped only once. A 6F ureteral catheter was placed through a rigid cystoscope without a lithotomy position even in men because a flexible cystoscope was not available for all cases. After pyelography, the selected calix was punctioned by the urologist on the posterior axillary line based on the CT findings and under fluoroscopic guidance. An 18 gauge needle was horizontally inserted. It was not necessary to rotate the C-arm laterally but rather to check for deformations of the calix on fluoroscopy. For cases in which the lateral bar of the table was located over the kidney, a C-arm rotation toward the surgeon solved the problem.
If no deformation on the calix was caused by the introduction of the needle, it was pulled out and reintroduced more anteriorly (Fig. 2). When the chosen calix was deformed, the needle was inserted a little more until a sudden resistance loss was noted. Then, the needle obturator was pulled out and a drop of urine confirmed the right position. Once there, a hydrophilic guidewire was passed through the ureter to the bladder or urethra. If this guidewire did not reach the ureter, a Teflon guidewire replaced it.
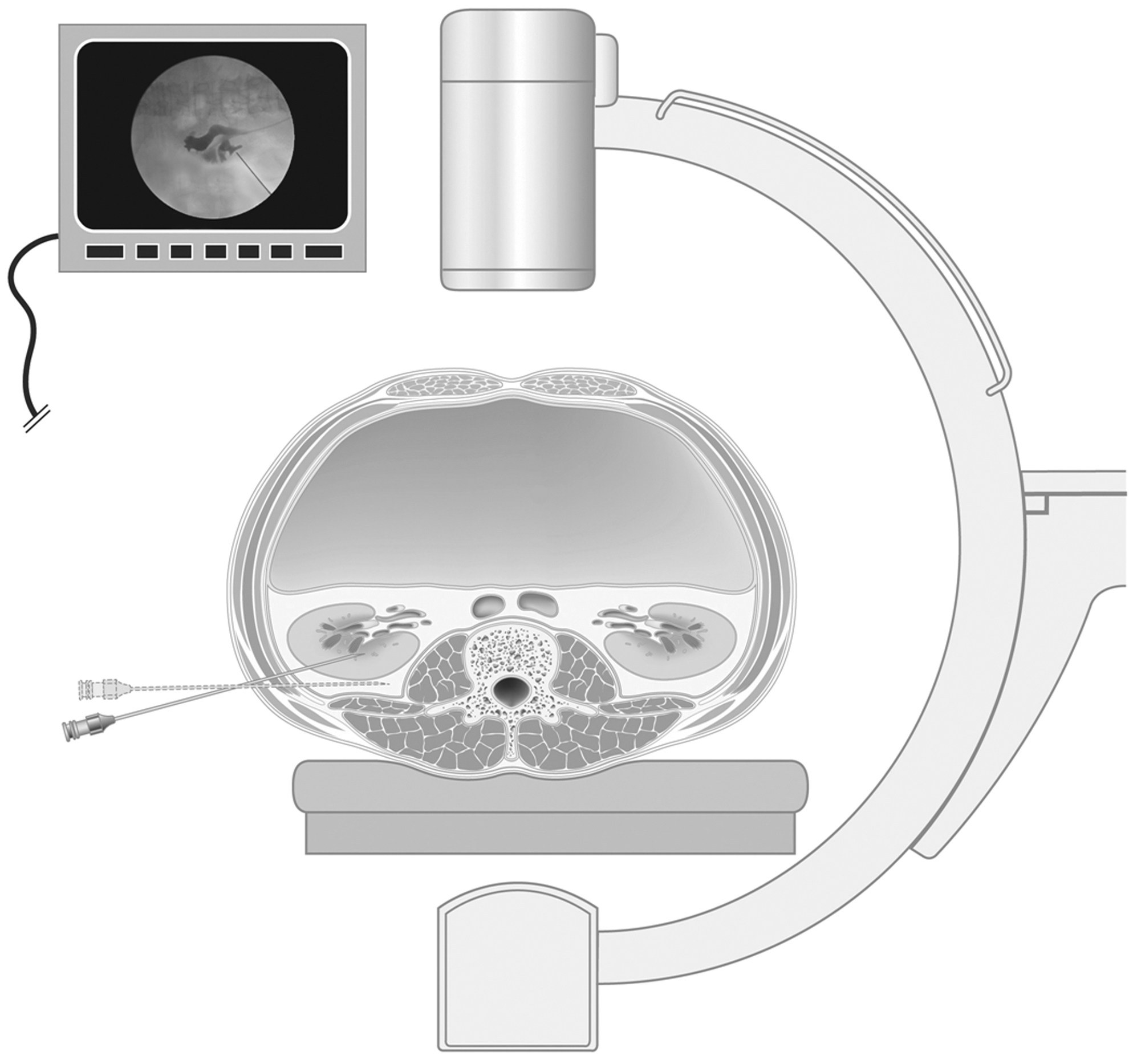
Calix puncture.
Finally, the tract was dilated with fascial dilators (numbers 10, 20, and 30, sequentially) and the Amplatz sheath was placed. We used an ultrasonic lithotripter for stone fragmentation and suction. A 16F nephrostomy tube was placed at the end of the procedure in case of bleeding, residual stones, pelvic perforation, or multiple accesses. A ureteral catheter or a Double-J stent was routinely left. Local anesthesia of the tract was achieved with 20 mL of 1% ropivacaine to improve analgesia.
Operative time was measured from the beginning of the cystoscopy for ureteral catheter insertion until the end of nephrostomy placement. A noncontrast CT scan and laboratory examinations were performed in the first postoperative day in all cases. Patients with residual stones underwent a second-look PCNL, flexible ureteroscopy, or extracorporeal shockwave lithotripsy (SWL) according to residual stone burden and location. Transfusion criteria were usually clinical. We tried to avoid blood transfusions, but it was performed if the patients became symptomatic during postoperative care. In some cases, the anesthesiologist decided for transfusion during PCNL based on hemodynamic parameters.
Success was defined as the presence of fragments ≤4 mm on the CT scan at the end of follow-up. Preoperative, intraoperative, and postoperative data were evaluated.
Results
One patient without residual stones and another four patients with residual stones after csPCNL were lost during the follow-up. These patients were included in the surgical data analysis but were excluded from the success rate evaluation. Table 1 summarizes demographic data, stone size, and the Guy stone score. Intraoperative and postoperative data are described in Table 2.
SD=standard deviation; ASA=American Society of Anesthesiologists.
PCNL=percutaneous nephrolithotomy.
There was no failure of access. The median operative time was 100 (20–240) minutes. Most (76.6%) of the patients had only one access, while 16.6% and 6.8% had two or three accesses, respectively. Inferior calix was preferred for the first access in 75% of the cases, while middle and superior calices were the first access in 20.8% and 4.2% of the cases, respectively. The superior calix was chosen as the first access only when the stones were located there exclusively. Overall, 156 punctures were performed. Supracostal accesses between the 12th and 11th ribs were used in 31 (19.8%) cases. No organ injury or significant pleural effusions necessitating drainage were noted.
The immediate and final success rates were 72.5% and 90.4%, respectively, after an average of 1.08 PCNL and 0.21 auxiliary procedures per case (18.3% of SWL and 3.3% of flexible ureteroscopy). The stone-free rate (no fragments at all) was 53.5%. Patients were left tubeless in 38.3% of the cases. There were no complications regarding the tubeless approach.
The mean reduction in hemoglobin level was 1.98±1.29 g/dL, and the transfusion rate was 4.2%. The complication rate was 16.8% (Clavien I: 5.0%; Clavien II: 6.7%; Clavien III: 3.3%; Clavien IV: 0.8%). Major complications (Clavien III or IV) included one migration of the Double-J stent, which was managed by ureteroscopy; one renal fistula managed with a Double-J, one steinstrasse managed by ureteroscopy; and one case of septic shock—the patient was treated with antibiotics. There were no colon injuries or deaths. The median time with a nephrostomy tube was 48 (24–720) hours, and the median hospital stay was 48 (24–840) hours.
Discussion
In 1976, Fernström and Johansson 2 performed the first PCNL. More than 30 years later, it remains the gold standard treatment for patients with large renal stones. 1 The initial results of PCNL performed in the supine position were described by Valdivia and associates 3 in 1998, and this technique has gained popularity through the years. Today, this procedure is performed in approximately 20% of urologic centers around the world. 8
The prone position is known to provide a large surface for puncture, a wider space for instrument manipulation, and a theoretically lower risk of colon, liver, or spleen injury. 10 Nevertheless, it is associated with higher patient discomfort, increased radiologic exposure of the urologist, longer operative time, and a risk of neural and ophthalmologic pressure lesions. 15,16 The supine position may overcome the disadvantages of the prone position, but it is criticized because it lacks the former's advantages.
Today, there are several studies that describe the outcomes and advantages of PCNL in the supine position. 4,5,7,11,17 Shoma and colleagues 17 compared the results of 130 patients who underwent PCNL in the supine and prone positions in a prospective and nonrandomized study and reported a similar overall success rate in both groups (89% vs 84%, respectively). Liu and coworkers 6 performed a systematic review and meta-analysis on PCNL in the supine versus the prone position. Although there was no difference between success, complications, and transfusion rates, the operative time in the supine position was significantly shorter than in the prone position (P<0.00001). Mazzucchi and colleagues 18 compared the outcomes of prone and complete supine PCNL in obese patients and found that although the success rates were similar, the operative time and hospital stay were shorter and that second-look PCNL and the transfusion rate were lower in the supine position.
Here, we have presented a detailed description of our modified technique for csPCNL performed by a single surgeon in two institutions under the same protocol. We decided to study a different position to solve some problems of the traditional or modified Valdivia position, such as a smaller area for renal puncture and difficulty with nephroscope manipulation, which is usually limited by the surgical table or the lumbar bolster. When describing their modified Valdivia position for PCNL, Neto and associates 11 proposed crossing the patient's legs and, thus, enlarging the flank field for the procedure. In our study, we kept the legs straight and slightly apart. The ipsilateral flank was extended and located on the border of the surgical table to improve the operative field and to allow access to the urethra without putting the patient in the lithotomy position. This technique proved feasible and effective, because more than one access was performed in approximately 25% of the cases. Limitations regarding the nephroscope manipulation were minimized and restricted to patients with large hips and high kidneys. In all cases, we were able to introduce the ureteral catheter with the rigid cystoscope without repositioning the patient, which resulted in a shorter operative time.
When our protocol was designed, no other group had described a complete supine technique. A few months later, Falahatkar and coworkers 4 published a randomized study comparing the outcomes of 40 csPCNL with 40 prone PCNL. In that article, the authors described csPCNL with the patient in a position similar to ours. There was no bolster under the flank, and the patient was located on the border of the surgical table with the legs straight and slightly apart. A difference remained in the lithotomy position for ureteral catheter placement and in the positioning of the ipsilateral arm, which we located over the thorax and did not leave opened as Falahatkar and coworkers 4 proposed. We used this position because the opened ipsilateral arm can occasionally disturb the surgeon and assistants.
Our stone-free rate based on CT (immediate success rate of 72.5% and final success rate of 90.4%) shows that our technique is as effective as the others previously described in the prone or supine position. 3,4,6 Falahatkar and coworkers 4 showed that csPCNL was safe and as effective in terms of stone-free rates as prone PCNL (80% vs 77.5%, respectively, based on radiography of the kidneys, ureters, and bladder (KUB). Neto and colleagues 11 reported a success rate of 70.5%, which was also based on KUB radiography and ultrasonography. Valdivia and coworkers 8 reported a success rate of 70.2% in a study including several institutions around the world.
Our complication rate was 16.8%, including 12.7% of Clavien I or II, which are minor complications that did not need additional intervention. According to the Clinical Research Office of the Endourological Society (CROES) study performed by Valdivia and coworkers, 8 complication rates were 19.2% for the supine position and 20.8% for the prone position. Our transfusion rate was 4.2% and was similar to those reported by the CrOES study and Neto and associates 11 but lower than the one reported by Falahatkar and coworkers 4 (20.2%).
Most urologists believe that there is a higher risk of colon injury with patients in the supine position than in the prone position, but this is not true. It has been shown that when a CT scan is performed with the patient in a supine position and then in a prone position, the colon lies retrorenal and is at risk for injury in 1.8% and 10% of the cases, respectively. 19,20 In addition, no instance of colon injury during a supine PCNL has been described in the literature. In our series, we also did not cause any colon injury or damage to other organs. Supracostal punctures were performed in 19.8% of the cases; all were under the 11th rib, and none caused significant pleural effusion.
A supracostal puncture in the supine position is relatively poorly studied. It has some peculiarities, because this procedure is usually performed over the tip of the 12th rib where the pleural reflection is not present. In our series, it was not associated with major complications. Most supracostal punctures were only detected after the postoperative CT scan. Neto and associates 11 had a 4.5% rate of supracostal punctures, but they did not perform CT scans after the procedure, which could have increased the rate.
Tubeless csPCNL was performed in 38.3% of our cases, according to restricted criteria. Similar to Falahatkar and colleagues, 21 who evaluated 117 patients who underwent a tubeless csPCNL, we also did not observe any major complications. Tubeless csPCNL is associated with a lower intake of analgesics and a faster discharge from the hospital. 22
Our study has some limitations. It was based on the outcomes of a single surgeon; therefore, other studies from different institutions and surgeons are necessary to validate the results. As it is a descriptive study, no control group was included. This study did not include any case of anomalous kidneys, such as pelvic or horseshoe kidneys; thus, it is not possible to apply our results to such situations. This study, however, involved a prospective series; all patients were controlled with CT scan preoperatively and postoperatively; complications were graded according to the modified Clavien score; and few patients were lost during follow-up.
Our technique combined the advantages of the supine position with a wider field for puncture and instrument manipulation. In addition, patients remained in the same position during the entire procedure. It also proved safe and effective because of our high success rate and low complication and transfusion rates. Thus, we consider it a good option for all patients with normal kidneys.
Conclusion
Our modified complete supine PCNL is a safe, feasible, and effective procedure with excellent outcomes and a low rate of complications. It provides the same advantages as traditional supine PCNL and also provides a good area for kidney access and surgical instrumentation.
Footnotes
Disclosure Statement
No competing financial interests exist.