
Abstract
Background and Purpose:
Laparoscopic resection of extra-adrenal pheochromocytoma (EAPs) necessitates meticulous surgical procedures because of changes in anatomic disposition and/or proximity to major blood vessels. Complete resection can be traumatic and may cause an increase in catecholamine levels. We present our experiences with laparoscopic resection of EAP (LEAP) and compare the intraoperative hemodynamics with those during laparoscopic resection of adrenal pheochromocytoma (LAP).
Patients and Methods:
We retrospectively reviewed the medical records of five patients who underwent LEAP (retrocaval EAP, n=2; interaortocaval EAP, n=1; periadrenal EAP, n=2) and five who underwent LAP between October 2001 and October 2011. We also evaluated fluctuations in blood pressure (BP) reported during both surgeries.
Results:
The tumors were successfully resected under laparoscopic guidance in both groups, and conversion to open surgery or blood transfusion was not needed. Intraoperative hypertension (BP>200 mm Hg) was observed in three LEAP and four LAP patients, whereas intraoperative hypotension (BP<80 mm Hg) was observed in five LEAP and three LAP patients. No significant differences were observed between groups, however.
Conclusions:
Laparoscopy is the method of choice for surgeons experienced in EAP resection because it is feasible and reproducible with appropriate preoperative planning, similar to LAP.
Introduction
A definitive treatment for EAP is surgical resection. Excessive catecholamine release from the tumor, however, can make surgical treatment difficult because of the risk of serious perioperative complications such as acute hypertension that is caused by manipulation of the tumor or sudden hypotension that occurs immediately after clamping the main vein. With careful preoperative medical treatment, appropriate patient selection, intensive anesthetic management, and less tumor manipulation, laparoscopic resection of AP (LAP) has been shown to be safe and associated with lower morbidity and improved convalescence when compared with open procedures. 6 –9
In the past few years, some studies have focused on differences in endocrine and cardiovascular changes occurring during LAP and open adrenalectomy for AP; all these studies have concluded in favor of the laparoscopic approach. 7,10 –12
The surgical procedures needed during laparoscopic resection of EAP (LEAP) are more meticulous than those needed during LAP because of changes in anatomic disposition, the possibility of dense adhesions and/or high vascularity around the tumor, and proximity to major blood vessels. For complete resection, a relatively traumatic dissection is needed because of unavoidable circumstances, and this may cause an increase in catecholamine levels. Despite appropriate preoperative medical treatments and intensive anesthetic management, LEAP is associated with the risk of serious perioperative complications such as acute hypertension.
In contrast to LAP, LEAP has not been studied frequently because of the rarity of EAP. 13 –17 Moreover, to the best of our knowledge, no reports have examined the intraoperative hemodynamic consequences that occur during LEAP. To confirm the feasibility and safety of LEAP, we reviewed our experiences with LEAP and compared the surgical outcomes of LEAP with those of LAP in terms of fluctuations in blood pressure (BP) during either surgery. We have also described our surgical strategy that was designed to avoid significant catecholamine release by surgical manipulation of the tumor during LEAP.
Patients and Methods
We retrospectively evaluated the medical records of five consecutive patients who underwent LEAP (retrocaval EAP, n=2; interaortocaval EAP, n=1; periadrenal EAP, n=2) and five who underwent conventional unilateral LAP between October 2001 and October 2011. The clinical presentations were typical in all but one EAP patient. Sustained hypertension and transitory hypertensive crises that were controlled by medical therapy were the most frequent symptoms. Diagnostic imaging included CT, MRI, and 123I-metaiodobenzylguanidine (123I-MIBG) scintigraphy. Features suggestive of malignancy, such as local fixity, invasion of the surrounding organs, venous thrombosis, and lymphadenopathy, were not evident.
In the LEAP group, CT angiography was performed for preoperative assessment and surgical planning, if necessary. Biochemical assessments included the measurement of plasma catecholamine levels and/or catecholamine or catecholamine metabolite levels in a 24-hour urine sample.
Patient characteristics are shown in Table 1. Tumors in the LEAP group were significantly larger than those in the LAP group (mean 4.8 cm; range 3.9–7.0 cm vs mean 2.9 cm; range 2.5–3.7 cm, respectively; P<0.05). Abnormal catecholamine excretion and positive findings on 123I-MIBG scans were observed in all patients. Therefore, all patients had a diagnosis of catecholamine-secreting tumors before surgery. None of the patients had familial syndromes.
Data presented as mean±standard deviation.
Defined as tumor largest dimension.
BMI=body mass index; sBp=systolic blood pressure; dBp=Diastolic blood pressure; EP=epinephrine; NEP=norepinephrine; EAP=extra-adrenal pheochromocytoma; AP=adrenal pheochromocytoma.
Preoperative medications, including antihypertensive drugs, were administered to all patients to dilate the vascular bed. These medications were selected on the basis of the type of catecholamine secreted, and they included alpha-blockers (doxazosin) and beta-blockers (atenolol) that were administered alone or in combination and calcium channel blockers if needed. In general, the medications were administered for at least 1 week before surgery. None of the patients underwent preoperative transfusions of packed red cells to expand blood volume. A stable BP of ≤140/90 mm Hg and a heart rate of <100 beats/min for 3 days were prerequisites for surgery.
During surgery, vital signs, arterial BP, and central venous pressure were continuously monitored. Arterial BP was monitored using a radial artery line in all patients. Pharmacologic intervention, including antihypertensive drugs to prevent hypertensive crises that could occur because of excessive catecholamine increase and antihypotensive drugs to managed serious hypotension that could occur just after clamping the main vein, was performed when needed by skilled anesthesiologists. Hemodynamic data were collected from anesthesiology records. A carbon dioxide (CO2) pneumoperitoneum was maintained at <12 mm Hg during the entire procedure.
The following intraoperative hemodynamic parameters were assessed: Highest intraoperative BP, interval in minutes during which the systolic BP (sBP) was >30% of the preinduction baseline, interval in minutes during which the sBP was >200 mm Hg, lowest intraoperative BP, interval in minutes during which the sBP was <30% of the preinduction baseline, highest and lowest heart rates, and duration of tachycardic (>110 beats/min) and bradycardic (<50 beats/min) episodes. These hemodynamic parameters were chosen on the basis of a previous report of patients with AP, where they served as descriptors of hemodynamic instability. 18 Data for the two groups were statistically compared using chi-square tests and unpaired Mann–Whitney U tests, with P values of <0.05 indicating statistical significance.
Surgical technique
LAP
LAP was performed using the transperitoneal approach. In patients with right AP, the standard transperitoneal anterior approach was applied, whereas in patients with left AP, the standard transperitoneal lateral approach was applied. Early or delayed ligation of the adrenal vein was not performed because of its known difficulty and for safety reasons.
Laparoscopic resection of retrocaval EAP
Our surgical technique for the laparoscopic resection of retrocaval EAP has been described previously. 19 Briefly, five ports were placed transperitoneally. The tumor was exposed behind the inferior vena cava (IVC) (Fig. 1), which was medially mobilized to expose the tumor surface completely. Thereafter, we proceeded with dissection of the posterior attachment of the tumor. The feeding artery was transected using an ultrasound coagulator. Finally, the tumor and right adrenal gland were completely resected.

Patient 1: Retrocaval extra-adrenal pheochromocytoma. The tumor (arrow) is compressing the inferior vena cava (arrowhead) in an anterior direction.
Laparoscopic resection of interaortocaval EAP
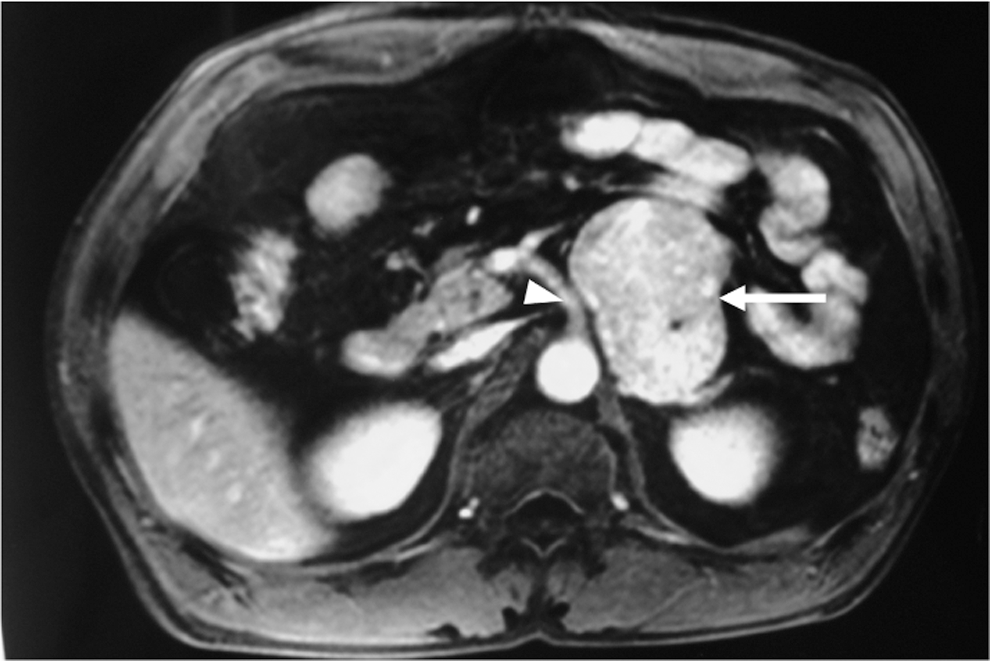
Under general anesthesia, the patient was placed in a 70-degree left lateral decubitus position. Four ports were placed transperitoneally. After liver retraction, the duodenum and pancreatic head were extensively kocherized to expose the IVC. The use of electrocautery was kept to a minimum near the duodenum. Thereafter, the interaortocaval mass (Fig. 2) was readily identified behind the jejunum.

Patient 5: Interaortocaval extra-adrenal pheochromocytoma. A soft-tissue density mass (arrow) is seen approximately at the L2–L3 level, without invasion of the aorta, inferior vena cava, or jejunum.
Initial dissection was performed at the border between the anterior surface of the tumor and the jejunum. The border was carefully dissected, and the jejunum was medially mobilized to expose the anterior surface of the tumor completely. Next, the border between the posterior surface of the tumor and the anterior surface of the IVC were carefully dissected, beginning at the right edge of the mass and the anterolateral surface of the IVC. Because this plane was developed progressively, the mass was lifted off the anterior surface of the IVC and retracted medially with the aid of gravity. Thereafter, we proceeded with dissection of the posterior attachment of the tumor.
For each plane abutting the major vessels, the dissection proceeded on the surface of the mass itself. The vascular feeding branches were isolated and controlled with monopolar cautery or titanium clips, selected according to vessel size. Hemostasis was confirmed, and the mass was resected en bloc and placed in an endobag.
Laparoscopic resection of periadrenal EAP (Figs. 3 and 4) was performed using the transperitoneal approach, similar to that used for LAP. In patient 2, dissection was initiated by taking down the splenic flexure with ultrasonic shears. Once the colon was reflected, the lateral margin of the tumor was identified to abut the spleen and splenic vessels. The medial margin of the mass was then approached, and it was found to be adjacent to the pancreas. The spleen was further mobilized until the stomach was visualized. The mass was noted to be well encapsulated, and it was carefully dissected off the splenic vessels and pancreas.
Patient 2: Left periadrenal extra-adrenal pheochromocytoma. The tumor (white arrow) is compressing the celiac artery (white arrowhead).

The tumor (white arrow) is also compressing the left renal vein (black arrowhead) in a caudal direction.
Next, we dissected the upper pole of the kidney for mobilization. This procedure improved the visibility of the deep attachments of the mass. The upper pole of the kidney was caudally retracted, which facilitated resection while avoiding capsule injury and minimizing traumatic retraction of the mass itself. At this point in the procedure, the left renal vein was exposed. The tumor was observed to be compressing the left renal vein in a caudal direction. Intra-abdominal ultrasonography was performed to confirm the tumor shape. There were no signs of invasion of the renal vein or venous thrombosis.
Careful dissection enabled excellent visualization of the gonadal and adrenal vein branches of the left renal vein. After careful dissection, the adrenal vein was picked up by clips and divided. The deep attachments to the mass were then addressed. We maintained adequate retraction of the mass while separating the posterior retroperitoneal attachments. The dissection was then continued, and the attachments of the mass to the lateral abdominal wall and diaphragm were separated. Finally, the tumor and ipsilateral adrenal gland were resected en bloc and placed in an endobag.
In patient 4, four ports were placed transperitoneally. The right triangular ligament and the retroperitoneal liver attachments were cauterized and divided to allow for liver retraction and exposure of the upper limits of the tumor. After dividing the retroperitoneum, the IVC was identified and dissected from the tumor. The entire tumor was hidden by the right upper pole of the kidney (Fig. 5). Therefore, we dissected around the entire right kidney for mobilization. The right kidney was gently pushed caudally with endo-peanuts, which improved the visibility of the deep attachments of the mass. Finally, the tumor and ipsilateral adrenal gland were resected en bloc and placed in an endobag.

Patient 4: Right periadrenal extra-adrenal pheochromocytoma. The tumor (arrow) is hidden behind the upper pole of the kidney (arrowhead).
Results
The patients' perioperative data are shown in Table 2. None of the patients' procedures needed conversion to open surgery. In four patients from the LEAP group, the tumors were adjacent to the ipsilateral adrenal gland; therefore, they were resected en bloc with the adrenal gland. The mean surgical duration was 160.4 minutes (range 116–201 min) in the LAP group and 290.4 minutes (range 189–440 min) in the LEAP group (P=0.067). The estimated blood loss in the LEAP group (mean 162.0 mL; range 20–475 mL) was higher than that in the LAP group (P=0.151). These differences were not significant, however, and none of the patients needed blood transfusion.
LEAP=laparoscopic extra-adrenal pheochromocytoma; LAP=laparoscopic adrenal pheochromocytoma; BP=blood pressure.
During adrenergic crises, arterial BP was higher in the LEAP group (mean 221.6±52.5 mmHg; range, 160–299 mmHg) than in the LAP group (mean, 200.4±43.1 mm Hg; range 140–262 mm Hg). This difference was also not significant (P=0.505). With intensive anesthetic management, no significant differences were found in the incidence of intraoperative hypertensive crises (defined as a sudden rise in sBP to over 200 mm Hg during laparoscopic manipulation) between the two groups (P=0.773). The use of intravenous beta-adrenergic antagonists or phentolamine can help in controlling tachyarrhythmias and hypertensive responses triggered by intra-abdominal surgical manipulation (Table 3). In contrast, arterial hypotension may occur after exclusion of the secreting tumor and acute depletion of circulatory catecholamines, necessitating the administration of sympathomimetic drugs. Intraoperative hypotension (BP<80 mmHg) occurred in five LEAP and three LAP patients, with no significant differences between the two groups.
LEAP=laparoscopic extra-adrenal pheochromocytoma; LAP=laparoscopic adrenal pheochromocytoma.
Postoperative complications occurred in one patient from the LEAP group (Patient 4) and one patient from the LAP group (Patient 9). The former exhibited unexplained delayed emergence from anesthesia. Tracheal intubation was maintained until the end of surgery. This patient was transported to the intensive care unit on mechanical ventilation, and she met the extubation criteria 8 hours after surgery. No neurologic deficits were apparent. She was discharged on postoperative day 8 in an ambulatory condition. Patient 9 exhibited disorientation 10 days after surgery. During surgery, the highest sBP value was 200 mm Hg whereas the lowest sBP was 100 mm Hg. This patient demonstrated no neurologic deficits after waking from anesthesia. Brain CT performed on postoperative day 10, however, revealed a cerebral infarction in the left temporal lobe. The patient's status gradually improved, and he was discharged from the hospital 20 days later with no motor disturbances.
Discussion
Once a diagnosis of AP or EAP is made, appropriate preoperative medical management is necessary to decrease the risk of perioperative complications. Although adequate preoperative medical preparation limits intraoperative cardiovascular instability, hypertensive crises can still occur as a result of significant catecholamine release caused by surgical manipulation of the tumor. During surgical manipulation, catecholamine levels can exceed the normal plasma concentration by 1000-fold, resulting in hypertensive crises, cardiac arrhythmias, cerebrovascular accidents, myocardial infarctions or ischemia, pulmonary edema, and/or multiorgan failure. 6
In the past few years, some studies have focused on differences in endocrine and cardiovascular changes occurring during laparoscopy and open adrenalectomy for AP. These studies retrospectively compared groups of well-matched patients who underwent surgeries using these different modalities. 7,8,11,20 –24 They demonstrated smaller increases in plasma catecholamine levels and significant benefits in terms of pharmacologic management of hypertensive peaks during laparoscopic surgery. These benefits were ascribed to the less traumatic nature of laparoscopic dissection, which causes a decrease in catecholamine levels as measured by multiple intraoperative blood collections. Therefore, AP resection should be performed using a laparoscopic approach whenever possible.
In this study, neither early nor delayed ligation of the adrenal vein was performed. Traditionally, the adrenal vein is ligated early during LAP. 25,26 Patient anatomy or lesion size, however, can sometimes make early dissection of this vein difficult or unsafe. Recently, several authors have reported that the intraoperative hemodynamic parameters associated with delayed adrenal vein ligation during LAP are comparable with those associated with the ‘‘vein-first’’ technique. 27,28 Therefore, laparoscopic management using the vein-first technique remains controversial. In our opinion, early or delayed division of the vein should be decided on an individual basis.
On the other hand, EAP is traditionally resected by open surgery because of multicentricity, malignancy (30%–40%), and close proximity to vital structures. Some surgeons have successfully applied laparoscopic techniques to EAP resection. 14 –18 The risk of massive hemorrhage remains, however, even if the surgeon exercises caution and handles all specimens carefully—relatively traumatic dissections are needed for complete resection because of unavoidable circumstances. These maneuvers may cause an excessive increase in catecholamine levels and serious perioperative complications such as acute hypertension.
Laparoscopic surgery has a number of limitations such as the lack of tactile sensation and a restricted view of the operative field. Furthermore, inadvertent lesions of small vessels may lead to bleeding that cannot be controlled under laparoscopic conditions, necessitating conversion to open laparotomy. These limitations are particularly evident during LEAP because of variability in the number and course of feeding vessels. Therefore, extensive preoperative knowledge of the vascular anatomy of the tumor is important for surgical planning of the ideal approach for LEAP, which varies for each patient.
Of late, it has become possible to map the patient's vascular anatomy using CT angiography, and image processing using rendering software can be used to reconstruct a three-dimensional model of the feeding vessels. In this study, CT angiography was performed when necessary for preoperative assessment before LEAP. Therefore, differences between the two groups in highest intraoperative systolic BP and incidence of intraoperative hypertensive crises were not significant, and in all patients, the increase in mean arterial pressure was corrected by adjusting the infusion rate of labetalol and sodium nitroprusside.
In our opinion, to avoid an excessive increase in catecholamine levels, it is necessary to excise EAP en bloc with minimal handling. This principle cannot be overemphasized. Considering the small number of patients enrolled in this study and the overall low prevalence of the pathologies investigated here, our results cannot be considered conclusive. We are confident in stating, however, that LEAP can be performed with less traumatic laparoscopic dissection in critical patients, which may result in a decrease in intraoperative catecholamine levels and fewer perioperative complications.
With regard to retroperitoneal EAP, the laparoscopic approach as well as the retroperitoneoscopic approach can be useful depending on tumor location. Walz and associates 17 reported laparoscopic resection of tumors located caudal to the renal vessels; EAP in the upper retroperitoneum was typically resected using the posterior retroperitoneoscopic approach. They emphasized that the retroperitoneal approach offers the advantage of dissection without the interference of the intra-abdominal organs, thus avoiding the respiratory and hemodynamic effects of the CO2 pneumoperitoneum and facilitating direct access without the need to mobilize the abdominal organs. With direct access without maneuvering in the peritoneum, this approach may decrease surgical duration compared with the transperitoneal approach. With this technique, however, it is difficult to create a retroperitoneal space for insertion of the trocar, and the laparoscopic surgeon does not have the anatomic landmarks needed to proceed with the dissection. In addition, the working space is restricted.
We always use the transabdominal laparoscopic lateral approach for LEAP because we believe that this approach offers the best visualization of the major vessels adjacent to the tumors; in addition, it facilitates maximal tumor exposure. We suggest that, during the learning curve for laparoscopy, young urologists should perform LEAP using the transperitoneal approach. In expert hands, both the transperitoneal and retroperitoneal approaches are feasible, and the choice depends on personal preference and tumor location. A large but well-encapsulated EAP without local invasion can be resected laparoscopically. The indications for LEAP should be considered with caution, however. When adequate retraction of the mass cannot be maintained because of unavoidable circumstances or limited working space, conversion to an open procedure should be a decision made early, before fracture of the tumor capsule or excessive retraction of the tumor itself.
Conclusions
LEAP presents a greater therapeutic dilemma to surgeons and is considered to be more challenging compared with standard LAP. Intraoperative hemodynamic instability remains a major concern during LEAP. Even in experienced hands, the procedure may be associated with a longer surgical duration and an increased perioperative complication rate compared with LAP. Despite these concerns, LEAP can be performed safely with preoperative normalization of BP, minimal handling of the tumor, and intensive anesthetic management. To ensure ideal preparation of patients scheduled for LEAP, very close communication between endocrinologists, surgeons, and anesthetists is essential. Such teamwork should be executed with the goal of achieving safe LEAP with minimal postoperative mortality and morbidity. Surgeons should be flexible when it comes to conversion to open surgery, however, particularly in patients needing complicated dissection or in patients with uncontrolled bleeding or malignant potential.
Footnotes
Disclosure Statement
No competing financial interests exist.