
Abstract
Background and Purpose:
It is generally advised to keep a safety guidewire (SGW) in the ureter alongside the ureteroscope during endoscopy of the upper urinary tract, but little is known of how the SGW influences the forces exerted on the ureteroscope in the ureter. The purpose of this study was to investigate whether the presence of an SGW during ureteroscopy (URS) in a normal clinical setting will influence the pushing and pulling forces exerted on a semirigid ureteroscope.
Patients and Methods:
In a 1-year period (2010–2011), 40 patients admitted to Haukeland University Hospital for endoscopic treatment of renal pelvic stone disease were included in a clinical randomized crossover trial measuring the forces needed to move a semirigid ureteroscope during URS. A digital force meter was connected to the ureteroscope to perform the force measurements. The pushing and pulling forces were measured at four locations during URS with and without an SGW. The patients were randomized to whether the first series of force measurements should be with or without SGW. Paired-samples t tests were used comparing the forces in the two series.
Results:
Significantly higher forces were found both when inserting and retracting the semirigid endoscope when an SGW was used compared with times when an SGW was omitted. The mean percentage increase in the forces with an SGW in place varied between 51.8% and 112.5% across locations and directions. A limitation is that the study has been performed with a semirigid ureteroscope only.
Conclusion:
An SGW substantially increased the resistance against moving a semirigid ureteroscope up and down the ureter. The SGW may thus be an obstacle to the ureteroscopic procedure and may even increase the risk of harming the ureter in some patients.
Introduction
The purpose of the present study has been to investigate whether an SGW in the ureter will influence the pushing and pulling forces required to move a semirigid ureteroscope in and out of the ureter. A secondary goal has been to compare the forces needed to advance and extract the endoscope in men and women.
Patients and Methods
Setting and study population
In a 1-year period (2010–2011), patients admitted to our institution and planned for endoscopic treatment of renal pelvic stones were invited to participate in a clinical randomized crossover trial. All patients were 18 years and older with normal renal function. Patients with indwelling stents or known ureteral pathology, such as ureteral calculi or ureteral stenosis, were excluded from the study. Consecutively admitted patients were assessed for recruitment. All participants signed a written consent before enrollment and after receiving written and verbal information about the trial. Two patients eligible for the study renounced participation. Of 40 patients included, 18 were women and 22 men, with a mean age of 52 years (18–81 years).
According to the side of the renal stones, 9 patients underwent force measurements in the right ureter and 31 in the left ureter.
Randomization
All patients underwent force measurements when inserting and retracting the ureteroscope both with and without an SGW in place in the ureter. Thus, the ureteroscope had to be inserted and retracted two times to complete the force measurements. The first introduction of the endoscope will dilate the upper urinary tract, and mechanical trauma caused by the ureteroscope will result in edema in the ureteral wall. This may influence the resistance to insertion and retraction in the second set of force measurements. To address this problem, we randomized the patients to one of two groups: In group 1, the first series of force measurements were performed with the SGW and the next series without the SGW in place. In group 2, the first series of measurements were performed without the SGW and the next with the SGW in the ureter. The randomization was performed electronically with 20 patients in each group. The results of the randomization were kept in 40 sealed and consecutively numbered envelopes that were opened just before starting the endoscopic procedures in each patient.
Force measurement procedure
The method of force measurement has been described in detail earlier. 8 In short, a standard semirigid ureteroscope 8.5F (Richard Wolf Medical Instruments Corporation, Vernon Hills, IL) was connected to a digital force meter (DFM). A computer linked to the DFM registered the forces in addition to displaying the real-time endoscopic picture (Fig. 1).
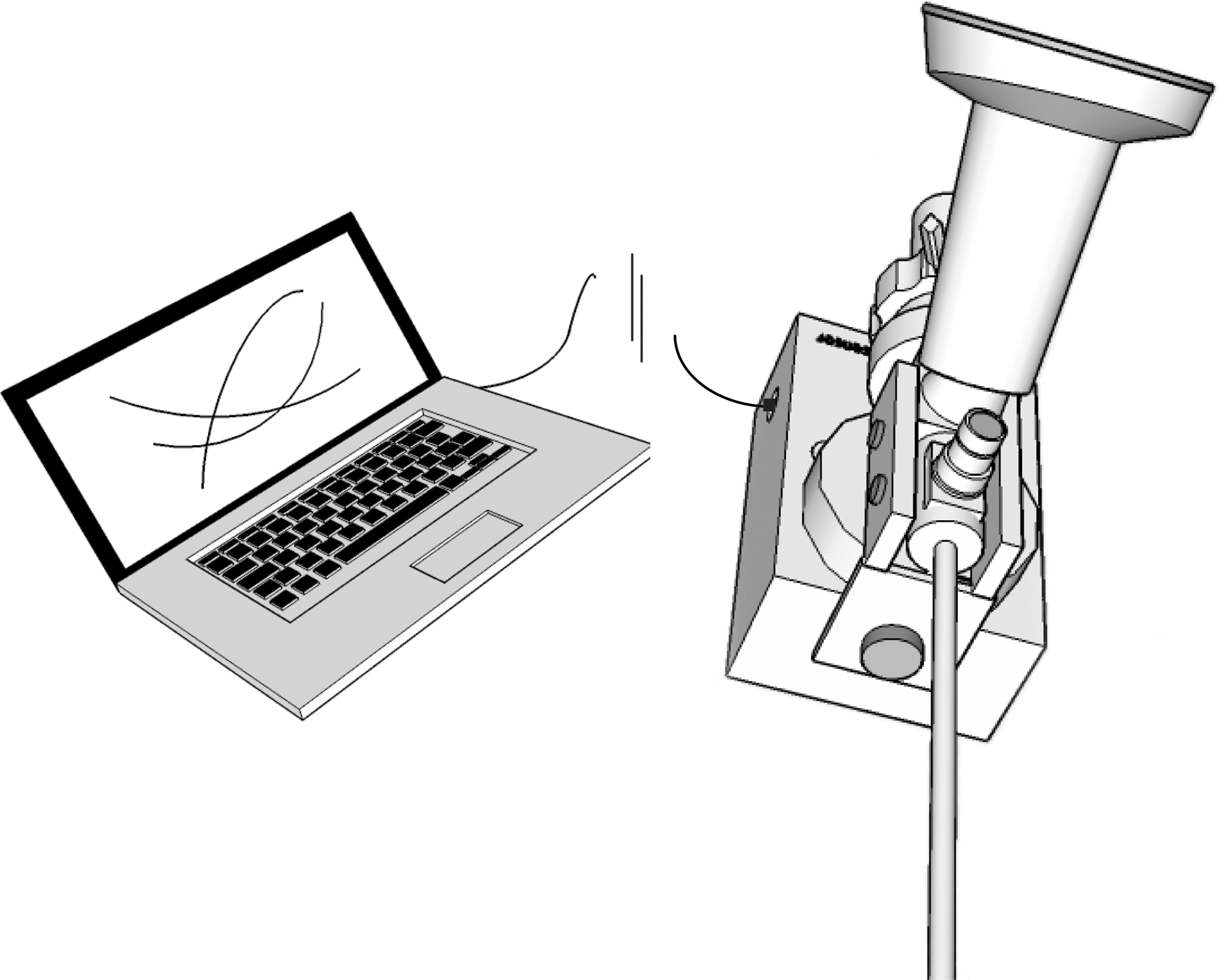
The force meter mounted to the ureteroscope and connected to a computer.
The ureteroscope was moved in the ureter by the surgeon holding the DFM without being in contact with the endoscope, ensuring the push and pull forces to be transferred from the urologist directly to the DFM.
Before advancing the ureteroscope up the ureter with the patient under general anesthesia, a hydrophilic guidewire (Terumo Glidewire® 0.035”, Terumo Medical Corporation, Somerset, NJ) was inserted through the working channel of the endoscope to straighten out the ureter in all patients. A second guidewire of the same type was used as an SGW alongside the ureteroscope in accordance with the randomization.
Force measurements were performed with the distal tip of the endoscope at four predefined locations in the ureter: In the intramural part, at the crossing of the iliac vessels, at level with the iliac crest, and 5 cm distal to the ureteropelvic junction (UPJ). Fluoroscopy verified correct positioning of the ureteroscope at the four locations in the ureter. The endoscope was introduced and extracted 3 cm at each measuring point. Registration of both the pushing and pulling forces were completed at the lowermost location before further advancement of the ureteroscope to the next measuring point in the ureter.
The forces were measured in Newton (N). Positive and negative values were registered for the pushing and pulling forces, respectively.
Statistics and approval
Paired-samples t tests were used comparing the maximum pushing and pulling forces with and without an SGW in place. A power analysis before the study was performed, assuming that the force differences with and without the SGW would be at least 0.74 N with a standard deviation of 1.2 N. A sample size of 23 would have 80% power to detect the assumed difference. To compensate for possible nonevaluable patients or measurements, 40 patients were included in the study. Independent-samples t tests were performed comparing the forces in men and women.
Statistical analyses were performed using IBM SPSS Statistics 20 (IBM, Armonk, NY). P<0.05 determined statistical significance. Force values are given as mean maximal forces±standard deviation (SD).
The study has been registered in the clinical research database, ClinicalTrials.gov (ID: NCT01117701), and was approved by the regional ethical committee.
Results
Figure 2 illustrates the patient flow through the study phases (enrollment, randomization, allocation, follow-up, and analysis). No patients were excluded from the study after enrollment, but in group 1, complete force measurements at the proximal part of the ureter were unsuccessful for technical reasons in two patients. In group 2, the force measurements were unsuccessful for technical reasons at all locations in the ureter in three patients.
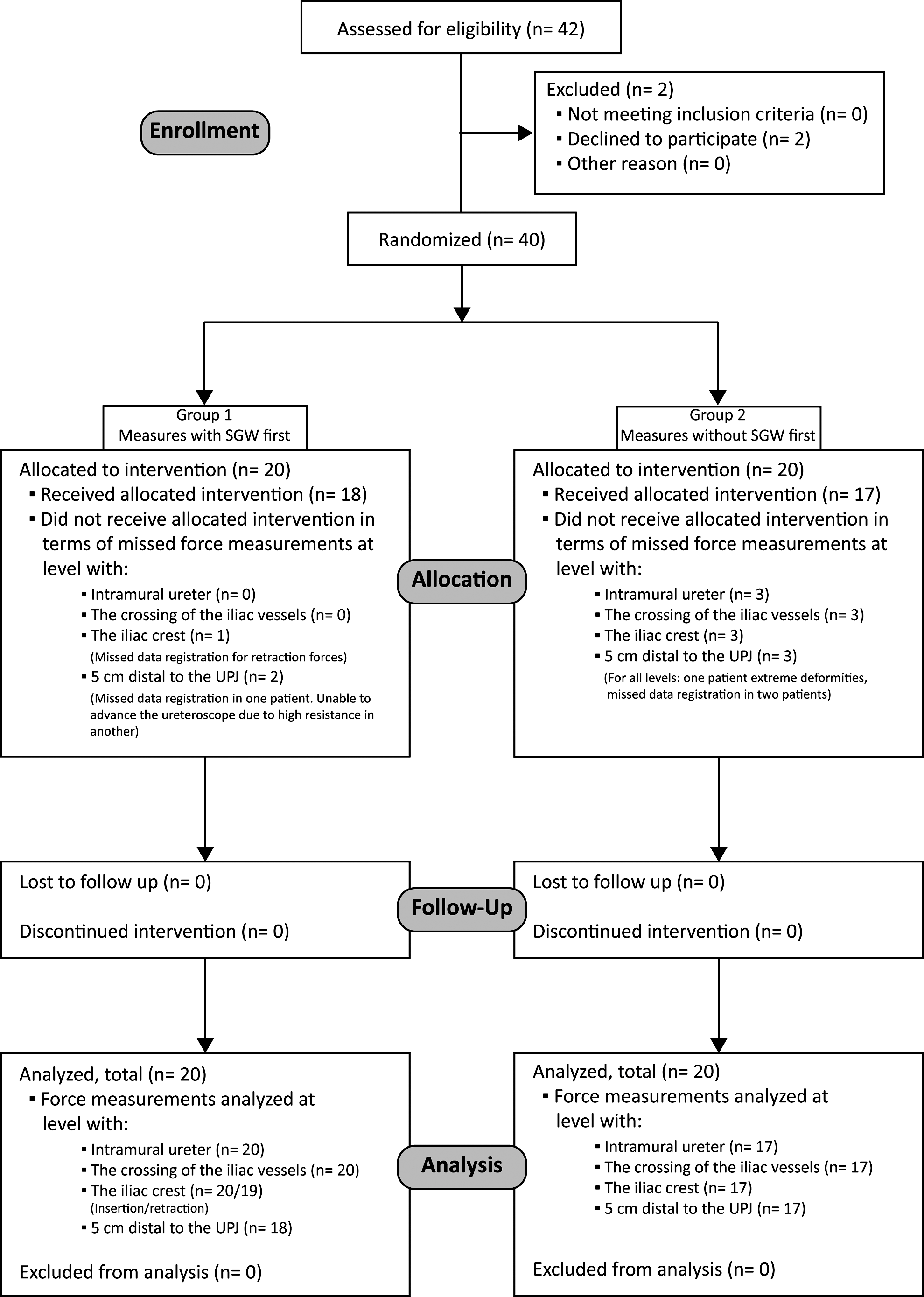
Patient flow through study phases.
Table 1 lists baseline study group demographics. Insertion of the ureteroscope in the ureter without previous dilation was successful in all patients. No prostate midlobe affecting the insertion of the endoscope through the ureteral orifice and distal ureter was seen in any of the men. The time spent on the experiment was on average 19 minutes (range 2–32 min) for each patient.
SGW=safety guidewire; ASA=American Society of Anesthesiologists.
The primary goal of the study was to compare the forces needed for insertion and retraction of the semirigid endoscope with and without an SGW in place in the ureter. The mean maximum pushing and pulling forces at the various locations in the ureter with and without an SGW are given in Table 2 and Figure 3. The forces found for insertion and extraction were significantly higher at all parts of the ureter when an SGW was used alongside the ureteroscope compared with times when an SGW was omitted. The mean percentage increase in the forces with an SGW in place varied between 51.8% and 112.5% across locations and directions. In a few patients, however, the forces that advanced the endoscope were highest at some of the locations in the ureter when an SGW was omitted.

Mean maximum forces during insertion and retraction of the ureteroscope with and without a safety guidewire (SGW). Mean forces for both insertion and retraction are illustrated as positive values.
P values refer to paired samples t test comparing measurements with and without safety guidewire.
SGW=safety guidewire; N=Newton; UPJ=ureteropelvic junction.
The forces needed to move the endoscope varied considerably from patient to patient. Just under the UPJ, the push force varied from the low extreme of 1.2 N in one patient to the high extreme of 27.3 N in another. In addition, in one patient, the advancement of the endoscope below the UPJ with the SGW in place had to be aborted because of the excessive force needed. The ureteroscope could be advanced to the UPJ in this patient, however, after the SGW had been removed. Although very large forces were used in some patients, no visible acute ureteral injuries were registered.
The force measurements in men and women are compared in Table 3. For both sexes, the forces were highest when measured with the SGW in the ureter. The pushing and pulling forces were significantly higher at all locations in men than in women both with and without an SGW in place, except for the pulling force 5 cm distal to the UPJ when measured with SGW (P=0.055).
P values refer to independent samples t tests comparing measurements in men and women.
SGW = safety guidewire; N = Newton; UPJ = ureteropelvic junction.
Discussion
Using a newly described method, 8 we have compared the forces needed for inserting and retracting a semirigid ureteroscope in patients with and without an SGW in place. The main finding in the present study is that the forces needed to insert and retract the endoscope were significantly higher at all locations in the ureter when an SGW was used alongside the ureteroscope compared with times when an SGW was omitted. The mean percentage increase in the forces that moved the ureteroscope with an SGW in place varied between 51.8% and 112.5% across locations and directions. Similar results are reported by Eandi and associates 7 who found that the resistance against moving a ureteroscope in the ureter in an ex vivo model was significantly greater when an SGW was in place.
Substantially larger forces to move the ureteroscope were found in the upper ureter than in the lower, whether an SGW was used or not. As stated earlier, straightening out a tortuous ureter by advancing the semirigid ureteroscope increases the pressure against the wall of the ureter. In addition, during advancement of the instrument the resistance between the endoscope and the ureteral mucosa increases as the contact area becomes larger. 8 It seems that the presence of an SGW, however, may be the most important cause of the increase of the resistance as the ureteroscope moves in to the proximal ureter, as seen from Figure 3. This effect may be further enhanced by the conical shape of the endoscope as the thicker shaft of the ureteroscope is introduced in the most constricted intramural ureter. 9
In one of our patients, the ureteroscope could not be advanced past the iliac crest when an SGW was used, while further advancement was possible in the same patient after the guidewire had been removed. The SGW may, therefore, in some patients be an obstacle to a successful procedure.
We found considerable variation in the forces from patient to patient. The variation is probably mainly related to anatomic and physiologic conditions. The highest pushing and pulling forces may have increased the risk of traumatic injuries in some patients, although no adverse effects have been registered. To prevent ureteral trauma, however, forced maneuvers with the ureteroscope should always be avoided. 10 Because avoidance of the routine use of the SGW reduces the forces needed to move the endoscope, it may also reduce the risk of traumatic ureteral lesions.
The increased forces needed to move the ureteroscope when an SGW is used may be caused by friction between the endoscope and the SGW and by increased pressure between the ureteral wall and the endoscope caused by the occupation of some of the intraluminal space by the SGW. The pressure against the ureteral wall is also influenced by the tone of the smooth muscles in the ureteral wall. Jung and coworkers 11 have found decreased renal pelvic pressure during URS with endoluminal isoproterenol irrigation. The role of the muscular tone in the ureteral wall in creating resistance to insertion and retraction of the ureteroscope should be studied further.
Clayman and associates 6 have studied the effect of the coating of various wires with respect to the friction between the wire and the inner surface of a ureteral model. Studies of the friction between the outer surface of the endoscope and various guidewires with different sizes and coatings should be performed to determine which SGW is the best. The quality of the SGW needs to be assessed in settings as close to the clinical situations as possible.
The coating of urethral catheters has been extensively studied to minimize the urethral trauma during catheterization. 12 Similar studies of various coatings on semirigid and flexible ureteroscopes may also be warranted.
Not surprisingly, the pushing and pulling forces were higher in men compared with women. The prostate and the urethral length are the most probable causes.
In a recent publication regarding Norwegian urologists' preferences on ureteroscopic treatment for patients with ureteral calculi, 79.3% of the physicians used SGW as a routine whenever performing URS. 13 This is in accordance with the advice given in the literature, 1,4 but recently some authors have reported that safe URS can be performed without the routine use of an SGW. 14 –16 The focus in these studies, however, has been directed toward the feasibility of routinely performing URS without SGW. Little attention was devoted to the potential adverse effects caused by the use of SGW. Further investigation comparing the clinical results of URS with and without SGW seems necessary.
Many urologists would probably feel reluctant to give up the use of the SGW just to minimize the traction forces on the ureter. Knowledge of the increased traction forces may nevertheless lead to a more shaded attitude to the generally accepted view of the SGW as mandatory during URS. What situations will allow us to dispose of the SGW cannot be assessed based on the present study, but some authors have stated that the routine use of an SGW during URS is not necessary. 7,14 –16 It is especially so in cases expected to be uncomplicated and when removing small lower pole stones where the flexible endoscope itself is considered as a safety mechanism, 14 or when the surgeon is an experienced endourologist. On the other hand, in situations with incision of a ureteral stricture or management of severely impacted stones, the use of an SGW is still advocated because of the increased risk of disturbing bleeding and need for a postendoscopic stent. 7 A frustrating paradox is, however, that in some cases, it may be impossible to pass the SGW beyond an impacted ureteral stone.
In the present study, the force measurements have been performed with a semirigid ureteroscope. Eandi and colleagues 7 found in their ex vivo study, however, similar results both with flexible and semirigid ureteroscopes. Another limitation in the present study is that only a standard SGW has been evaluated. It is likely that thinner and more lubricious guidewires create less friction.
Conclusions
The forces needed to insert and retract the ureteroscope are substantially higher when an SGW is in place compared with times when an SGW is omitted. The SGW may, therefore, be an obstacle to a successful URS and may even increase the risk of harming the ureter in some patients. Studies comparing the clinical outcomes of URS with and without SGW seem to be warranted.
Footnotes
Disclosure Statement
No competing financial interests exist.