
Abstract
Introduction/Objective:
We sought to examine the contemporary relationship between case volume and outcome for percutaneous nephrolithotomy (PCNL) using a publicly available administrative database.
Methods:
A weighted sample of 7785 patients was obtained from the 2010 Healthcare Cost and Utilization Project (HCUP) Nationwide Inpatient Sample (NIS). ICD-9-CM diagnostic codes were used to identify patients with urolithiasis (592.0, 592.1, and 592.9) who underwent percutaneous nephrostomy with fragmentation (5504). Charlson Comorbidity Indices (CCI) were calculated based on diagnostic codes for all patients. Hospital case volume was quartile classified and we then compared key outcomes (the complication rate, transfusion rate, length of stay [LOS], and in-hospital mortality rate) by volume quartile. We then performed multivariate analysis to examine the effect of CCI, annual volume, and age on key outcomes.
Results:
The overall complication rate was 17% in the weighted sample. In univariate analysis, statistically significant variation in the complication rate, CCI, transfusion rate, and in-hospital mortality was noted with regard to the hospital volume. The complication rate and transfusion rates varied by case volume, but in a nonlinear fashion, wherein rates were highest at the lowest and highest volume centers. CCI was strongly predictive (p<0.001) of complications and LOS in the multivariate analysis. Case volume was only predictive (p=0.042) of LOS in the multivariate analysis.
Conclusion:
Annual case volume of the treating center was associated with shorter LOS after PCNL, but case volume was not independently predictive of complication or transfusion in multivariate analysis. CCI was a strong independent predictor of complication and LOS.
Introduction
Yet, the relationship between volume and outcome (specifically, the complication rate) for endourologic procedures has not been extensively studied, relative to high-risk urologic oncology procedures. In the field of endourology, percutaneous nephrolithotomy (PCNL) has a unique utilization pattern; the procedure is mostly performed by fellowship-trained urologists and young urologists in practice for less than 5 years. 4 Specifically, a 2006 study reported that PCNL was performed more commonly at teaching and urban hospitals, 5 where case volumes are typically higher. Based on these considerations, we sought to examine the volume–outcome relationship for PCNL in North America. To address this question, we used the nationwide inpatient sample (NIS), a large, publicly available administrative dataset of U.S. inpatient stays.
Methodology
We collected data from the 2010 Healthcare Cost and Utilization Project NIS. The NIS dataset is maintained by the Agency for Healthcare Research and Quality and includes administrative data from 8 million hospital discharges drawn from >1000 hospitals in 44 states, approximating 20% of all hospital discharges. The NIS includes all payers, including Medicare, Medicaid, and private insurance, as well as the uninsured. The NIS is a 20% sample; so, the Healthcare Cost and Utilization Project (HCUP) advises researchers to multiple by the DISCWT (discharge weight) variable to arrive at national estimates, which are then termed “weighted samples.”
Using the International Classification of Disease, 9th revision, clinical modification (ICD-9-CM) diagnostic codes, we first identified patients with urolithiasis (592.0, 592.1, and 592.9). From this subset of patients, we identified those who were treated with percutaneous nephrostomy with fragmentation (5504). We excluded patients who had percutaneous nephrostomy without fragmentation (5503) because we did not want our analysis to be confounded by patients whose primary treatment was decompression rather than definitive stone surgery.
Baseline patient characteristics, including age and gender, were extracted. The NIS reports up to 15 procedures and 25 diagnosis codes per hospital stay. We calculated the Charlson comorbidity index (CCI) based on diagnostic codes present along with the primary diagnosis of urolithiasis. We used methodology published by Trinh et al. 6 to identify complications by searching for ICD-9 codes (Table 2) associated with complications. Intraoperative complications consisted of surgical laceration of the bowel, ureter, and nerves and/or vessels during a procedure (998.2). Blood transfusion recipients were identified using the ICD-9 procedure codes 99.02, 99.04. Five groups of postoperative complications were identified consisting of potentially life-threatening cardiac, respiratory, or vascular events, miscellaneous medical and surgical events. Urologic complications were excluded because urologic diagnoses are often miscoded as urologic complications in NIS datasets. NIS also provides data on the length of stay (LOS) and inpatient mortality.
The number of procedures performed at each hospital in 2010 was calculated using unique hospital identifiers. Median annual case volume was 10 (interquartile range 5–33) cases per center. Four volume groups were defined by separating the hospitals' volume into quartiles. We defined the first quartile volume as 1 to 5 annual cases, second quartile volume as 6 to 10 cases, third quartile volume as 11 to 32 cases, and fourth quartile volume as 33 or more cases. Once the volume groups were established, we compared the four groups to look for differences in our primary outcomes (the complication rate, LOS, transfusion rate, and in-hospital mortality rate). We then attempted to link the differences in complication rates, transfusions, and LOS with potential predictors in a multivariate regression analysis. Regression analysis was run for all three of those outcomes and potential predictors were case volume, patient age, and CCI.
Statistical tests were the two-sided t-test, chi-square test, Mann–Whitney U test, Kruskal–Wallis, and multinomial logistic regression, where appropriate. Covariates included age, CCI, and annual hospital caseload. All tests were two-sided, with a statistical significance set at p<0.05. Analyses were conducted using SAS software (Cary, NC).
Results
A weighted sample of 7785 patients was identified; 3592 (46%) had PCNL at a high- or very high-volume center. The overall complication rate was 17% (n=1305).
Descriptive analyses are tabulated in Table 1. CCI was statistically different between the four groups, although the groups were similar in that ∼90% of patients in each group had a CCI of zero or one. Third and fourth quartile volume centers treated a larger amount of patients with CCI of 3+, although the overall proportion of such patients was less than 5% in both groups. Complication rates were statistically different among groups (p=0.016), with the highest proportion of complications occurring at centers with the lowest and highest volumes (Fig. 1). A similar distribution was noted for transfusion rates, with the higher rates seen at the lowest and highest volume centers.
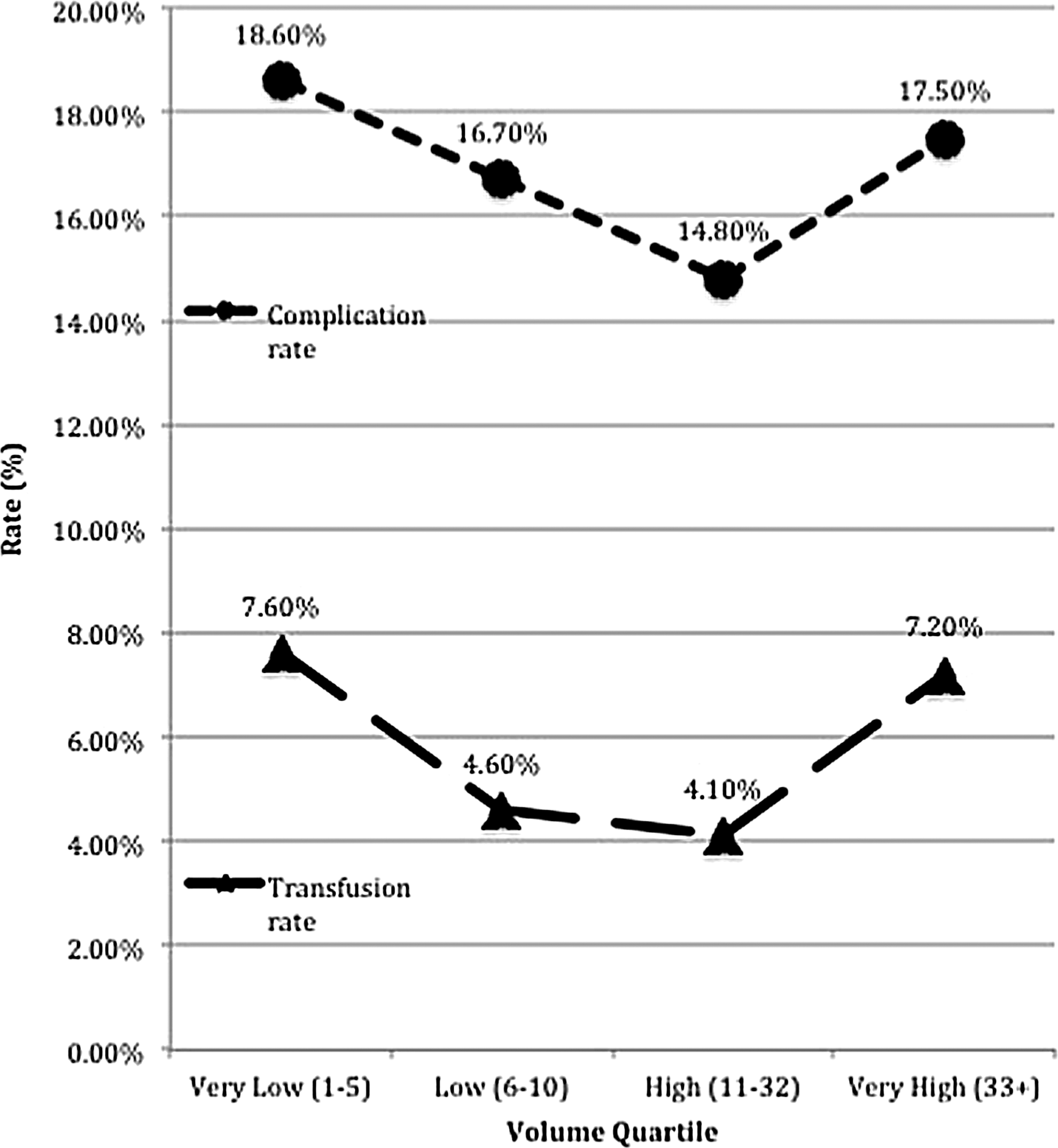
Rates of complication and transfusion by volume quartile.
CCI=Charlson comorbidity index; LOS=length of stay.
Table 2 denotes the diagnostic codes used for complication capture, separated by category. Table 3 provides a breakdown of complications by type, compared between the below-median and above-median volume groups. Cardiac, gastrointestinal, and infectious complications were more frequent in the below-median group. Patients who had a complication had a higher in-hospital mortality rate (1.1% vs. 0.1%, p<0.001) and a longer median LOS (7 vs. 3 days, p<0.001) than those who did not have a complication (data not shown in tables).
In the multivariate analysis, for the outcome of most interest, that is, the overall complication rate, CCI was strongly associated with differences in the complication rate and LOS. Hospital volume, on the other hand, was only significantly associated with differences in LOS. None of the tested variables were independently associated with differences in transfusion rates (Table 4).
Discussion
This study is one of the few that have questioned whether case volume has an impact on the outcomes of PCNL. Two notable prior studies are the recently published study by the CROES PCNL group 7 and an older study out of the University of Michigan that used the NIS to examine volume–outcome relationships. 5
The CROES study, which included 3933 patients treated at 96 global centers over a 1-year period, attempted to identify and quantify differences in key outcome variables between low- and high-volume centers. The authors show a lower operative time, lower perforation rate, higher stone-free rate, and lower rate of Clavien-classified complications for high-volume centers. Mortality was low overall, but was higher at the low-volume centers. Stone burden was equivalent between groups.
Two methodological qualities make that study quite different from ours; both relate to the definition of high and low volume themselves. First, the CROES study excluded all centers with <10 procedures; in comparison, that group comprised half of our cohort. Second, the median annual case volume was 77 cases, and as such, many of the CROES centers classified as low volume would have tended toward the higher end of volume in our study. In addition, CROES used the modified Clavien system to classify complications, which we acknowledge to be a superior method of complication recording and classification, although one that cannot be applied to currently available administrative databases. Even so, the patients in our study who had a complication also had a significantly longer LOS and, as such, we feel that meaningful complications were indeed captured.
For the above reasons, any comparison between our study and CROES must be undertaken with caution. It is interesting, however, that despite the differences in methodology, both studies showed gradually decreasing complication rates as higher volumes are reached, but an uptick in complications at the highest volume centers. It is debatable which quantitation of volume is most useful. We feel that an annual volume of 77 PCNL would be considered quite high at many American medical centers, which is supported by the volume distribution of the NIS sample itself. In this regard, the NIS is probably more representative of all centers than the CROES group, which by its very nature is more selected toward centers that perform a very high volume of PCNL. On the other hand, we may not have captured all the possible PCNLs in the NIS due to our reliance on ICD-9 codes for case identification; this could have rendered our volumes falsely low.
With regard to volume itself, a potential criticism of the study may be its attempt to define high and low volume. These terms are, in a sense, inherently subjective; high volume to one surgeon may be low volume to another and vice versa. For this reason, we have presented the data in its most objective format, that is, classification by quartile alone, without a definition of “high” or “low” volume. What we do know is that we used a consistent methodology to capture cases in this large dataset and that the volumes were evenly and fairly divided by quartiles. Furthermore, all counted cases were in fact PCNL, as opposed to mere nephrostomy placement for decompression. In that regard, at the very worst, our volume classifications could be regarded as relative, as opposed to absolute, which would still yield adequate internal and external validity. Finally, the numbers in our study compare well with the Michigan study (discussed in the next paragraph), which attests to the reproducibility of the data capture afforded by using the NIS.
The Michigan study used the NIS to examine volume–outcome relationships for over 12,000 PCNLs performed between 1988 and 2002. Two key differences between this study and our study were the focus on utilization trends (not a part of our study) and the absence of complication rates as an outcome variable (a significant part of our study). Moreover, an extramethodological difference between the studies was the time frame of the data itself; our data are contemporary, and therefore reflect many of the changes in endourologic practice patterns that have evolved over the last decade. 4 In terms of similarities, typical case volumes and the volume–mortality relationship (i.e., inverse relationship between mortality and volume) were comparable between their study and ours.
The results of the complication breakdown (Table 3) yielded some interesting discussion points. First, despite the fact that below-median volume centers tended toward a lower number of patients with high CCI scores, the rate of cardiac complications was nearly double that of the above-median centers. That finding seems unlikely to be explained by differences in the PCNL volume and may be better explained by other factors is not within the scope of our study. The other categories of complication that were different between groups were gastrointestinal and infectious complications, both of which are more frequent at the below-median volume centers. These types of complications (e.g., ileus, C-dff diarrhea, UTI, and sepsis) may be more directly relatable to factors such as PCNL volume and surgeon experience. Unfortunately, the NIS does not specifically categorize or grade complications; so, any conclusions drawn from this section of our study remain more speculative than definitive.
Critical factors that may account for the curvilinear relationship between volume and outcome and transfusion and outcome, are case complexity and patient selection. For instance, the higher rate of complications and transfusions seen at the highest volume centers may have been due to a higher rate of case complexity, a tendency toward reoperative procedures, or an academic environment, where trainees are involved in the operation. At any rate, the NIS is blind to these important factors; so, this study cannot make any definitive conclusions about their role in the observed outcomes.
The purpose of the multivariate analysis was to determine which variables were independently associated with the noted differences in the complication rate, transfusion rate, and LOS. The mortality rate could not be analyzed due to its rarity. A multifactorial logistic regression analysis was performed for the three aforementioned outcome variables, with respect to variables of age, CCI, and annual case volume classified by quartile. CCI was independently associated with differences in complication rate and LOS; volume was only independently associated with differences in LOS. This highlights the importance of comorbidity in patients undergoing PCNL; indeed, based on our results, comorbidity appeared to the most critical factor in determining both complications and hospital LOS.
Our study was not designed to determine causality, but these findings at least suggest that differences in the outcome of PCNL may not be as strongly associated with annual case volume (at the treating center) as that for other high-risk urologic procedures. Furthermore, this study suggests that patient variables (i.e., CCI) have a stronger impact on outcome than case volume itself. While that idea seems intuitive, few studies have objectively demonstrated these relationships in a fashion specific to PCNL. Whether or not contemporary trends in utilization of PCNL have leveled the playing field between lower and higher volume centers is an interesting question that could be examined in a future study.
As with any large dataset, small differences in raw numbers often translate into statistically significant differences and associations. One must ask whether or not the differences that we observed in our key outcomes are significant from a clinical standpoint. For instance, the CCI distribution reported among groups is different by the chi-square test, but the raw numbers are relatively similar between groups. Furthermore, even the raw percentages for complication and transfusion rates are relatively similar between groups. For these reasons, our data may be interpreted in at least two ways. One interpretation views the outcomes at face value and recognizes that any individual patient is likely to experience relatively similar outcomes regardless of the treating center's case volume. The other interpretation gives more weight to the statistical differences and suggests, at least from a systems standpoint, that patients undergoing PCNL fare best at a higher volume center. The two interpretations are not mutually exclusive, but are another example, where decision analysis for the individual may differ from that for the population at large.
We acknowledge several limitations of this study. The NIS is a claim-based database that contains information for a single hospital admission and has many inherent limitations. The issue of volume classification is addressed above. The primary limitation of all administrative databases is that there is a reliance on accurate coding. In addition, the NIS dataset does not include important patient characteristics such as body mass index, laterality (uni- vs bi-), stone size, or composition. In a related vein, a reviewer has asked if the NIS captures cases in which the patient was admitted under a 23-hour observation (not inpatient); the underlying concern was that such patients could be missed, which would lend considerable bias to the sample. We contacted the HCUP with this question and they confirmed that any patient treated at an inpatient facility would be captured by the NIS, even if admitted for same-day surgery or a 23-hour observation. Cases done in a strictly outpatient setting (i.e., having no association with an inpatient facility), however, would not be captured. It is our belief that a small minority of PCNLs in the United States would be performed in such facilities.
Moreover, we did not have information on surgeon characteristics (surgeon volume) or the surgical approach (tubeless vs. traditional). Perhaps, more importantly, there is no indication of who obtained access; this may have been important, as some studies have suggested that complications are higher when a radiologist obtained access. 8 In regard to outcomes, we do not know whether the patients were stone free or required additional procedures. Furthermore, because the NIS represents a single hospital stay, mortality and complication rates may be underestimated, as some patients may have had complications after discharge or died at other institutions. Despite these limitations, population-based studies are important for the study of quality of care. Population-based studies adjust for the inherent limitations of single-institution studies and allow us to study differences that may be less apparent with smaller sample sizes.
In summary, we feel that our study provides a good snapshot of the current relationship between outcome and volume for PCNL performed in the United States. There appears to be a trend toward better outcomes at centers with higher case volumes, but the trend reverses at centers of the highest volumes, which may be a product of increased case complexity or some other variable that is difficult to capture in an administrative dataset. In any event, the rates of significant complications after PCNL, as well as that of in-hospital death, remain relatively low, regardless of the treating center's annual case volume.
Conclusions
In univariate analysis, there is a significant association between quartile-classified volume and complication rates, transfusion rates, and LOS after PCNL. Complication and transfusion rates are highest at very low- and very high-volume centers; LOS is shortest at very high-volume centers. In-hospital mortality rates are lower at higher volume centers. In multivariate logistic regression analysis, CCI is the only significant predictor of both complication rates and LOS, after controlling for age and quartile-classified volume. Further studies using the NIS, or a similar dataset, could examine if the above findings have changed over time.
Disclosure Statement
No competing financial interests exist.