
Abstract
Background and Purpose:
There is a paucity of prospective long-term data on living kidney donor (LKD) quality of life (QoL). The Living Organ Donor Network (LODN) database follows donors longitudinally and cross-references with United Network for Organ Sharing (UNOS) data to assess factors that affect donor QoL.
Patients and Methods:
The Short Form (SF)-36 was sent to donors at 6 months and yearly thereafter. Recipient outcomes were determined from the UNOS database. Of 2219 donors, 1030 returned ≥1 QoL survey in the first year. Seven-hundred and thirty-one donors returned at least two surveys with 51 associated with a nonfunctioning graft and 38 with recipient death.
Results:
Initial QoL scores were not different between donors whose recipients were alive with graft function, and those whose recipients died (88.9 vs 89.2, P=0.87). For donors whose recipient died, QoL in the year after recipient death averaged 6 points lower than the initial QoL (88.9 vs 82.9, P=0.01). Thirty-one donors returned surveys an average of 4.1 years after their recipient's death. Final QoL score increased by 2.5 points, no longer significantly lower than the initial QoL (85.4 vs 88.9, P=0.16). Thirty-eight donors returned surveys in the year after their recipient's graft failure and their QoL decreased by 5.6 points on average (86.9 vs 81.2, P=0.07). Twenty-eight of these donors returned future surveys and final QoL was unchanged (81.2 vs 81.2, P=0.99).
Conclusions:
Donor QoL declines after recipient death but recovers with time. Graft failure resulted in decreased QoL without recovery. The LODN database identifies factors affecting LKD QoL and provides a model for a national registry.
Introduction
L
Because of expanding criteria for accepting patients for living donation despite obesity, hypertension, and other comorbidities, it is more important than ever to follow donor outcomes closely and responsibly. Unfortunately, there is no national database or registry to follow living kidney donor (LKD) outcomes prospectively, despite numerous authors calling for such a program. 8 –12
The Living Organ Donor Network (LODN) was established by The American Foundation for Donation and Transplantation in October of 2000 to follow kidney donor QoL prospectively. 9 It is a multicentered registry and open to any kidney donor, but initially four (and later six) centers agreed to offer enrollment to all kidney donors. At these centers, participation in the program provides the donor with supplemental health, life, and disability insurance. The program tracks donors from time of donation and assesses them with a short-form 36-item (SF-36) QoL survey at 6 months postdonation and yearly thereafter. 13 A Living Donation Survey is obtained at 3 and 6 months postdonation as well. Donor QoL was examined to determine the longitudinal effect of recipient graft failure (GF) or death.
Although other authors have reported that donor QoL is better than or equal to the general population, little is known about donor QoL over time and what factors are associated with worse outcomes. 12,14 –27 The studies published to date suffer from design limitations and are either retrospective, 14 –23,30 –35 from a single center, 12,14 –18,24 –26,28 –30 or involve fewer than 150 donors. 12,14 –16,21 –27,29,31,32,36,37 Furthermore, the relationship between recipient outcomes and donor QoL has not been well described, and concerns have been raised regarding insufficient psychological care before and after kidney donation. 32
Patients and Methods
The LODN registry enrolled 2649 patients from October 2000 through December 2010 at 26 North American centers. The majority (72%) of the patients were enrolled at those centers participating in the LODN insurance program. The remaining (28%) patients were enrolled by centers that participated in the registry for a short period, and there were several other (<1%) patients who contacted LODN directly to enroll. The patients who enrolled through centers other than the principal centers were not uniformly offered the insurance benefit. At the time of enrollment, the donors gave their informed consent to participate.
The SF-36, a validated questionnaire, was sent to all enrolled donors 6 months after donation and yearly thereafter. Questionnaires were mailed up to three times at each time point to optimize response rate. Recipient outcomes were determined from the UNOS database. Included were all donors who donated before December 31, 2010 and returned at least one QoL survey. Of 2219 donors who consented before December 31, 2010, 1030 returned a QoL survey within the first year and 841 returned at least one subsequent QoL survey, 731 in the first year (Fig. 1). UNOS data showed that of the above donors, 67 of the grafts failed and 63 of the recipients died. Of 1030 donors who met inclusion criteria, 51 GFs and 38 recipient deaths were noted. Three of the donors were associated with both GF and then recipient death within a 3-month period, and these were analyzed as recipient deaths. The initial QoL scores were compared between all donors who returned at least one survey and their recipient had either GF or mortality (Table 1).
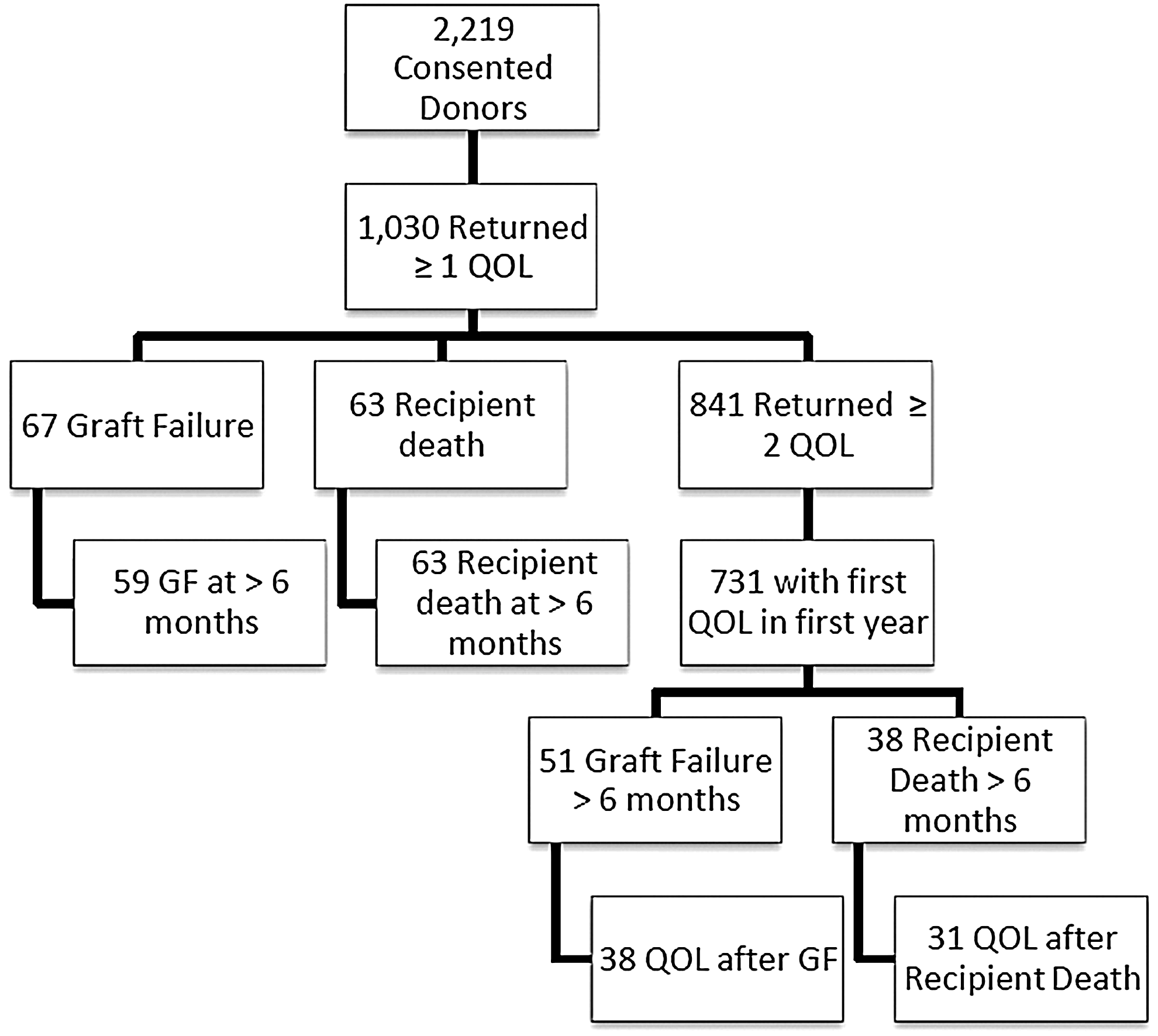
Study population. QoL=quality of life; GF=graft failure.
Statistically significant.
QoL=quality of life.
The results were analyzed with the Student t test to compare continuous data and a P of < 0.05 was used to determine statistical significance. Proportion data were analyzed with rxc contingency tables (chi-square test). GraphPad QuickCalcs (GraphPad Software, La Jolla, CA) was used for statistical analysis.
Results
Initial QoL scores were not different between donors whose recipients are alive with graft function, and those whose recipients later died (88.9 vs 89.2, P=0.87). For the 38 donors whose recipient died, QoL in the year subsequent to recipient death was an average of 6 points lower than the initial QoL (88.9 vs 82.9, P=0.01). Thirty-one donors returned surveys an average of 4.1 years after their recipient's death. Their final QoL scores averaged 2.5 points higher than right after recipient death (85.4). This improvement did not reach significance (P=0.4), but it is also not significantly lower than the original QoL (P=0.16).
For 59 donors, the recipient's graft failed more than 6 months after transplant. Their initial QoL was lower than the donors whose recipients are still alive with graft function (88.9 vs 85.0, P=0.02) and donors whose recipients died >6 months postdonation (88.7 vs 85.0, P=0.07). Eight recipients had within 6 months of transplant, and the QoL responses for their donors was the lowest at 75.5±23.6 (P=0.06 compared with GF >6 months).
Thirty-eight donors returned surveys in the year subsequent to their recipient's GF, and their QoL scores were 5.6 points lower (86.9 vs 81.2, P=0.07). Twenty-eight of these donors returned future surveys, and their final QoL scores demonstrated no change (81.2 vs 81.2, P=0.99).
The surgical approach used was reported by 88.0% of donors. Of those, 91.3 % (2131) underwent a laparoscopic operation and 8.7% (202) underwent open surgery. There was no statistically significant association between the surgical technique (laparoscopic or open approach) and donor QoL or recipient outcomes.
Of the individual QoL component scores, mental health scores were 83.8±13.6 at initial, 73.3±19.9 after death (P=0.01), and 81.3±18.5 at last survey. Vitality scores averaged 73.5±13.8 at first survey, dipped to 67.3±20.4 (P=0.14) in the year after recipient death, and returned to 73.3±19.9 at last survey.
Discussion
There is no significant difference between initial QoL scores in the donors whose recipients did well compared with those whose recipient later died. After the death of the recipient, however, the QoL scores plunge by an average of 6 points. In these patients, this decrease is most pronounced in the domains of mental health and vitality. Although this decrease may not be surprising after the death of someone with whom the donor is presumably close and often closely related (Table 1), this is a weighty reminder that there are potentially overlooked hazards associated with donation. Particularly, it highlights our duty to the donors to address their suffering after the death of their recipient.
We observed a subsequent increase in QoL as time went on after the recipient's death. Although this did not quite reach the baseline QoL score, it was not statistically significantly lower. The reasons for this are not clear, but it does appear that there is some recovery of QoL after a recipient death. To our knowledge, this effect has not been previously presented. It may be that as the grieving process progresses, the death of the recipient has less adverse impact on donor QoL.
In contrast, the donors (n=59) whose recipient had graft failure more than 6 months after transplantation seemingly foreshadowed the failure with decreased QoL scores relative to other donors. Even lower was the QoL score at 6 months of the donors (n=8) whose graft had already failed before 6 months. Interestingly, the 38 donors who returned surveys in the year after their recipient's graft failure showed another 5.6 point drop. For those we were able to continue to follow, the scores appear to remain at this nadir. This trend contrasts with the apparent diminishing of impact of recipient death as time passes. Perhaps the donors whose grafts later fail experience a distinct impact on their QoL that is more durable because of an on-going grieving process without closure.
A registry like the LODN can help to prospectively and actively identify not only donor physical health-related complications but also decreases in QoL related to poor recipient outcomes that may be amenable to treatment.
A limitation of this report is the low rate of response to the surveys. The more time that passed after donation, the less likely the donors were to respond. With a low response rate, the impact of attrition bias is augmented. The response rates were similar to those found in other publications, however. 18,19 Furthermore, there are statistically significant demographic differences related to sample size. Adverse outcomes of graft failure and recipient death are fortunately uncommon, but this does limit our study population. Although the structure of the database has changed to include a baseline SF-36 before donation, this was not collected during the period of the study. The recipient reported donor health status was not verified with the transplant center or their healthcare provider. Donor self-reporting of recipient's death and graft failure was verified with UNOS, but the health status of the recipient was not otherwise verified.
Conclusion
Donor QoL was negatively impacted by the death of their recipient, with an average 6-point drop in the year subsequent to recipient death. The final QoL score, however, was an average of 2.5 points higher an average of 4.1 years after recipient death. This was not statistically significantly lower than the initial postdonation QoL. Graft failure resulted in a 5.6-point decrease in donor QoL that appears to be durable over time.
Donors whose recipient has suffered morbidity or mortality are at an increased risk for poor QoL outcomes. A national registry that assesses donor QoL prospectively would aid in recognition of these donors who could then be offered interventions to facilitate healing and coping. Our database similarly facilitates identification of decline in individual LKD QoL and provides a model for future development of a national registry for LKDs. This should serve as another call to the transplant community to support a nationwide registry that is able to collect data prospectively for the sake of understanding potential hazards but also for identifying particular patients who may benefit from medical or mental health support.
Footnotes
Acknowledgments
The LODN registry and statistical analysis are supported and funded by the American Foundation for Donation and Transplantation. We would like to extend a sincere thank you to all living donors. We would also like to acknowledge the American Foundation for Donation and Transplantation for establishing the Living Organ Donor Network. With special thanks to the board members and Arlene Skinner.
Disclosure Statement
No competing financial interests exist.