
Abstract
Purpose:
The purpose of this study was to evaluate the amount of radiation exposure patients with small renal masses undergoing percutaneous cyroablation (PCA) or percutaneous radiofrequency ablation (PRFA) received during treatment and follow up.
Materials and Methods:
A retrospective review was conducted on all patients with small renal masses <4 cm treated with PCA or PRFA over a 7-year period in a single academic center. Preoperative, operative, and post-operative variables were collected and compared. Radiation exposure received during treatment and 1 year of follow up were also determined for each modality. Statistical analysis was conducted using SPSS V.17 (SPSS, Chicago, IL). The groups were compared using the Mann–Whitney U and Pearson Chi-Square tests. Statistical significance was considered at p<0.05.
Results:
There was no significant difference in pretreatment parameters or oncologic outcomes. The average PCA treatment radiation exposure was 39.7 mSv (15.5–133.4 mSv) compared with 22.2 mSv (8.1–67.7 mSv) for PRFA (p=0.001). During the initial year after treatment, the estimated mean treatment and follow-up radiation exposure for PCA was 134.5 mSv, compared with 117 mSv for RFA when routine computerized tomography imaging was employed.
Conclusion:
To our knowledge, this is the first published study that quantifies radiation exposure in PCA and PRFA treatment for small renal masses. These relatively high radiation exposures should be included in the informed consent for these procedures. In addition, caution should be employed when applying these technologies in young patients who are most susceptible to long-term radiation damage.
Introduction
I
Since percutaneous ablative therapies routinely require computerized tomography (CT) image guidance, patients are exposed to radiation during tumor localization, biopsy, probe placement, ablation, and follow up. Although the use of CT guidance for percutaneous ablations may be of little concern if these approaches were strictly applied in elderly patients with short life expectancy, the application of these approaches to young healthy patients is more concerning. It has been estimated that in the United States, 1.5%–2.0% of all cancers develop as a result of radiation received during CT imaging alone. 5 Although the amount of radiation exposure received during conventional CT imaging is well known, the amount of radiation received from use of CT guidance during percutaneous cryoablation and radiofrequency ablation has not been well characterized. These patients may receive multiple limited CT scans during tumor localization, probe placement, and tumor ablation; however, the imaging is routinely confined to the portion of the kidney bearing the tumor. The purpose of this study was to determine the amount of radiation exposure received by patients undergoing percutaneous cryoablation and percutaneous radiofrequency ablation (PRFA) for the treatment of small renal masses.
Materials and Methods
After institutional review board approval, a retrospective review was conducted on all patients from January 2004 to April 2010 with renal masses <4 cm treated at a single academic center with percutaneous cryoablation (PCA) or PRFA. All of the procedures were performed by the same surgical team, including an attending interventional radiologist (J.C.S.) and an endourologist (D.D.B.). Each ablative therapy was performed using CT guidance using a LightSpeed® VCT 16-slice CT scanner (General Electric Health Care, Piscataway, NJ). The procedure time was determined from the time-stamped CT images saved during the procedure. The starting time was defined as the time at which the first treatment probe was placed. The procedure end time was defined as the last CT image in the series with probes and did not include the single post-procedural CT image. The number of limited CT scans was documented for each patient. To enable adequate comparisons of radiation exposure between treatments, the CT scans used for biopsy, displacement of adjacent structures, or post-procedural imaging were not included in comparisons. Variables collected for analysis included routine operative characteristics, including procedure time, blood loss, hospital stay, complication rate, procedure success rate, and duration of follow up. In addition, the amounts of radiation that the patients received during treatment and in the follow-up period were determined.
Radiation exposure was recorded from the dose report at the end of each CT series, and it was recorded as the dose length product (DLP) in mGy-cm. The effective doses of each modality was then calculated using the ratio: Effective dose in mSv=DLP mGy-cm×17.0×10−3 mSv/mGy-cm as published by Huda et al. 6 These radiation dosages were then compared with the maximum annual permissible radiation dose allowed by the United States Nuclear Regulatory Commission.
In addition, the amount of radiation exposure during the first year of follow up was also estimated using a 3-, 6-, and 12-month surveillance regimen and a 3- and 12-month surveillance regimen. The amount of radiation for 10 follow-up CT abdomen/pelvis studies was used to estimate the mean radiation exposure at follow up. The yearly radiation exposure was also calculated using a CT abdomen alone and using magnetic resonance imaging (MRI) follow up.
Statistical analysis was conducted using SPSS V.17 (SPSS, Chicago, IL). The groups were compared using the Mann–Whitney U and Pearson Chi-Square tests. Statistical significance was considered at p<0.05.
Results
Fifty-three patients with renal masses <4 cm treated with a percutaneous ablative therapy were analyzed. The age of the patients ranged from 43.6 to 87.4, with an average age of 67.8 years. There were no patients less than age 40, 5 patients were 41–50, 9 patients were 51–60, 16 patients were 61–70, 18 patients were between 71 and 80, and 5 patients were 81 and older. One PRFA procedure could not be completed due to technical failure of the procedural equipment, and this was subsequently excluded from further analysis.
In this study, one patient underwent a PCA, after a failed PRA attempt, for a total of 53 ablations in 53 patients. PRFA was performed in 23 patients, and PCA was performed in 30 patients. Forty-one patients had dose report information available and were analyzed for differences in radiation exposure between the two ablative techniques. There was no significant difference in maximum tumor diameter (p=0.106), American Society of Anesthesiologists (ASA) score (p=0.695), age (p=0.660), or gender (p=0.185) between the two groups (Table 1).
Italicized values indicate statistical significance.
CT=computerized tomography; ASA=American Society of Anesthesiologists.
In our study, the average radiation exposure received from PCA during the procedure was 39.7 mSv (15.5–133.4 mSv). The average amount of radiation exposure for PRFA was 22.2 mSv (8.1–67.7 mSv). Patients undergoing PRFA received significantly less radiation exposure (p=0.001). There was no difference in median length of follow up between the PCA and PRFA patients (598.2 vs 737.6 days, p=0.132), hospital stay (39.3 vs 32.1 hours, p=0.102), complication rate (20% vs 13%, p=0.715), or treatment success rate (97% vs 96%, p=1.0), respectively. The mean radiation exposure received on post-operative follow-up imaging, which was a random selection from 10 representative imaging studies (CT of the abdomen and pelvis with and without intravenous contrast), was 40.2 mSv (range 25.7–73.6 mSv). For the CT abdomen alone, the radiation exposure was 20.1 mSv per study.
Discussion
This study characterizes the radiation exposure received by patients treated with PCA and PRFA. It demonstrates several important facts that should be considered by surgeons as they are selecting treatment and follow up for patients with small renal masses. Despite the fact that the imaging was confined to the tumor-bearing region of the kidney, the many different focal scans performed for probe placement and treatment resulted in a mean of 39.7 mSv for PCA and 22.2 mSv for PRFA.
Interestingly, on sub-group analysis, 52.4% of the percutaneous cryotherapy group and 30% of the PRFA group received 50 mSv or greater radiation with treatment and follow-up studies when assuming a 3-, 6-, and 12-month standard follow up. These data are compelling considering the maximal permissible radiation dose allowed annually by the United States Nuclear Regulatory Commission is 50 mSv/year. Furthermore, this amount of radiation is within the range of 5–200 mSv, which is similar to the amount of radiation affecting the people living within 3000 m of the atomic bomb in Hiroshima 7 What is even more concerning in these studies, it is documented that >50% of this population (26,300 people) were exposed to doses which were less than 50 mSv. 8
These relatively high radiation exposures are concerning. The potential harmful effects of radiation exposure from diagnostic and therapeutic imaging has been highlighted by the United States Food and Drug administration. In February 2011, the FDA issued a white paper designed to encourage physicians to limit unnecessary radiation exposure from medical imaging modalities, including CT, fluoroscopy, and nuclear medicine studies. 9 This white paper came at a time when the use of CT imaging has been growing at exponential rates. In 1980, there were ∼3 million CT scans performed in the United States compared with ∼62 million CT scans in 2006. 5 It is estimated that for every 250 female patients aged 20 who undergo a multiphase CT of the abdomen and pelvis, one will develop a radiation-induced cancer. 10
There are several possible means to reduce radiation-induced patient risk when performing ablative procedures. One method would be to encourage patients with greater than 20 year life expectancies to select treatment modalities not requiring intraprocedural radiation such as a partial nephrectomy. Alternatively, patients with long life expectancies could potentially be treated with laparoscopic approaches applied using direct vision or ultrasound (US) guidance. In a retrospective study performed by Gill et al. the 3-year cancer specific survival for T1N0M0 disease was 99.3% for laparoscopic partial nephrectomy. 11 The same group performed a prospective study evaluating 56 patients who underwent laparoscopic renal cryoablation with a 3-year follow up. In the 51 patients undergoing cryotherapy for a unilateral sporadic renal tumor, 3-year cancer specific survival was 98%. 12 Although laparoscopic ablative approaches may decrease radiation exposure, they may increase other risks as they are more invasive, require general anesthesia, and have a greater risk of bleeding and longer hospital stays than percutaneous approaches. Finley and colleagues performed a 4-year retrospective study with percutaneous cryoablation and laparoscopy for treating small renal masses. In this cohort, 11.1% of the percutaneous cryoablation patients required transfusion in contrast to 27.8% of the laparoscopic cryoablation patients. The average length of stay in the percutaneous cryoablation group was 1.3 days (range 1–4 days) and 3.1 days (range 1–6 days) in the laparoscopic cryoablation group. Furthermore, the laparoscopic cryoablation group required 3.5 times more analgesic than the percutaneous cryoablation group. 13
A second alternative to reduce the radiation exposure would be to selectively apply radiofrequency ablation in younger patients. The greater radiation exposure identified with percutaneous cryoablation is likely due to how these ablative modalities are performed. One of the advantages of cryotherapy is that the surgeon has the ability to actively monitor the ice ball to ensure complete coverage with an appropriate margin to ensure the entire tumor is treated with lethal ice. 14 With every evaluation of the ice ball, another CT scan is performed. Although cryoablation allows the surgeon to shape the iceball to avoid critical structures and ensures complete treatment of the tumor, over the course of the treatment, this leads to a significant increase in radiation exposure. In contrast, during RFA, periodic CT monitoring is not routinely performed as it has no advantage in monitoring the treatment. In addition, with RFA, a cluster probe containing three probes may be placed simultaneously, allowing less radiation exposure during probe placement. There are certainly other factors to be considered when selecting between PCA and PRFA, including surgeon familiarity and treatment success. In our small study, there was no difference in recurrence rates noted between the two modalities, but this article is not designed or powered to be a comparison of treatment efficacy.
A third possible way to reduce the radiation exposures associated with these therapies is to alter the imaging itself. MRI guidance has been employed as the imaging modality during percutaneous cryoablation of the kidney. Shingleton and colleagues described their experiences with MRI guidance of a PCA in 20 patients. 15 Although feasible, MRI guidance suffers from several limitations, including increased cost, the requirement of special equipment not available in most institutions, need for the patient to remain motionless for an extended period of time, and this technique is not an option in people with claustrophobia or with metallic implants.
US image guidance has also been successfully described. Bassignani et al. used US in three patients with four renal masses who underwent percutaneous cryoablation. All of the patients tolerated the procedure well, and there were no complications. 16 Compared with MRI, the US is relatively inexpensive, uses equipment routinely available in every hospital, and offers the advantage of real-time imaging. Unfortunately, the US also has drawbacks. The probes may be difficult to image, and larger patients are more difficult to image with US. In addition, some iso-echoic tumors may be difficult to image when using US guidance.
If CT is still utilized as the imaging modality, there are still several methods available to reduce the radiation exposure to the patient. The imaging should be confined as much as possible to the area of interest. Imaging at end expiration, the most consistent portion of the respiratory cycle allows the surgeon to limit the area of imaging. Instead of including large segments with several centimeters above and below the mass, we endeavor to limit the number of cuts on each limited CT scan to include only 1 cm above and below the tumor. In addition, the mAs and Kilovoltage Peak (KVP) may be reduced in tumors that are exophytic and easily identified on CT. In our own institution, we have demonstrated that by utilizing ultra low-dose protocols for CT-guided lung biopsies, the radiation dose during the biopsy was reduced by 95% without a decrease in technical success or patient safety. 17 We are currently working to adapt these low dose protocols to percutaneous ablations.
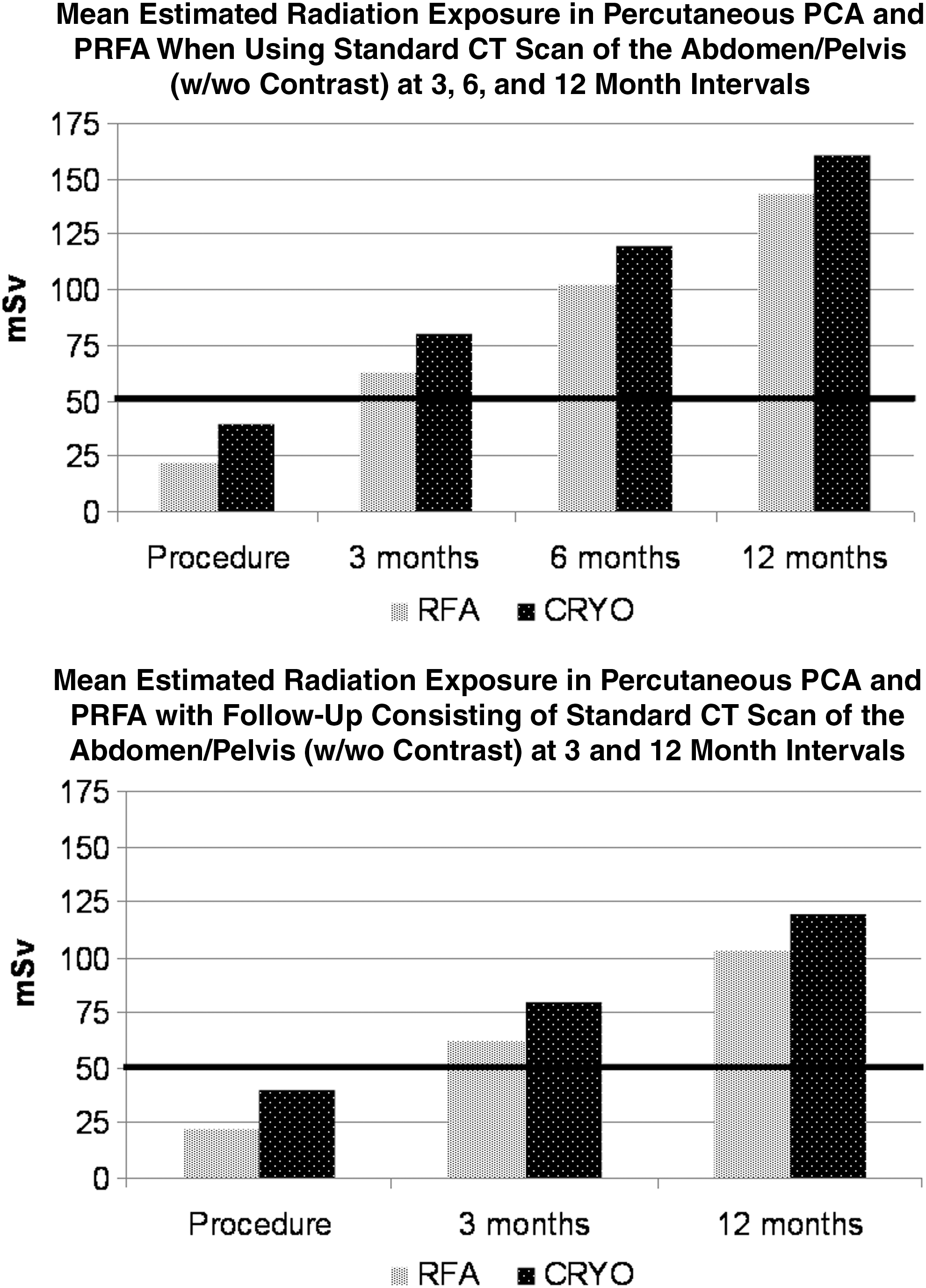
Finally, it should be considered that the follow-up modality and interval may significantly increase the radiation exposure in these patients. Most institutions routinely performed abdominal and pelvic CT with and without contrast at 3, 6, and 12 months. Utilizing the average radiation exposure from CT scans in our study, a patient undergoing percutaneous ablative therapy will exceed 50 mSv after performing the 3-month follow-up imaging. By 1 year if the same protocol was followed, the patients would have been exposed to more than double the amount of radiation considered safe by the United States Nuclear Regulatory Commission (Fig. 1). As a result of these compelling data, we have modified our follow up to substitute MRI imaging for all patients who are candidates. In patients who are not candidates for MRI, we routinely perform a CT abdomen with and without contrast at 3 months. Subsequent imaging is individualized with well-treated low-grade tumors that are potentially not being imaged for 12 months, while more aggressive (grades 3 and 4) and larger tumors (>3 cm) are imaged at 6-month intervals (Figs. 2 and 3). It is certainly important to obtain timely imaging to avoid risk of recurrence and progression, and future studies will be required to identify safe follow-up periods for specific risk profiles.
Procedure data.

Radiation exposure using different CT follow-up protocols.

Radiation exposure using MRI only for follow-up.
This study had several limitations. One limitation was that the number of scans used to biopsy the lesion and to displace adjacent structures was not included in the comparison, and, therefore, the actual radiation exposure may have been somewhat underestimated in these patients. This method of comparison was intentionally selected to enable a fair comparison of modalities independent of the earlier biopsy status, or the tumor location. Second, this study was a retrospective study and is subject to all the biases inherent in a retrospective study design. In addition, the actual radiation exposures used in follow up were not determined for all patients, but instead, a mean exposure calculated from 10 patients undergoing follow up was used for follow-up radiation dosage determinations. This method was selected, as the majority of patients in our series had outside imaging for follow up that did not allow exposure calculations. Despite this, our study represents the first study to determine cumulative radiation exposures in both percutaneous cryoablation and PRFA. Certainly, the knowledge and awareness of this radiation exposure represents the first step in taking measures to reduce these radiation exposures to patients treated with percutaneous ablative therapies. The results of this study also emphasize the importance of careful and thorough counseling of all patients undergoing CT-guided percutaneous ablative therapies and, in particular, emphasizes the importance of using these modalities cautiously in younger healthier patients who may have a long survival.
Conclusion
No earlier study has determined the radiation exposures in PCA and PRFA. Our study shows relatively high radiation exposures in both patient groups, particularly when follow-up studies are included in exposure calculations. Knowledge of the radiation exposure associated with these treatments and their follow-up imaging is essential for both surgeons and patients. These relatively high levels of radiation exposure are most concerning in young healthy patients who have the longest expected survival and subsequently, the greatest risk for secondary malignancy. The amount of potential radiation exposure should be considered when selecting between different techniques for renal preservation and discussed with patients when obtaining informed consent, so they can make an educated decision regarding their disease management.
Footnotes
Author Disclosure Statement
No competing financial interests exist.