
Abstract
Objective:
To compare the effective doses (EDs) associated with imaging modalities for follow-up of patients with urolithiasis, including stone protocol non-contrast computed tomography (NCCT), kidney, ureter, and bladder radiograph (KUB), intravenous urogram (IVU), and digital tomosynthesis (DT).
Methods:
A validated Monte–Carlo simulation-based software PCXMC 2.0 (STUK) designed for estimation of patient dose from medical X-ray exposures was used to determine the ED for KUB, IVU (KUB scout plus three tomographic images), and DT (two scouts and one tomographic sweep). Simulations were performed using a two-dimensional stationary field onto the corresponding body area of the built-in digital phantom, with actual kVp, mAs, and geometrical parameters of the protocols. The ED for NCCT was determined using an anthropomorphic male phantom that was placed prone on a 64-slice GE Healthcare volume computed tomography (VCT) scanner. High-sensitivity metal oxide semiconductor field effect transistors dosimeters were placed at 20 organ locations and used to measure organ radiation doses.
Results:
The ED for a stone protocol NCCT was 3.04±0.34 mSv. The ED for a KUB was 0.63 and 1.1 mSv for the additional tomographic film. The total ED for IVU was 3.93 mSv. The ED for DT performed with two scouts and one sweep (14.2°) was 0.83 mSv.
Conclusions:
Among the different imaging modalities for follow-up of patients with urolithiasis, DT was associated with the least radiation exposure (0.83 mSv). This ED corresponds to a fifth of NCCT or IVU studies. Further studies are needed to demonstrate the sensitivity and specificity of DT for the follow-up of nephrolithiasis patients.
Introduction
Concerns about medical radiation exposure have been raised, though the long-term risk is not easily quantifiable. Nevertheless, decreasing radiation exposure remains an important consideration.
With the inception of newer CT scanners and optimized software, lower radiation doses could have been achieved in the past while maintaining diagnostic accuracy for the imaging of nephrolithiasis. Furthermore, there have been a number of studies assessing “low dose” CT scans for the evaluation of calculi and renal colic. 3 –5 Niemann et al. report in a meta-analysis of studies evaluating low-dose NCCT a pooled sensitivity of 97% and specificity of 95% for the detection of urolithiasis, so that low-dose CT is considered the first-line imaging study in acute renal colic and should be preferred to a regular NCCT. 6
Digital tomosynthesis (DT) is a new technology based on conventional X-ray tomography that may reduce radiation exposure even further. With this technique, a series of low-dose projection images are acquired with a digital detector during a single sweep of the X-ray tube. The data are later reconstructed using computational software that can also remove overlying structures and provide indepth information about the structure of interest. 7 In comparison, conventional tomography requires multiple sweeps at different angles to focus at different depths.
The primary use of this new technology has been in chest radiography and breast imaging. 8 Lately, there have been two studies reporting its clinical use for the evaluation of urolithiasis. Mermuys and coworkers compared the ability to detect stones by DT and digital standard radiography combined with a zoomed-in shot of the pelvis using NCCT as a standard comparison. They concluded that DT was superior to digital radiography for the identification of renal stones but not for ureteral stones. 9 Wells et al. studied the diagnostic quality of an IVU performed with the technique of DT. 10 In their study, two uro-radiologists compared a traditional IVU with an IVU performed with DT. They found that 95.5% of the IVU with DT were of subjective diagnostic quality v 46.5% of the traditional IVUs. In addition, the dose of radiation (as assessed from the scanner) was lower for the IVU with DT and took less time.
We hypothesize that DT will expose patients to less ionizing radiation in comparison to a KUB with tomograms, IVU, or stone protocol NCCT. This is the first study comparing DT to standard follow-up imaging modalities.
Materials and Methods
An anthropomorphic male phantom (model 701-D; CIRS), which has been previously validated for human organ dosimetry, was used to determine the effective dose (ED) of an NCCT. 11 The phantom is 173 cm tall and weighs 73 kg. It is composed of 39 contiguous axial slices, with each being 25 mm thick. The slices have numbered locations representing anatomical locations of internal organs. A male phantom is used, because the male gonads receive higher radiation exposure than female gonads due to the superficial location of the testes. The only other significant difference for female phantoms occurs in evaluating doses for chest CT scans. A total of 20 high sensitivity metal oxide semiconductor field effect transistor (MOSFET) dosimeters (Model TN-1002RD; Best Medical) were placed in the phantom at specific organ locations. A total of three NCCTs were performed (GE 64 slice VCT scanner) at settings used in clinical practice at our institution for stone detection (120 kV, 700 mA, noise index 17.5, pitch 1.375, and total time exposure of 4.2 seconds). The performed scans used automatic tube current modulation. A total of 80 images were obtained with each CT with a slice thickness of 5 mm and a scan range from the top of the kidneys through the bladder. Each organ dose was multiplied by the tissue-weighting factor published by the International Commission of Radiological Protection in order to obtain the organ-specific equivalent dose. 12 The sum of doses was averaged to calculate the ED for the stone protocol NCCT.
ED from one KUB, KUB with tomograms, and IVU (Simulated X-ray system: “Digital Diagnost.”; Philips Healthcare) were estimated using PCXMC 2.0 (STUK), a validated Monte–Carlo simulation-based software designed for estimation of patient dose from medical X-ray exposures. 13 Due to the relatively small tube rotation angles involved, simulations were performed using a two-dimensional (2D) stationary field onto the corresponding body area of the built-in digital adult phantom, with actual kVp, mAs, and geometrical parameters of the protocols (Table 1).
KUB, kidney, ureter, and bladder radiograph; KVP, kilovolt penk; FID, focus to image distance.
The ED for DT was estimated using the PCXMC 2.0 (STUK) Monte–Carlo simulation-based software. 13 The DT protocol (Simulated X-ray system: “Definium 8000,” GE Healthcare) consists of two scouts (85 kV, 630 mA and 800 mA) of the upper and lower abdomen/pelvis and one tomogram (85 kV, 630 mA, 14.2° sweep angle, 17 slices, and 5.5 seconds of scan time). The Dose-Area Product (DAP) for each part of the protocol was read from the system console, which were 7.6, 6.0, and 27.0 dGy cm2, for the two scouts and tomogram, respectively. The DAP values were fed into the PCXMC software as machine output reference to calculate the total ED. Similar to the simulations done for the KUB and tomogram, due to the relatively small sweep angle of the DT, simulation was done with a 2D stationary field onto the corresponding body area of the digital phantom.
Results
The measured ED for a stone protocol CT is 3.04±0.34 mSv. The ED of a KUB is 0.63 mSv, and the ED of each tomographic image is 1.1 mSv. For an IVU or KUB with tomograms, a combined dose of 3.93 mSv was calculated, assuming a single scout KUB and three tomographic images. The ED for DT (two scouts and one tomographic sweep) was determined to be 0.83 mSv with the Monte–Carlo simulation (Fig. 1). The cost for a KUB with tomograms is double of a single KUB and similar compared with DT. An IVU study costs almost four times as much as a single KUB. A DT combined with bilateral renal sonograms is about five times of a single KUB. The cost of a renal stone protocol CT is four times the cost of an IVU.
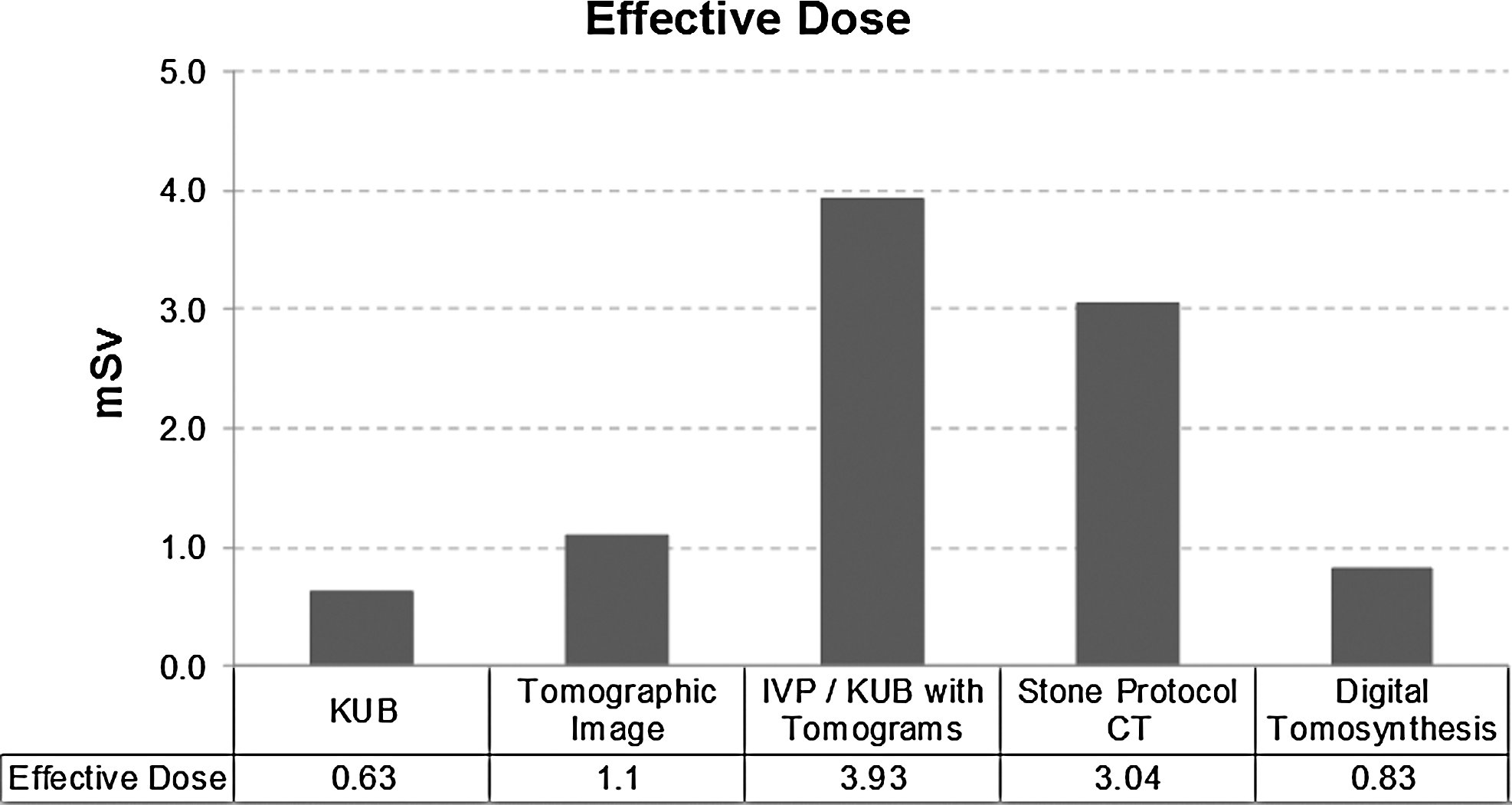
Effective doses of the different studies.
Discussion
As medically related radiation exposure has increased, so have concerns about its long-term effects. Annual per capita radiation exposure from medical sources has increased from an average 0.54 mSv in 1980 to 3.0 mSv in 2006. 14 The growth in CT usage has increased exponentially during this time, which is likely to be a strong contributing factor. 15
For the evaluation of patients with acute colic, NCCT is considered the gold standard and is widely employed. 6 As stated earlier, stone formers may receive multiple CTs in a short period with an average of 1.7 CTs performed after one acute stone episode. 2 Young recurrent stone formers with a long life expectancy may be particularly at risk for developing a malignancy due to accumulated radiation dose from repeated medical imaging.
“Low dose” stone protocol CTs have been introduced to reduce radiation exposure. 3,16 One technique involves decreasing the scanner tube current (mA), but ED is lowered at the expense of decreasing image quality. Especially in obese patients, small stones may be difficult to appreciate. 17,18 Different manufacturers and institutional variability in CT protocols preclude standardization of ED from CT. The CT protocol evaluated in the current study is the “low dose” renal stone protocol CT that is currently used at our institution. Our ED of 3.04 mSv is higher than some EDs reported in the literature for low-dose and ultra-low-dose CT protocols with EDs of 1.40–1.97 mSv and 0.5–0.7 mSv, respectively. 3,16 Notably, both studies used simulation models to achieve the EDs, whereas the ED for our institutional stone protocol CT was measured with a validated phantom model. 11 However, it is generally accepted that the term “low dose” CT refers to an NCCT with a dose of 3 mSv or less. 6
In our practice, NCCTs are often used in evaluating acute stone episodes. However, we have used KUB and tomograms to follow recurrent stone formers to assess for changes in their stone burden. The reason that we used KUB with tomograms v plain KUB was the increased sensitivity of tomograms to detect stones 19 and the assumption that the tomograms contributed only a small amount of radiation. Instead, the radiation exposure from one KUB with three tomograms greatly exceeded that from a KUB and even exceeded that from a stone protocol NCCT performed at our institution (with 3.93 mSv v 0.63 mSv and 3.04 mSv). The standard IVU at our institution is performed with the same protocol as a KUB with three tomograms, thus exposing patients to the same amount of radiation.
Digital tomosythesis may be an attractive substitute for a KUB and standard tomography for the follow-up of patients with nephrolithiasis. When combined with ultrasound, it may be an attractive substitute for IVU or NCCT. Instead of taking a KUB and multiple films or tomographic sweeps of the patient, only two digital scouts and a single sweep of the X-ray tube is required. This fully evaluates the kidney, and the digital tomogram provides all the data needed to make the coronal images.
Post-image processing allows for reconstruction of an arbitrary number of planes from the single acquisition sequence. This allows for generation of high-resolution images at different coronal depths or high-resolution “slices” that could potentially improve sensitivity for stone detection (Fig. 2). Similar to conventional tomography, it removes overlying structures and provides indepth information. 20 Clinically, it has been used in chest and breast imaging. 8,21 In our study, the ED of a DT (0.83 mSv) is lower than the ED of both NCCT and IVU or KUB with traditional tomography.

Comparison between KUB and digital tomosynthesis.
Mermuys and coworkers have described the use of DT for evaluating nephrolithiasis and compared the EDs for digital radiography and DT with 0.5 and 0.85 mSv, respectively. 9 They found better sensitivity for DT compared with digital radiography in the kidney, but only a 29% sensitivity for DT in the ureter. In this location, DT did not improve sensitivity. Overall, smaller calculi were especially difficult to detect, with a sensitivity of 36% for stones <2 mm, 54% for stones 2–5 mm in diameter, and 76% for stones >5 mm. This may be due to the fact that conventional radiography uses a separate film for the pelvis, thus having higher resolution—but also higher radiation—to detect distal ureter stones. However, the sensitivity of a KUB for diagnosing urolithiasis has been reported to be 45–58% overall, 22 –25 and DT exceeds this.
As with traditional tomography, DT has difficulties in identifying small stones (<2 mm) and ureteral stones. It is not a substitute for NCCT in the evaluation of renal colic or for surgical planning, but may still be valuable in the follow-up of recurrent stone formers and their stone burden. It appears to provide a higher amount of information compared with KUB with traditional tomograms for kidney stones, at similar costs, but with significantly lower radiation exposure. It has been proved in an early study on conventional tomograms that in 46% of patients, additional stones were seen in tomograms when compared with KUB, and in 8% of patients, stones were not seen in KUB but were identified in tomograms. 19
The clinical role of DT has still to be determined in comparative studies and in sensitivity comparisons between DT and ultrasound in contrast to IVU and/or low-dose NCCT. However, one of the other concerns with the application of low-dose CTs is cost. The cost of DT is the same as KUB with conventional tomograms and cheaper than an IVU at our institution. Both are significantly cheaper than an NCCT (about sevenfold). In our clinical practice, we are now obtaining both a renal ultrasound and DT (instead of KUB) for routine post-op visits after uncomplicated ureterorenoscopy and percutaneous nephrolithotomy. This combination is still significantly less expensive than NCCT and comparable in cost to obtaining an IVU. For annual follow-up of recurrent stone formers, we simply get a DT (instead of KUB and tomograms).
There are a few limitations to this study. This is a single-institution study and given the wide variability in equipment and protocols at other institutions, it is difficult to generalize our results. These results cannot easily be extrapolated to obese and pediatric patients, as our phantoms were available in only one standard size (with a normal weight body mass index of 24.4 kg/m2). We also used different methods of modeling radiation exposure between exams. The ED of DT and KUB with tomograms were calculated from Monte–Carlo simulation based software, while the stone protocol NCCT ED was calculated from an anthropomorphic male phantom utilizing MOSFETs. Both these are validated methods that are used to calculate ED. These methods are superior to any other kind of dose estimations (i.e., in animal models). 11,13 Due to the low applied doses of either KUB or, in particular, DT, MOSFETs were not effectively able to evaluate organ-specific doses.
Conclusions
Cumulative radiation dose is an important consideration in the nephrolithiasis patient population. Understanding radiation dose is necessary to make informed decisions regarding imaging techniques in these patients and for counseling patients about the relative risks from radiation exposure. IVU or KUB with tomograms exposes patients to more radiation than low-dose NCCT. DT, however, has a lower ED than all of these techniques. For this reason, DT may play a significant role in future surveillance of nephrolithiasis patients.
Footnotes
Acknowledgments
This work was supported in part by a Ferdinand Eisenberger grant of the Deutsche Gesellschaft für Urologie (German Society of Urology), ID NeA1/FE-11 (Andreas Neisius). Gastón M. Astroza has been supported by the Endourological Society and Cook Urological. The authors thank Matvey Tsivian for a critical reading of this article.
Disclosure Statement
Dr. Lipkin is a consultant for Boston Scientific and speaker for Lumenis; Dr. Ferrandino is a proctor for Intuitive Surgical. For the remaining authors, no competing financial interests exist.