
Abstract
Purpose:
To evaluate meperidine-sparing effect of intravenous (IV) paracetamol in patients undergoing percutaneous nephrolithotomy (PCNL).
Patients and Methods:
One hundred patients who underwent PCNL were randomized to paracetamol (n=50) and placebo (n=50) groups. Patients received 100 mL of physiologic saline with or without 1 g IV paracetamol every 8 hours after PCNL up to 24 hours in the paracetamol and placebo groups, respectively. Patients in both groups received intramuscular meperidine in case of unrelieved pain. The visual analog scale (VAS) was used to evaluate pain intensity scores in the postoperative period. Total meperidine consumption, mean VAS score in the first 6 and 24 hours, demographic variables, operative variables, and side effects were recorded.
Results:
The mean VAS pain intensity scores at 6 and 24 hours were 50.22 and 41.32 mm in the paracetamol and 75.29 or 65.5 mm in the placebo group (P<0.001). The mean consumed meperidine dose was 54.40 mg and 77.60 mg in the paracetamol and placebo groups, respectively (P<0.001).
Conclusion:
In this study, IV paracetamol significantly reduced total meperidine consumption and pain intensity scores compared with placebo. IV paracetamol can be an effective and safe part of multimodal analgesia regimes for postoperative pain management after PCNL.
Introduction
P
Traditionally, the common practice in postoperative pain management is prescribing opioid analgesics. Extensive use of these drugs, however, leads to high rates of side effects including ventilatory depression, drowsiness and sedation, postoperative nausea and vomiting, pruritus, urinary retention, ileus and constipation, and consequently longer hospital stay and higher overall costs. 3 Applying multimodal or balanced analgesic techniques decreases the total opioid dosage. 4 Intravenous (IV) paracetamol (acetaminophen) is a nonopioid, centrally acting analgesic without serious unwanted side effects in therapeutic doses. 5,6
Several authors have described some methods to decrease post-PCNL pain management such as tubeless PCNL, local anesthetic infiltration, and multimodal analgesia. 7 –9 To our knowledge, this is the first randomized clinical trial evaluating the opioid-sparing effect of IV paracetamol in patients undergoing PCNL.
Patients and Methods
This study was a single-center double-blind, randomized, controlled trial to compare IV paracetamol and placebo in pain control after PCNL. Written informed consent was obtained from all patients. The study was approved by the ethics committee of our center. Patients aged 18 years old or older with otherwise American Society of Anesthesiologists (ASA) risk class I (but ASA II because of the stone) were included in the study. Exclusion criteria were pregnancy and lactation, drug and alcohol abuse, history of any allergy to acetaminophen or opioids, history of hepatic (liver transaminase level two times more than normal limits) or renal failure (serum creatinine >1.5 mg/dL), bleeding tendency, consumption of monoamine oxidase inhibitors or discontinuing them over the past 2 weeks, painful physical conditions that may affect pain assessment after PCNL, any psychiatric or medical condition impairing communication, and use of nonsteroidal anti-inflammatory drugs (NSAIDs) or other analgesic agents less than 12 hours before prescribing the study medications.
All patients underwent physical examination and laboratory evaluation including complete blood cell count and differentiation, serum creatinine, blood urea nitrogen, liver function tests, and coagulation profile 1 day before and after the surgery. Stone burden was evaluated with abdominopelvic CT. All PCNL procedures were performed under the supervision of one attending endourologist.
The anesthesia protocol used in all patients included a muscle relaxant (atracurium: 0.5 to 0.6 mg/kg), an opioid analgesic (fentanyl: 5 to 10 mg/kg), Nesdonal (thiopental): 5 to 7 mg/kg, and anesthesia maintenance with inhalation of isoflorane 0.8 to 1 MAC. No opioid analgesics were used after extubation in the anesthesiology protocol.
Interventions
Enrolled patients were randomly allocated to the placebo or paracetamol group using the balanced block randomization method. After the operation, patients were observed in the postanesthesia care unit for 30 to 60 minutes, and then transferred to the ward. In the paracetamol group, patients received 100 mL of physiologic saline and 1 g of IV paracetamol 30 minutes after extubation and every 8 hours until 24 hours. In the placebo group, patients received only 100 mL of physiologic saline 30 minutes after extubation and every 8 hours for 24 hours (four times overall). Patients in both groups received 25 to 50 mg intramuscular meperidine based on the patient demand (up to 200 mg per day).
The randomization schedule was prepared by an assistant blinded to the study. Serums containing placebo and paracetamol, identical in color and appearance, were prepared by an assistant and administered by nursing personnel blinded to the study.
Outcome measurement
To record pain perception, the 100-mm visual analog scale (VAS) was used 30 minutes, 1, 4, 8, 12, 16, 20, and 24 hours after extubation in both groups. The VAS score at 30 minutes was considered as the baseline before paracetamol administration. Moreover, based on each patient's demand for opioid analgesics, pain perception was evaluated. The analgesic efficacy was assessed by the mean VAS pain intensity scores over the first 6 hours and first 24 hours after extubation. Total meperidine dose consumed for each patient was recorded. Adverse side effects including ventilatory depression, drowsiness and sedation, postoperative nausea and vomiting, pruritus, ileus, and constipation were also recorded in a specially designed form. Patients' demographic information, history of surgery at the same site, stone burden, number of tracts, duration of surgery, and decrease in hemoglobin as the indicator of blood loss were also collected.
Data analysis was performed using repeated measure analysis of variance (ANOVA) to compare dependent continuous variables with normal distribution and nonparametric tests for the others.
Results
One hundred and fifty-three consecutive patients were assessed for eligibility; initially, 51 patients were excluded for a variety of reasons and 2 patients did not complete the study. Finally, 100 patients remained in the study. No deviation from the protocol was seen. There were 34 men and 16 women in the paracetamol group and 40 men and 10 women in the placebo group. Age, body mass index (BMI), stone size, and operative time were not significantly different between the two groups (Table 1). Single tract and multitract PCNL was performed in 98 and 2 patients (one patient in each group), respectively.
SD=standard deviation; BMI=body mass index.
Meperidine use had no significant association with age and BMI, but it was significantly different between men and women. Meperidine consumption in women was 18% more than men (P<0.05). Total meperidine use in the paracetamol group was less than the placebo group (P<0.001). Multivariate analysis adjusted for sex, BMI, stone burden, duration of surgery, and hemoglobin depletion after surgery showed similar results (P<0.001).
Baseline VAS pain intensity score at 30 minutes was not significantly different between the groups. VAS pain intensity scores had a statistically significant correlation with total meperidine consumption (P<0.001). As shown in Table 2, a statistically significant difference (P<0.001) was seen between VAS distribution in the paracetamol and placebo groups. Table 3 shows that the mean VAS pain intensity scores at 6 and 24 hours were higher in the placebo group than the paracetamol group (P<0.001).
P value=< 0.001.
VAS=visual analog scale.
SD=standard deviation; VAS=visual analog scale.
Repeated measures ANOVA showed no statistically significant difference between paracetamol and placebo groups in the meperidine consumption pattern over time, in the first 6 and 24 hours after the operation. The longer time passed after the operation, the less meperidine was needed in both groups. The amount of reduction in both groups was comparable with no interaction between the groups (Fig. 1).
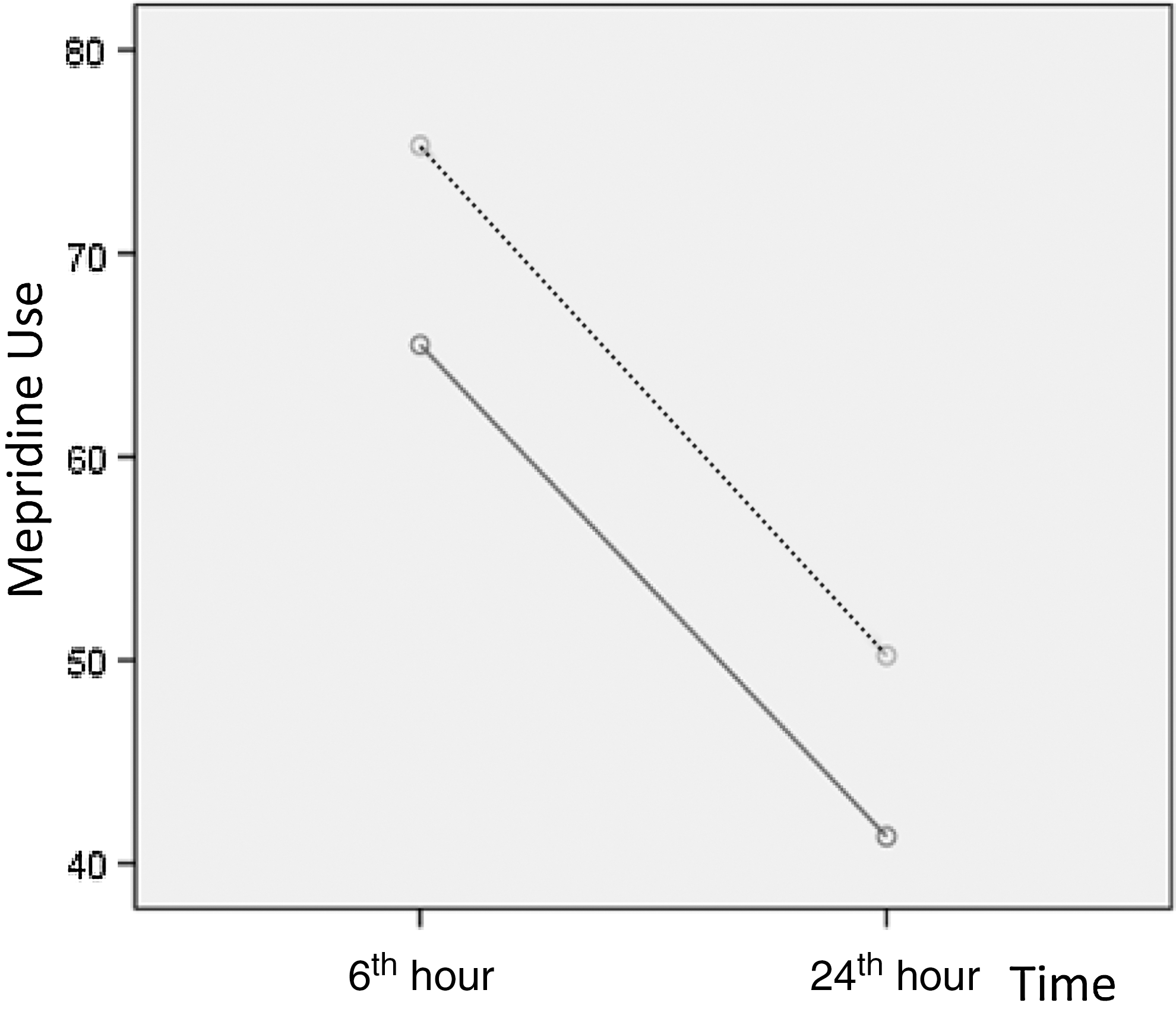
Meperidine consumption in paracetamol and placebo groups during the first postoperative day. Dotted line=total meperidine consumption dose in the placebo group; gray line=total meperidine consumption dose in the paracetamol group.
In the paracetamol group, two patients experienced nausea that was self-limited. In the placebo group, six patients had nausea and vomiting and four of them needed to be treated with metoclopramide. There was not any significant rise in the postoperative serum creatinine and liver transaminase levels in the patients.
Discussion
Since the first description of PCNL in 1976, treatment of patients with renal calculi has evolved, and PCNL has become the standard surgical treatment for patients with large renal stones (>2 cm). 10 Postoperative pain could cause considerable morbidity including endocrine, ventilator, and gastrointestinal problems. 11 It is the most significant cause of preoperative anxiety and has a strong impact on the recovery period. 1 Several authors have described the role of the presence and size of the nephrostomy tube as a main source of postoperative pain in patients undergoing PCNL. 12 Tubeless PCNL has been associated with decreased postoperative hospital stay, analgesic requirement, health costs, and shortening of the recovery period. 7 When the nephrostomy tube cannot be dispensed, reduced size of the tube could be associated with decreased pain severity. Previous studies have shown that patients with a 10F nephrostomy tube had lower VAS pain scores compared with patients with a 22F tube. 13
Several authors have suggested some analgesic methods for management of postoperative pain after PCNL such as local instillation of analgesic agents, multimodal analgesia regime, and a combination of local levobupivacaine infiltration to the nephrostomy tract and IV paracetamol. 7 –11 Haleblian and colleagues 10 reported a randomized prospective trial evaluating the impact of bupivacaine infiltration of the nephrostomy tract in PCNL patients. They showed a trend toward decreased postoperative narcotic use in patients receiving bupivacaine. Gokten and coworkers 11 evaluated levobupivacaine infiltration to the nephrostomy tract combined with intravenous paracetamol for postoperative analgesia in PCNL patients, and showed that the combined regime is safe and efficacious.
To our knowledge, this is the first study focused on the opioid-sparing effect of IV paracetamol in patients undergoing PCNL. Our findings showed that administration of IV paracetamol after PCNL not only reduced meperidine consumption significantly, but also led to significant reduction of pain intensity scores, especially in the first 6 hours.
There is an ever-increasing tendency to use multimodal or balanced approaches (a combination of lower doses of opioid analgesics with nonopioid analgesics) in the management of postoperative pain. 4,13 Because of the minimal side effects of paracetamol and the recent production of its IV preparation, it is gaining increasing popularity in multimodal analgesia regimes. 3,14 Several articles have compared different NSAIDs, paracetamol, and proparacetamol (paracetamol prodrug) with different types of opioid analgesics in the management of postoperative pain, and mainly indicated that the combination of opioid with nonopioid analgesics is supported.
In a well designed meta-analysis of randomized controlled trials by Remy and associates, 15 the effect of acetaminophen on morphine consumption and side effects after major surgeries was evaluated. They demonstrated that the combination of acetaminophen and morphine significantly reduced consumption of morphine but did not change the incidence of morphine side effects in the postoperative period. Toms and colleagues 16 in a Cochrane review of single dose oral paracetamol (acetaminophen) for postoperative pain in adults evaluated 51 studies. They concluded that single-dose oral paracetamol produced efficient analgesia in more than half of patients, especially in the first 4 hours after the surgery with few side effects of which the majority were minor. Bektas and coworkers 17 performed a well-designed detailed triple-blind trail to compare the analgesic efficacy of single-dose 1 g IV paracetamol, single-dose 0.1 mg/kg IV morphine, and placebo in patients presenting to an emergency department for renal colic. They analyzed 146 consecutive patients and demonstrated that mean reduction of pain intensity scores was significantly higher in paracetamol and morphine groups compared with placebo but was not different between paracetamol and morphine groups. They also found 45% of patients in the paracetamol, 49% in morphine, and 67% in the placebo group needed a rescue drug because of unrelieved pain after 30 minutes of the first injection. In conclusion, they stated paracetamol is an efficient and safe treatment in patients presenting to an emergency department for renal colic.
Our results reflecting opioid-sparing effects of IV paracetamol were comparable to those of other studies. 18 –21 In our study, meperidine consumption and pain intensity scores were significantly different in the paracetamol and placebo groups when adjusted for age, BMI, stone burden, and operative time. Our results showed that paracetamol reduces pain intensity scores and meperidine consumption dose in the mentioned subgroups. Totally, meperidine consumption in women was more than men. This could be explained by gender differences in pain perception. Several authors have reported that men and women are different in response to pain, with increasing pain sensitivity among women. 22 In similar situations, women complain of severe pain more often than men. 23 Cepeda and Carr 24 evaluated postoperative pain scores and the dose of morphin required for pain relief in male and female patients after various surgery types. They reported higher pain intensity scores and a greater need for morphine in women.
Although pain intensity scores were significantly lower in the paracetamol group, patterns of pain alteration were similar in both groups (Fig. 1). In addition, although the cost of IV paracetamol is higher than its opioid counterparts, a few doses of this medication can lead to significant reduction in pain intensity scores. Because of the low frequency of unwanted adverse effects in our study, we were unable to evaluate and analyze effects of IV paracetamol on meperidine side effects, but other studies have demonstrated a decrease in opioid side effects in the multimodal management of postoperative pain. The subjective nature of the pain was another limitation of this study. Moreover, because of ethical considerations, a strict protocol could not be used for opioid consumption in case of unrelieved pain.
Conclusion
IV paracetamol, in combination with opioid analgesics, can be an effective and safe part of a multimodal approach to postoperative pain management in patients undergoing PCNL. Further studies are needed to assess the effects of IV paracetamol on overall costs and patient satisfaction.
Footnotes
Disclosure Statement
No competing financial interests exist.