
Abstract
Purpose:
To describe our bladder neck dissection during robot-assisted radical prostatectomy (RARP), to describe the degrees of robot-assisted bladder neck preservation (R-BNP) we have encountered, and to determine the effect of increasing R-BNP on postoperative continence and positive surgical margin (PSM) rates.
Patients and Methods:
We performed a retrospective analysis of 599 patients who underwent robot-assisted radical prostatectomy (RARP) by a single surgeon (DIL). All bladder neck dissections were graded between 1 and 4; higher grades corresponded to an increasing degree of robot-assisted bladder neck preservation (R-BNP). After grouping patients by R-BNP grade, postoperative continence and positive surgical margin (PSM) rates were compared. The association between R-BNP and continence was also assessed using multivariate binary logistic regression models.
Results:
Similar outcomes were seen for two definitions of continence (0 pads per day [ppd]; 0 ppd or security pad, respectively). A higher proportion of patients were continent at 3 months postoperatively who received grade 4 compared with grade 1 (P=0.043; P=0.001) and grade 2 (P=0.006; P=0.009); and grade 3 compared with grade 1 (P=0.048; P=0.002) and grade 2 (P=0.009; P=0.030) R-BNP. There was no difference between grade 1 and 2 (P=0.541; P=0.064), and grade 3 and 4 (P=0.898; P=0.584) R-BNP. At 1 year postoperatively, there was no difference among the four groups in continence rate (P=0.771; P=0.411). R-BNP was an independent predictor of continence at 3 months (odds ratio [OR] [95% confidence interval (CI)]=1.33 [1.06–1.67]; OR [95% CI]=1.45 [1.1–1.82]), but not at 1 year (OR [95% CI]=1.07 [0.82–1.39]; OR (95% CI)=1.30 [0.92–1.85]). There was no difference among the four groups in PSM rates (P=0.946).
Conclusions:
R-BNP is a graded, rather than all-or-none outcome. An increasing degree of R-BNP is associated with an earlier return to continence, without compromising oncologic outcomes.
Introduction
R
Robot-assisted radical prostatectomy (RARP) has been increasingly used for treatment of patients with clinically localized prostate cancer. 9 Advantages of robot-assisted surgery include high definition, magnified, and three-dimensional vision, wristed instrumentation, and an ergonomically advantageous interface. RARP, however, is technically challenging and associated with a steep learning curve. 10 Bladder neck dissection (BND) is considered to be one of the hardest portions of RARP in which to obtain proficiency. 11 Thiel and associates 12 demonstrated that operative times for BND increased over the first 50 cases and were slow to improve thereafter. The absence of tactile sensation of the prostate and urethral catheter during RARP makes identification and dissection of the BN particularly difficult for the robotic novice. 13 Precision is critical during BND, because too distal a dissection may compromise oncologic control by leaving residual prostatic tissue, while too proximal a dissection may leave a large BN necessitating time-consuming bladder neck reconstruction (BNR). BNP during RARP (R-BNP) has also been suggested to be associated with an earlier return to continence, while having a limited role in long-term return to continence. 14,15
There are three major objectives of this study: First, to describe our consistent BND technique that allows for maximal R-BNP without compromising oncologic control and minimizing the need for BNR; second, to describe the typical degrees of R-BNP that we have encountered; and third, to determine the effect of increasing degree of R-BNP on continence rates at 3 months and 1 year postoperatively.
Patients and Methods
Retrospective chart review
Charts for 599 patients who underwent RARP by a single surgeon (DIL) at our institution between January 2008 and December 2009 were retrospectively reviewed. In each case, R-BNP was performed exclusively by DIL, and the surgical technique for RARP remained consistent throughout the study interval. Operating room (OR) time was defined as the number of minutes elapsed between initial incision and closure. Postoperative continence, which was assessed at 3 months and 1 year postoperatively, was defined in two ways: 0 pads per day (ppd); and 0 ppd or security pad.
Surgical technique
After transperitoneally entering the space of Retzius, incising the endopelvic fascia, and stapling the dorsal venous complex, the BND is performed. A 30-degree down lens, Maryland bipolar grasper, permanent cautery spatula, and ProGrasp forceps (Intuitive Surgical, Sunnyvale, CA) is used in the camera, left, right, and fourth robotic arms, respectively. Energy settings for both monopolar and bipolar current are 35 W.
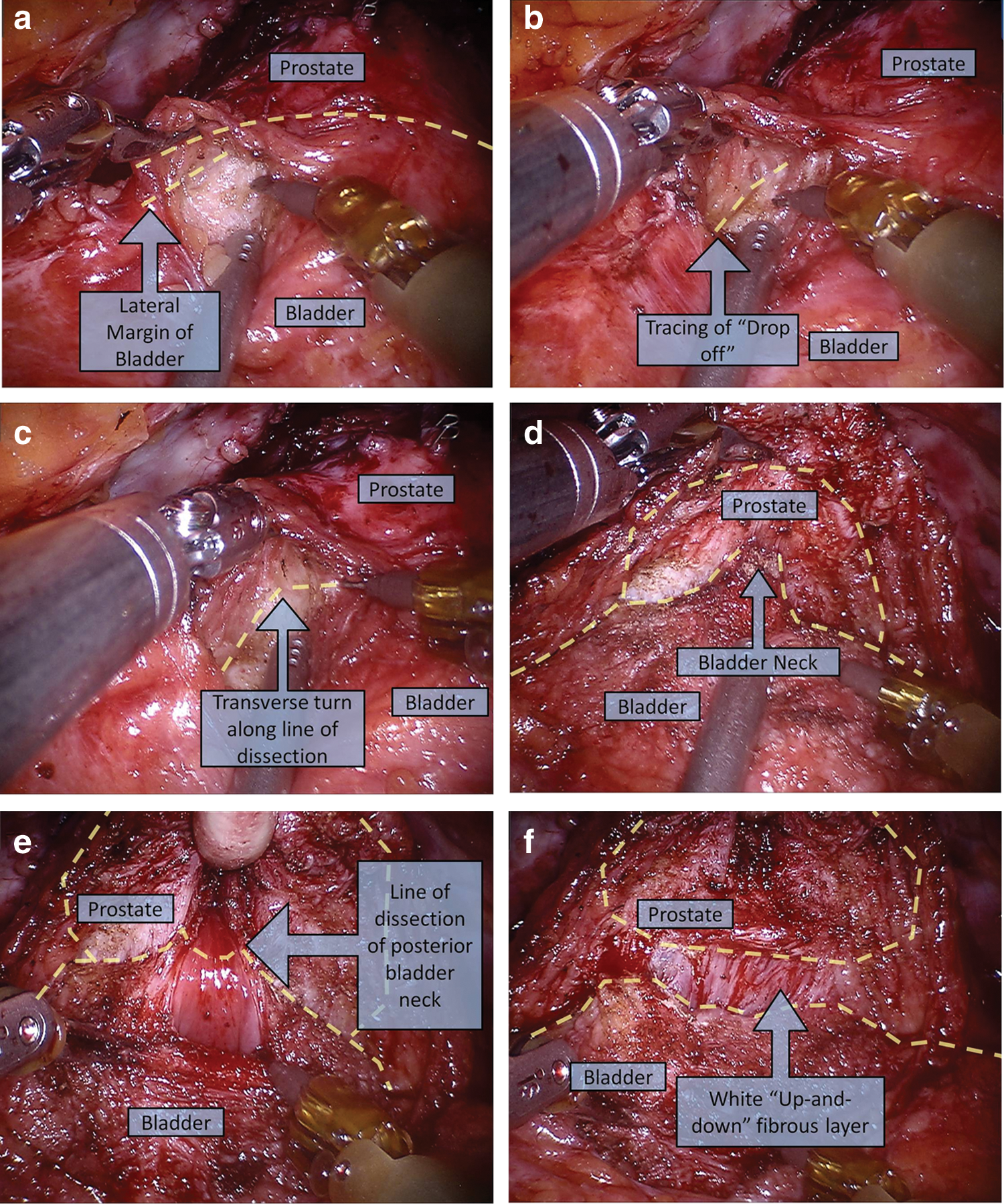
BND is started at the perivesical fat overlying the lateral bladder wall, 2 cm proximal and 2 cm lateral to the midpoint of the BN (Fig. 1a). The BN location can be estimated by in-and-out movement of the Foley catheter with the balloon inflated. This step becomes less necessary with increasing experience. The Maryland bipolar grasper is used to lift a veil of overlying perivesical fat laterally, while the spatula is used to dissect down through the adipose tissue layer to the outer detrusor wall with blunt and cautery dissection. It is important to maintain the tissue plane along the detrusor muscle until reaching the lateral edge of the bladder, which can be appreciated by a dramatic “drop-off” as the posterior aspect of the bladder turns underneath the BN (Fig. 1b).
Key steps of robot-assisted bladder neck preservation:
Next, the lateral aspect of the bladder wall is dissected toward the prostate. This portion of the procedure is facilitated by gentle downward countertraction on the bladder with the suction device provided by a bedside assistant. On reaching the prostatovesical junction, a difference between the firm prostate and the elastic bladder can be appreciated. At this junction, the dissection plane takes a transverse angle toward the contralateral side of the bladder (Fig. 1c), and the bladder is literally peeled off the anterior prostate. The same dissection is repeated on the contralateral bladder wall. On completion, the two anterolateral dissections should converge on the BN (Fig. 1d). When complete BNP is desired, this dissection plane will lead down to the BN and prostatic urethra. When a wider dissection plane is desired, however, a cuff of bladder can be left on the prostate to ensure a larger margin.
After the anterior vesicourethral junction is opened, the urethral catheter balloon is deflated and the tip of the catheter is delivered to the ProGrasp, which is retracted to a level above the symphysis pubis. Countertraction is created by securing the drainage end of the catheter to the bedside with a hemostat. The posterior BN is meticulously sculpted using monopolar cautery via the spatula with intermittent sweeping motions. When dissecting the posterior BN (Fig. 1e), it is important to maintain adequate thickness on the inferolateral edges of the bladder. This is achieved by turning upward around the posterior bladder wall edges before complete transaction. In addition, it is important to examine for a median lobe. Often, the presence of a median lobe is suggested by lateral deviation of the Foley balloon from the midline at the outset of the dissection. If a median lobe is present, the posterior BN is divided at a point about one-third of the way up on the median lobe to preserve some posterior BN tissue. Usually at this point, there is some detrusor that will be thick enough to hold the vesicourethral anastomotic sutures. When posterior BND is performed properly, there will be little posterolateral attachment left. With some blunt downward retraction on the bladder, a whitish “up-and-down” fibrous layer, which signifies the complete detachment of the bladder from the prostate, is appreciated (Fig. 1f ). Dividing this layer in a horizontal fashion allows visualization of the vas deferens and seminal vesicles.
In all cases, the maximal amount of R-BNP based on preoperative evaluation and intraoperative findings, is performed. Each R-BNP is assigned a grade based on the degree of BNP (Fig. 2a–d).
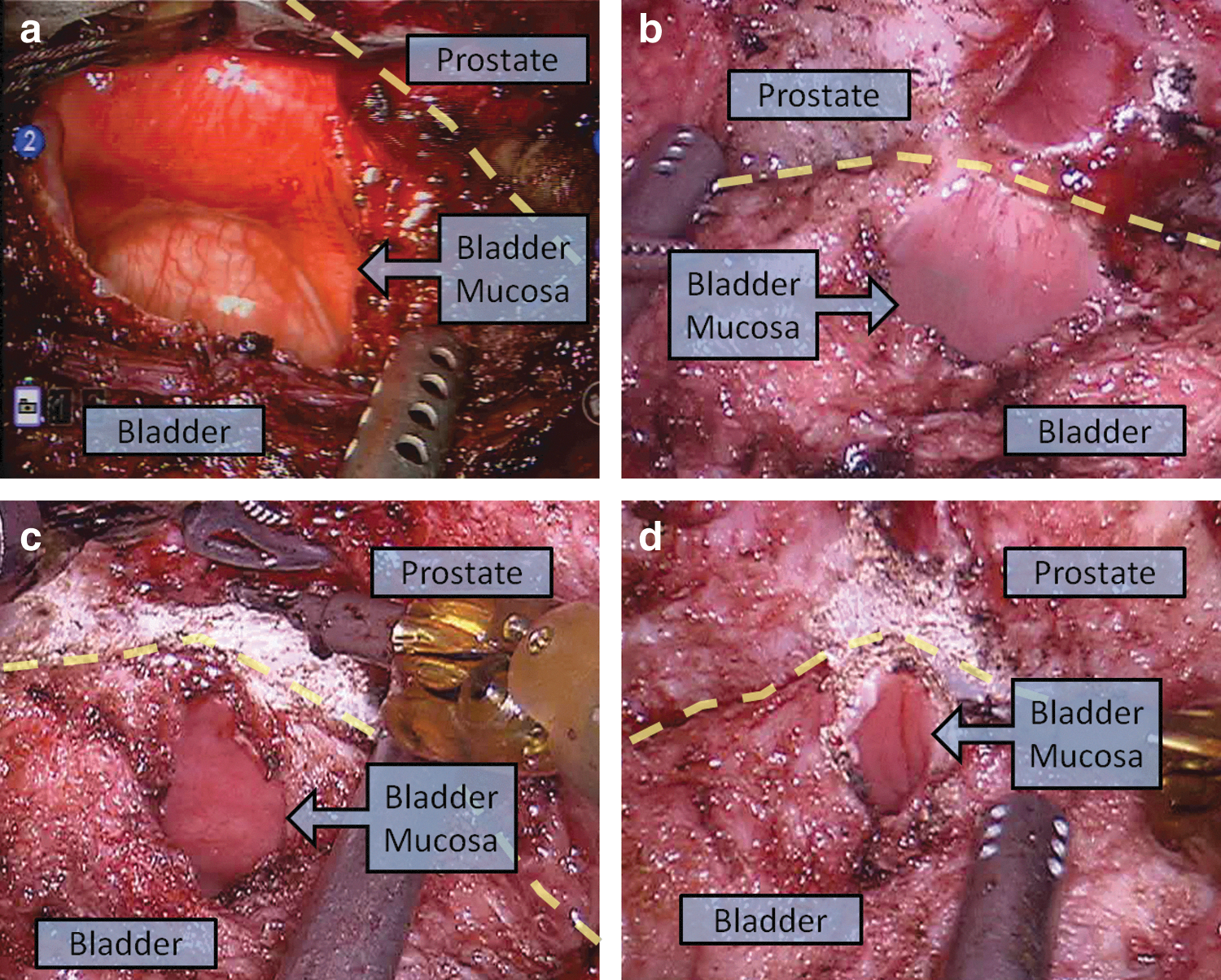
Dotted line separates prostate and bladder.
Statistical analysis
Statistical analyses were conducted after grouping patients chronologically into quartiles and also according to the degree of R-BNP received. Approximately normal variables were compared using a one-way analysis of variance test, and categorical variables were compared using a two-tailed chi-square test. In addition, the association between R-BNP and postoperative urinary continence rates at 3 months and 1 year were assessed using multivariate binary logistic regression models that also included age, body mass index (BMI), prostate weight, and preoperative American Urological Association Symptom Score (AUASS). In all cases, P<0.05 was considered to be statistically significant. Statistical analyses were conducted with Minitab 16 (Minitab Inc., State College, PA).
Results
Grade 1 R-BNP was performed in 18/599 (3.0%), grade 2 R-BNP was performed in 85/599 (14.2%), grade 3 R-BNP was performed in 235/599 (39.2%), and grade 4 R-BNP was performed in 261/599 (43.6%). Perioperative characteristics according to chronologic quartiles are shown in Table 1. There was no difference in the proportion of patients who received grade 1 (P=0.226), grade 2 (P=0.510), grade 3 (P=0.078), and grade 4 R-BNP (P=0.397) based on when RARP was performed. Also, there was no difference in rate of positive surgical margins (PSM) (P=0.272), and postoperative urinary continence rates (0 ppd; 0 ppd or security pad, respectively) at 3 months (P=0.562; P=0.083) and 1 year (P=0.964; P=0.793).
Two-tailed chi-square test of Quartile 1–4.
R-BNP=robot-assisted bladder neck preservation; PSM=positive surgical margin; ppd=pads per day.
Preoperative characteristics according to the degree of R-BNP are shown in Table 2. There was no significant difference among the four groups in preoperative mean age (P=0.495), BMI (P=0.111), AUASS (P=0.203), and serum prostate-specific antigen (PSA) (P=0.279). There was no significant difference in the proportion of patients with a diagnosis of clinical stage T1 (P=0.505) and T2 (P=0.290), and biopsy Gleason score 6 (P=0.369) and 7 (P=0.689) among the four groups. Comparison of patients with a preoperative diagnosis of clinical stage T3, and biopsy Gleason score 5, 8, and 9 among the four groups were deferred because of the limited number of patients in each category.
One-way analysis of variance test of Grades 1–4; bTwo-tailed χ2 test of Grades 1–4; cTwo-tailed chi-square test of Grades 1–4 not performed as multiple cells with expected counts less than 5.
SD=standard deviation; BMI=body mass index; AUASS=American Urological Association Symptom Score; PSA=prostate-specific antigen.
Operative and postoperative characteristics according to the degree of R-BNP are shown in Table 3. There was a significant difference among the four groups in mean OR time (P<0.001). Grade 1 needed a longer mean OR time than grade 2 (P=0.001), grade 2 needed a longer mean OR time than grade 3 (P=0.038), and grade 3 needed a longer mean OR time than grade 4 (P=0.042) R-BNP. There was a significant difference among the four groups in mean estimated blood loss (EBL) (P=0.018). Grade 1 was associated with a higher mean EBL than grade 2 (P=0.031) and grade 4 (P=0.008), and grade 3 was associated with a higher mean EBL than grade 4 (P=0.024) R-BNP. There was a significant difference among the four groups in the proportion of patients noted to have a median lobe (P<0.001). The proportion of patients with a median lobe was higher in those who underwent grade 1 compared with grade 4 (P=0.003), grade 2 compared with grade 3 (P=0.007) and grade 4 (P<0.001), and grade 3 compared with grade 4 (P<0.001) R-BNP.
=one–way analysis of variance test of Grades 1–4; b=two–tailed chi-square test of Grades 1–4; c=two–tailed chi-square test of Grades 1–4 not performed because of insufficient counts; d=% of total positive margins occurring at base.
=one–way analysis of variance test of Grades 1–4, Grade 1 and 2, Grade 1 and 3, Grade 1 and 4, Grade 2 and 3, Grade 2 and 4, and Grade 3 and 4, respectively; **=two–tailed chi-square test of Grades 1–4, Grade 1 and 2, Grade 1 and 3, Grade 1 and 4, Grade 2 and 3, Grade 2 and 4, Grade 3 and 4, respectively; ***=two–tailed chi-square test of Grades 1–4, and Grades 2–4, respectively.
Mean follow-up±SD (mos).
SD=standard deviation; PSM=positive surgical margin; ppd=pads per day.
There was a significant difference among the four groups in mean prostate weight (P<0.001). Grade 1 was associated with a higher mean prostate size than grade 4 (P<0.001), grade 2 was associated with a higher mean prostate size than grade 3 (P=0.004) and grade 4 (P<0.001), and grade 3 was associated with a higher mean prostate size than grade 4 (P<0.001) R-BNP. There was no significant difference among the four groups in mean length of hospital stay (P=0.949), and the proportion of patients with PSM (P=0.946). There was no significant difference in the proportion of patients with pathological stage T2 (P=0.593) and T3 (P=0.593), and pathologic Gleason score 6 (P=0.557) and 7 (P=0.532) among the four groups. Comparisons of patients with a postoperative diagnosis of pathologic Gleason score 8 and 9 among the four groups were deferred because of the limited numbers of patients in each category.
Similar outcomes were found for both definitions of continence (0 ppd; 0 ppd or security pad, respectively). At 3 months postoperatively, there was a significant difference in the proportion of patients who were continent among the four groups (P=0.008; P=0.001). A higher proportion of patients were continent at 3 months postoperatively who received grade 4 compared with grade 1 (P=0.043; P=0.001) and grade 2 (P=0.006; P=0.009), and grade 3 compared with grade 1 (P=0.048; P=0.002) and grade 2 (P=0.009; P=0.030) R-BNP. There was no significant difference between grades 1 and 2 (P=0.541; P=0.064), and grades 3 and 4 (P=0.898; P=0.584) R-BNP. At 1 year postoperatively, there was no significant difference in the proportion of patients who were continent among the four groups (P=0.771; P=0.411).
Multivariate binary logistic regression models for urinary continence are shown in Table 4. At 3 months postoperatively, age (OR [95% CI]=0.95 [0.92–0.97]; OR [95% CI]=0.96 [0.94–0.99]), preoperative AUASS (OR [95% CI]=0.97 [0.94–1.00]; OR [95% CI]=0.97 [0.94–0.99]), and R-BNP grade (OR [95% CI]=1.33 [1.06–1.67]; OR [95% CI]=1.45 [1.15–1.82]) were significant predictors of urinary continence (0 ppd; 0 ppd or security pad, respectively). At 3 months postoperatively, however, BMI (OR [95% CI]=0.97 [0.93–1.01]; OR [95% CI]=0.98 [0.94–1.02]) and prostate weight (OR [95% CI]=1.00 [0.99–1.01]; OR [95% CI]=1.00 [0.99–1.01]) were not significant predictors of urinary continence (0 ppd; 0 ppd or security pad, respectively). At 1 year postoperatively, age (OR [95% CI]=0.93 [0.90–0.96]; OR [95% CI]=0.92 [0.88–0.97]) and preoperative AUASS (OR [95% CI]=0.96 [0.93–0.99]; OR [95% CI]=0.94 [0.90–0.98]) were significant predictors of urinary continence (0 ppd; 0 ppd or security pad, respectively). At 1 year postoperatively, however, BMI (OR [95% CI]=0.99 [0.94–1.04]; OR [95% CI]=1.00 [0.94–1.08]), R-BNP grade (OR (95% CI]=1.07 [0.82–1.39]; OR [95% CI]=1.30 [0.92–1.85]), and prostate weight (OR [95% CI]=1.00 [0.99–1.02]; OR [95% CI]=1.01 [0.99–1.02]) were not significant predictors of urinary continence (0 ppd; 0 ppd or security pad, respectively).
ppd=pads per day; OR=odds ratio; CI=confidence interval; BMI=body mass index; AUASS=American Urological Association Symptom Score; R-BNP=robot-assisted bladder neck preservation.
Discussion
Our R-BNP technique involves dissecting the lateral edges of the BN from the overlying perivesical fat and base of the prostate before BN transection. This allows for a consistent BN transection that maximizes the ability to provide R-BNP, while minimizing the risk of BNR. A large BN may necessitate time-consuming reconstructive tapering, which may be more susceptible to anastomotic leak because of a longer suture line. In our study, 581 (97.0%) patients received some degree of R-BNP, while only 18 (3.0%) patients needed BNR. Although previous studies generally did not report the rate of BNR during attempted R-BNP, one report noted that BNR was needed in 0.9% to 96% of cases. 14 Furthermore, our approach to RARP and application of R-BNP remained consistent throughout the study interval, because the proportion of patients receiving the varying degrees of R-BNP, PSM rate, and postoperative urinary continence rate at 3 months and 1 year did not change with time.
When preoperative patient characteristics were analyzed to elicit factors that could potentially explain the need for differing degrees of R-BNP, mean age, BMI, preoperative AUASS, PSA level, clinical stage, and biopsy Gleason grade did not significantly influence the degree of R-BNP performed. When operative and postoperative patient characteristics were analyzed to elicit factors that could potentially explain the need for differing degrees of R-BNP, pathologic stage and postoperative Gleason grade did not significantly influence the degree of R-BNP performed. The presence of a median lobe and larger prostate weight, however, may inhibit the ability of the surgeon to perform a greater degree of R-BNP.
Although previous reports have supported the role of R-BNP in earlier return to postoperative continence, these reports only considered R-BNP on the basis of whether or not it was performed. 14 –16 The results of our study suggest that BNP is a graded, rather than an all-or-none outcome. An increasing degree of R-BNP performed was associated with a stepwise decrease in OR time, and a general decrease in EBL. These associations may be attributable to the additional manipulations associated with a large BN needed before anastomosis.
With regard to continence rates, similar outcomes were found regardless of whether continence was defined as 0 ppd, or 0 ppd or security pad. An increasing degree of R-BNP was associated with higher rates of continence at 3 months postoperatively. Patients who received grade 3 and grade 4 R-BNP had higher rates of continence at 3 months compared with patients who received grade 2 and grade 1 R-BNP. There was no difference in continence rates, however, between grade 3 vs grade 4, and grade 1 vs grade 2 R-BNP. Our results suggest that although there may not be a difference in continence rates at 3 months between BNR and a wide BNP, there may be improved continence rates when a tighter BNP is performed. These results could explain previous studies that showed no difference in return to continence between BNP and BNR. 17 When comparing continence rates at 1 year postoperatively, there was no difference among the four groups. Also, our finding that R-BNP was an independent predictor of urinary continence at 3 months but not at 1 year further supports the role of R-BNP in earlier return to urinary continence after RARP.
Some reports have suggested that BNP may increase the likelihood of PSM at the prostatic base. 18,19 Our results suggest that an increasing degree of R-BNP does not increase the likelihood of PSM. The total number of positive margins was 105/599 (17.5%); of these PSMs, 10/105 (9.5%) were at the base of the prostate. These values are comparable to those reported in the RARP literature. 20
Our study, one of the largest single surgeon series investigating R-BNP, is the first study to suggest that BNP may be a graded outcome. Our study must be taken in the context of being a retrospective study, however. Another limitation is the subjective nature of our grading scale. Nevertheless, we believe that characterizing degree of BNP may allow for a more accurate determination of the precise role of BNP in RP. Also, comparing our continence outcomes to those in the literature may be difficult because of the variations of the definition of postoperative continence. 21 This was our primary reason for conducting our analysis using two definitions of continence (0 ppd, and 0 ppd or security pad).
Conclusions
Our consistent BND technique allows for maximal R-BNP that does not compromise oncologic control, while minimizing the risk for BNR. R-BNP is a graded, rather than all-or-none outcome, and an increasing degree of R-BNP is associated with earlier return to continence, decreased mean OR time, and decreased EBL.
Footnotes
Acknowledgment
We would like to thank Brett Lissenden, biostatistical consultant at the Graduate School of Arts and Sciences, University of Virginia.
Disclosure Statement
Daniel D. Eun is a proctor for Intuitive Surgical and a lecturer for Covidien. David I. Lee receives study support from Johnson and Johnson and Pfizer and is a lecturer for Intuitive Surgical, Ethicon Endosurgery, and Covidien. For the remaining authors, no competing financial interests exist.