
Abstract
Objective:
To compare the treatment outcome of laparoscopic versus open surgery for renal masses with infrahepatic (levels I and II) tumor thrombus and analyze the largest series of retroperitoneal experience in such cases from China.
Materials and Methods:
Forty-nine patients with renal masses with infrahepatic tumor thrombus were analyzed retrospectively between January 2009 and January 2013 at our institution. The diagnosis was confirmed by computed tomography and/or magnetic resonance imaging preoperatively. They were divided into two groups based on the detailed surgical approach applied. Group 1 (A, pure laparoscopic; B, laparoscopic nephrectomy with open thrombectomy) consisted of 17 patients (34.7%) and group 2 (pure open) consisted of 32 patients (65.3%).
Results:
The two groups were comparable with regard to all of the patients' baseline characteristics. All operations were performed successfully without severe complications. In group 1, the mean operative time was 208.5 minutes, the mean estimated blood loss was 147.1 mL, the mean postoperative hospital stay was 5.8 days, and only two patients (11.8%) accepted blood transfusion with a mean quantity of 300 mL. In group 2, the figures were 268.3 minutes, 1345.3 mL, 12.5 days, respectively, and a total of 17 patients (53.1%) received transfusion with a mean quantity of 1488.2 mL. The differences of all these parameters were statistically significant between both groups (p<0.05). However, comparisons between the group 1A and 1B in all of the perioperative characteristics were not statistically significant. During a mean follow-up of 18.2 months, 13 patients in group 1 and 26 patients in group 2 survived. The difference in the cancer-survival rates between both groups was not statistically significant.
Conclusions:
Although it remains technically complex, demanding and challenging for renal masses with infrahepatic tumor thrombus, laparoscopic surgery with a retroperitoneal approach can make favorable perioperative results and comparable survival rates in selectively less complex patients compared with the traditional open surgery.
Introduction
S
Although LNT has not been recommended for all patients due to its technical challenge, it has recently been a more common modality owing to its minimally invasive feature compared to ONT. 3 McDougall et al. 4 reported the first successful transperitoneal LNT in 1996 and Savage et al. 5 depicted the first successful retroperitoneal LNT in 2000. Gradually, recent publications have fully confirmed the feasibility and safety of LNT 6,7 in cases of renal vein (RV) involvement. Unfortunately, although case reports have been introduced, there is still no series report of retroperitoneal LNT applied for renal masses with tumor thrombus, even if infrahepatic tumor thrombus. To our knowledge, we are the first to compare the treatment outcome of LNT versus ONT in renal masses with infrahepatic tumor thrombus and more importantly, to present the largest series of retroperitoneal experience in such cases from China.
Material and Methods
Between January 2009 and January 2013, a total of 49 patients diagnosed with renal masses with infrahepatic tumor thrombus received surgery at our institution. We retrospectively reviewed and analyzed the file records of these patients after obtaining approval from our institutional review board. In all patients, written informed consent was obtained. The patients with bilateral lesions and those with intrahepatic and suprahepatic tumor thrombus were excluded from the trail. None had experienced previous renal surgery or suffered from renal dysfunction. Among them, 34 (69.4%) were male and 15 (30.6%) were female. On admission, the extension level of the tumor thrombus and involvement of the wall of the vena cava were determined using computed tomography and/or magnetic resonance imaging preoperatively. A comprehensively operative plan, including cavotomy was subsequently confirmed if level II tumor thrombus existed. Typical radiographic indications of renal masses with infrahepatic tumor thrombus are revealed in Figure 1A–D. These patients were divided into two groups based on the detailed surgical approach applied. Group 1 (A, pure laparoscopic; B, laparoscopic nephrectomy with open thrombectomy) consisted of 17 patients (34.7%) referred to a single surgeon and group 2 (pure open) consisted of 32 patients (65.3%) operated by two other experienced surgeons. Patient demographics, intraoperative variables, and postoperative outcomes were reported and analyzed. By analyzing these perioperative data between both groups, all tests were carried out with the program SPSS v16.0. For statistical analysis, categorical variables were summarized as the frequency and percent. Continuous variables are summarized as the mean±standard deviation for normally distributed data. The groups were compared for continuous variables using the independent t test, Pearson Chi-square test, or Fisher's exact test. The significance level for each hypothesis was established at 0.05.
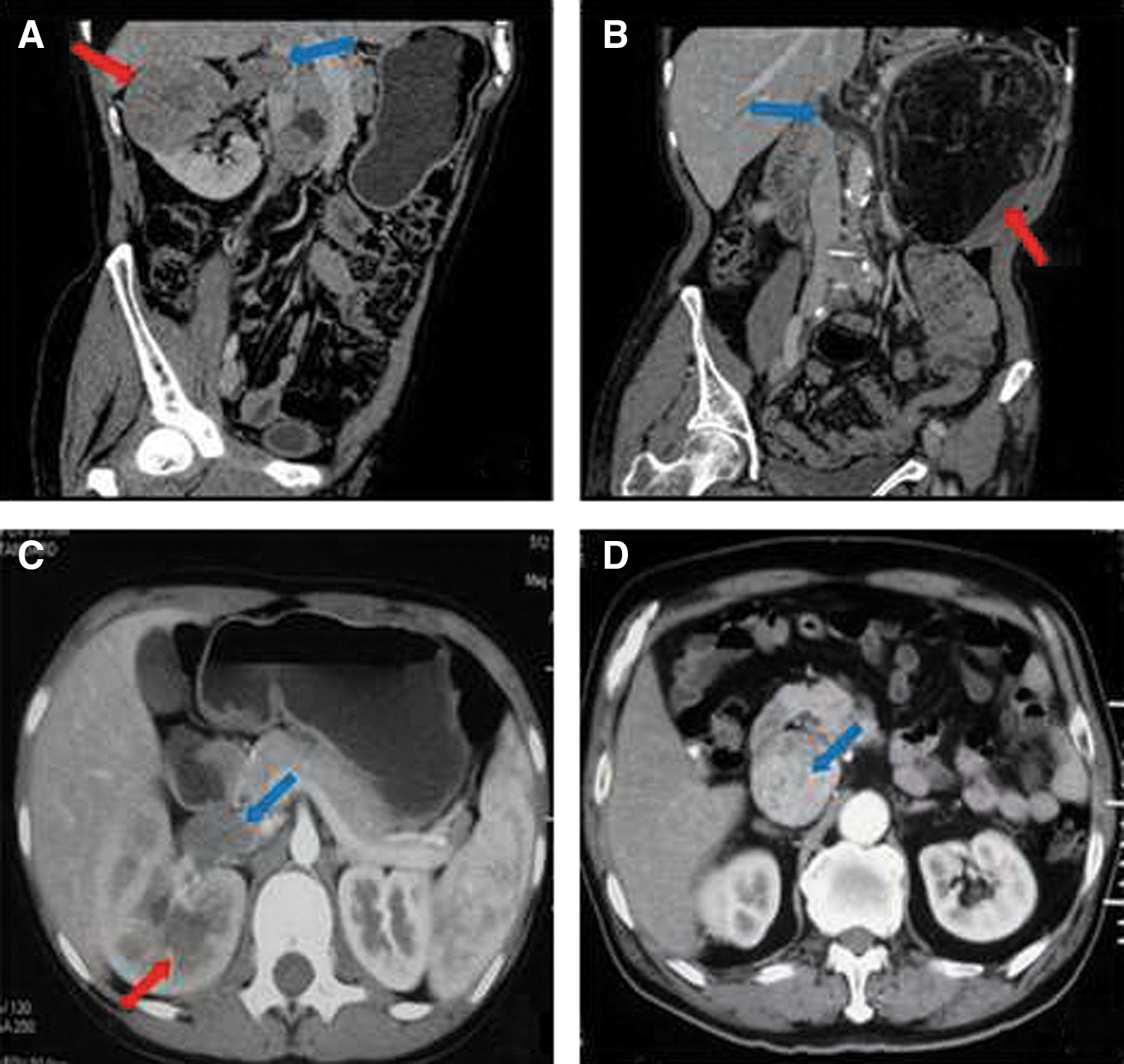
Typical images of renal masses
All of the 49 patients underwent a retroperitoneal approach with minimal handling of the abdominal cavity. None of these patients were embolized or receiving neoadjuvant targeted therapy preoperatively. After induction of general anesthesia, the patients were placed in the left or right lateral decubitus at 90 degrees. In group 1, the laparoscopic procedure was performed with only a three-trocar technique. The detailed procedures to construct a retroperitoneal cavity had been introduced previously in detail. 8,9 The three trocars formed an equilateral triangle (Fig. 2A, B) to provide a nearly empty cavity without any abdominal organs disturbing the manipulation. After longitudinal resection of Gerota's fascia and careful separation for the space between the kidney and perirenal fat, the renal artery (RA) was easily visualized, then carefully dissected up to its origin, and ligated with two-folded Hem-o-loks (Fig. 2C). Subsequently, the renal hilum was fully exposed and the tumor-bearing kidney was completely mobilized outside of Gerota's fascia with the ureter ligated, leaving the kidney attached only by the RV (Fig. 2D).
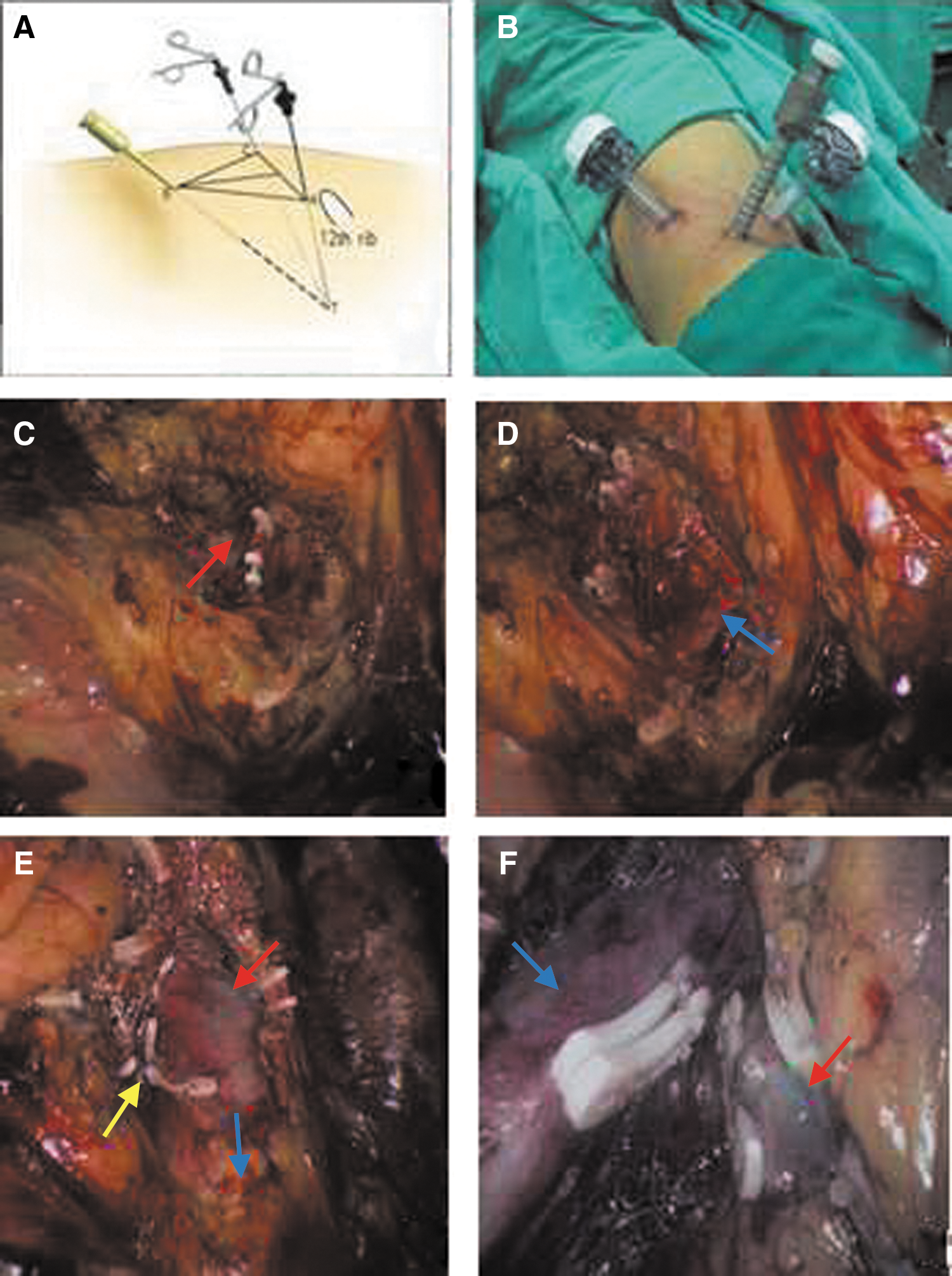
Intraoperative images under laparoscopic vision.
After the lumbar veins were ligated with the inferior vena cava (IVC) and venous tumor thrombus clearly identified (Fig. 2E), accurate intraoperative staging of the thrombus extension was essential for determining the appropriate surgical approach. If the tumor thrombus was classified into level I, meaning that tumor thrombus extending into IVC was short and could be milked back into the RV, pure retroperitoneal laparoscopic technique could be performed without occlusion of IVC and contralateral RV. After milking the thrombus distally into the RV, the RV was subsequently stapled between the milked thrombus and IVC to achieve proximal and distal vascular control (Fig. 2F). The kidney with tumor thrombus was then mobilized and entrapped in an impermeable EndoCatch bag (United States Surgical Corp.) without the kidney morcellated to facilitate extraction of large tumors. Finally, the enbloc specimen was removed intact through the port site without extension of skin incisions. However, if the tumor thrombus was classified into level II, especially the complex level II, including a higher location nearly at the intrahepatic level or a tumor thrombus with the largest diameter >7 cm of a renal mass, which could be confirmed with intraoperative ultrasonography, the thrombus would not be brought back distally to the RV. The patients were then laid flat to undergo a transperitoneally open thrombectomy after laparoscopic mobilization of the kidney, which facilitated safe cavotomy and thrombus extraction. An 5–10 cm subcostal incision was made for the most direct access to IVC. The IVC was mobilized and skeletonized circumferentially above and below the junction of the RV and IVC to the extent determined by the length of the tumor thrombus. A longitudinal incision was made in the IVC to remove the tumor thrombus intact with the IVC reconstructing by a running 4-0 polypropylene cardiovascular suture. The abdominal incision was finally closed in the usual fashion (Fig. 3A). Surprisingly, if the level I tumor thrombus could be milked purely and totally under the laparoscopic vision, the incisions would be more minimal and imperceptible (Fig. 3B). As for ONT in group 2, we had no special modification or innovation to the previously open retroperitoneal experience and the conventional standard surgical techniques were followed for mobilization, exposure, thrombectomy, and repair, if necessary.
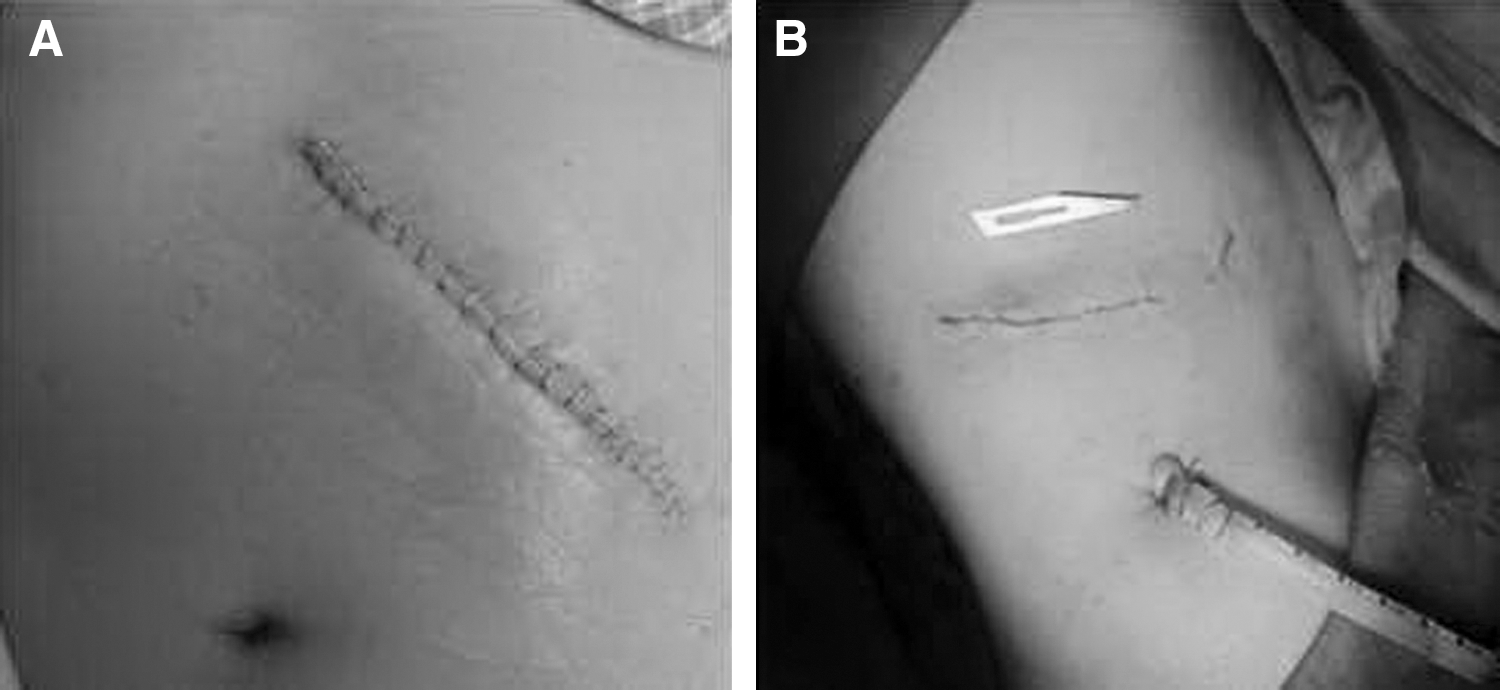
Postoperative incisions.
Patients were followed up at 3-month intervals postoperatively with physical examination, imaging studies, and serum creatinine evaluation. Survival was calculated from the data of surgery to the date of last follow-up visit for surviving patients or to death. Overall cancer-survival rates were estimated using Kaplan–Meier curves. The differences between groups were tested using the log-rank test.
Results
The detailed patient demographics and outcome characteristics are listed in Tables 1 and 2. The two groups were comparable with regard to all the patients' baseline characteristics, including age, body mass index, sex, tumor location, tumor size, and the detailed tumor thrombus level. All operations were performed successfully without severe complications such as acute pulmonary embolism and uncontrollable hemorrhage. All laparoscopic procedures were performed successfully without any unexpected intraoperative open conversions. There were also no intraoperative deaths. Apart from transfusion, only two patients in group 2 experienced postoperative minor complications (one poor wound healing and one intestinal obstruction), yet they were treated successfully only by conservative methods. The two groups were comparable in the complication rates, but a tendency of fewer complication events was observed in group 1. In group 1, the mean operative time was 208.5 minutes, the mean estimated blood loss was 147.1 mL, the mean postoperative hospital stay was 5.8 days, and only two patients (11.8%) accepted blood transfusion with a mean quantity of 300 mL. In group 2, the figures were 268.3 minutes, 1345.3 mL, 12.5 days, respectively, and a total of 17 patients (53.1%) received transfusion with a mean quantity of 1488.2 mL. The differences of all these intra- and postoperative parameters, including operative time, estimated blood loss, hospital stay, blood transfusion, and quantity of transfusion were statistically significant between both groups. Above all, group 1 was associated with shorter operative time, less blood loss and blood transfusion, faster recovery, and fewer complications.
BMI=body mass index.
Furthermore, when making a comparison among these parameters between group 1A and 1B, there was no significant difference involved in all of the perioperative characteristics although a more relatively complex level II tumor thrombus was included in group 1B.
Histology revealed 46 renal cell carcinomas (RCC), 2 renal angiomyolipomas and 1 nephroblastoma in all patients with negative surgical margins. During a mean follow-up of 18.2 months (range 4–33 months), 13 patients (76.5%) in group 1 and 26 (81.3%) in group 2 survived without any recurrence or metastasis. The survival curves are illustrated in Figure 4. The difference between both groups was calculated by the log-rank test, which was proven not statistically significant (p=0.768>0.05).
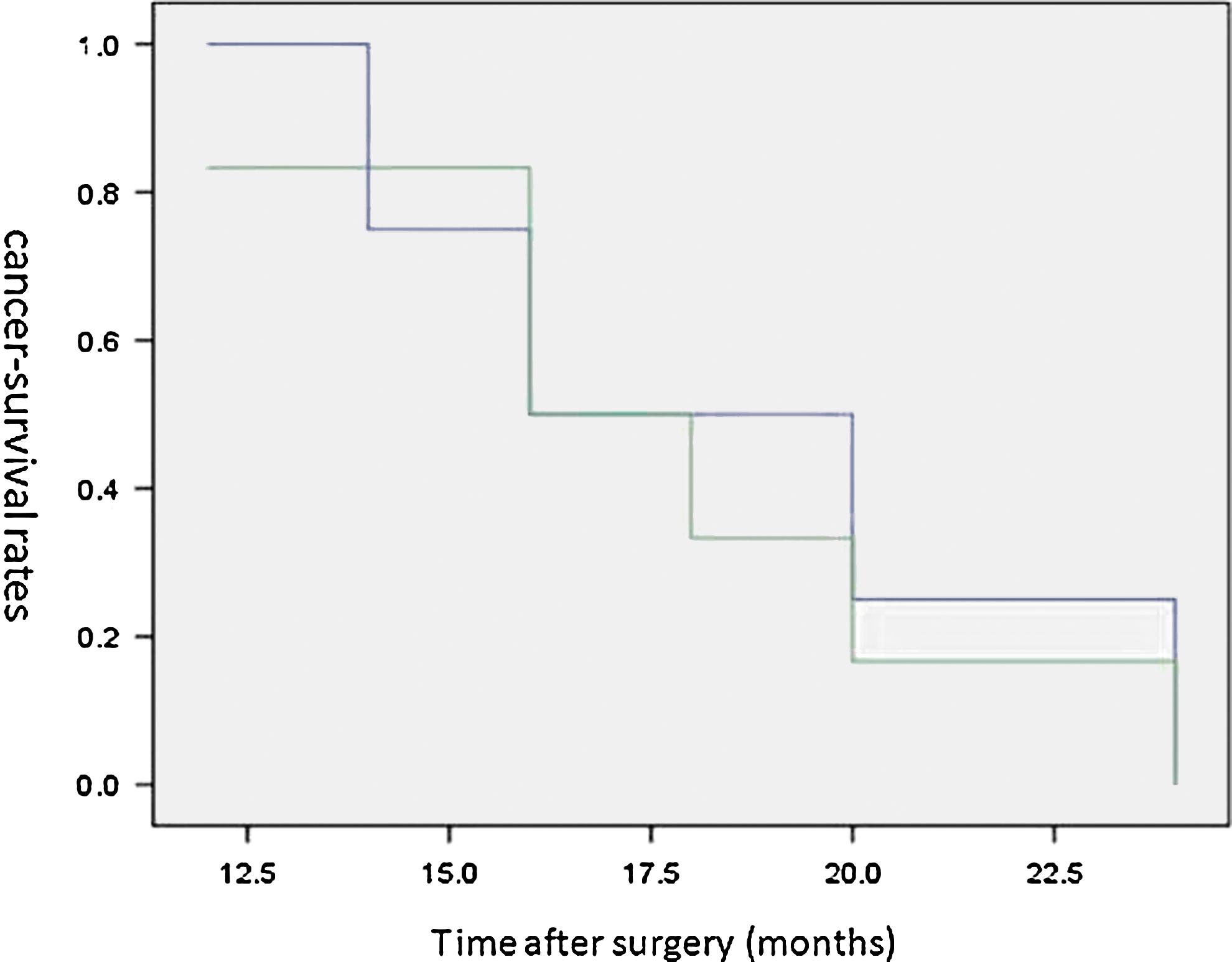
Cancer-specific survival rates of patients in group 1 (blue curve indicated) and group 2 (green curve indicated).
Discussion
Renal masses with venous tumor thrombus are not rare, particularly in RCC with tumor thrombus, which has a tendency to invade IVC with an incidence ranging from 4% to 15%. 10,11 The recommended and well-established option for the treatment of this disease is ONT, 12 enabling long-term survival in >50% of patients with infrahepatic tumor thrombus without distant metastasis. 13 Nevertheless, accumulating evidence has supported a laparoscopic approach to be applied in the treatment, although few published data are available. Our present study is a direct comparison of retroperitoneal LNT and ONT for patients suffering from renal masses with infrahepatic tumor thrombus. The intraoperative safety and short-term survivals were evaluated to figure out the feasibility and advantages of retroperitoneal LNT.
It is believed that LNT is a challenging procedure not only because of the complicated expertise, but primarily two increased risks of undesirable events: thrombus fragmentation with possible pulmonary embolism and uncontrollable hemorrhages. 14 Nevertheless, serious and fatal complications can also occur with ONT. To solve the problem, Gorin et al. 15 advised that addressing the tumor thrombus before kidney mobilization can minimize the torque transmitted to the thrombus and decrease the risk of tumor embolization although we never attempted this technique for the difficult manipulation in a retroperitoneal vision. Due to the above risks, we emphasize that it is not always necessary to perform a purely laparoscopic approach for minimal invasion. Especially in our clinical research, some patients underwent retroperitoneal laparoscopic nephrectomy with open thrombectomy, not pure retroperitoneal laparoscopic technique, for warding off the risk of gas embolisms, massive hemorrhage, and the neoplastic dissemination, given the considerable size of these tumors and the need for a huge incision for complete specimen extraction. This crossover technique combined with a minimal laparoscopic invasion and safe open manipulation has also been carried out and developed gradually by many urologists. 3,16,17
According to our initial experience, LNT has its exclusive intraoperative and postoperative advantages compared to ONT. In laparoscopic visualization, especially the retroperitoneal approach offering an excellent exposure of the surgical field, RA can be visualized and spared directly, then ligated easily without any perturbation to the RV containing tumor thrombus. Once the RA is ligated, the intrahepatic IVC tumor thrombus often retracts spontaneously a few centimeters, which facilitates to milk the tumor thrombus into the proximal RV completely using pure advanced laparoscopic techniques. In addition, LNT can result in shorter operative time, less bleeding and blood transfusion, faster recovery, and even a relatively shorter incision compared with ONT, all of which have been confirmed in our analysis. Our investigation also demonstrates that there are no significant differences between LNT and ONT in terms of perioperative complications and postoperative mortality, which may strongly support the perioperative safety of LNT although the conclusion of whether LNT is indeed more or less safe than the ONT has not been made.
In Table 3, combining our laparoscopic data with the other urologists' experience, the perioperative data are relatively superior owing to the direct visualization and a bloodless field with the advantages of retroperitoneal approach. In retroperitoneal LNT, it can afford easier access to the RV and a quicker access to the IVC than the transperitoneal route without necessity to mobilize the liver, duodenum, or colon. Another advantage of the retroperitoneal route is a shorter total operative time resulting from optimal and immediate access to the RA and RV compared with the transperitoneal approach. Moreover, the transperitoneal approach fails to provide a satisfied vision to expose the lumbar veins, which will increase the rates of massive hemorrhage or conversion to open surgery due to venous laceration, but the lumbar veins can be dissected easily and ligated completely in the retroperitoneal approach. Besides, although transperitoneal LNT is recommended in European and American daily practice for a greater working space and a more distinguishable anatomical structure, it may not be applicable to Asian patients who often have a smaller body contour compared to those from Europe and America, which means that there is a relatively smaller manipulation space for the eastern people by the transperitoneal pathway.
EBL=estimated blood loss; LNT=laparoscopic nephrectomy with thrombectomy; NA=not available.
Admittedly, our study has several limitations. First of all, it is a retrospective and nonrandomized study. The retrospective nature of this series clearly biases subsequent analysis. Second, no evident criteria exist to determine how to choose surgical modalities and it just depends on the surgeon's preference and patient's selection. Besides, although the short-term results are encouraging in laparoscopic technique, the incidence of local recurrence and distant metastasis in the long-term follow-up is still not clear. Despite the limitations of this study, the usefulness of comparing the treatment outcome of LNT versus ONT for renal masses with infrahepatic tumor thrombus is to build a foundation in the literature to support future prospective clinical experiments.
Conclusion
In conclusion, although it remains technically complex, demanding and challenging for renal masses with infrahepatic tumor thrombus, the pure laparoscopic or laparoscopic-assisted surgery in retroperitoneal approach can make favorable perioperative results and comparable survival rates compared with the traditional open approach. Hence, they cannot be recommended as a first line of surgical approach for most patients temporarily and should be considered only in highly selected cases with experienced hands.
Footnotes
Disclosure Statement
No competing financial interests exist.