
Abstract
Purpose:
To evaluate the feasibility of performing noninvasive puncture of pediatric ureteroceles with cavitation-based focused ultrasound (US) (histotripsy).
Materials and Methods:
A model for the ureterocele wall was developed from an excised bovine bladder wall. The model was exposed to focused US pulses in a water bath under three different US parameter sets for up to 300 seconds to create localized perforations in the wall. B-mode US imaging was used to monitor the treatment and assess potential imaging guidance and feedback.
Results:
Punctures were formed between 46–300 seconds, depending on the focused US exposure parameters and model wall thickness. Puncture diameter was controllable through choice of exposure parameters and could be varied between 0.8–2.8 mm mean diameter. US-induced cavitation was visible on B-mode imaging, which provided targeting and treatment feedback.
Conclusions:
Cavitation-based focused US can create punctures in a model that mimics the tissue properties of a ureterocele wall, under guidance from US imaging.
Introduction
A
Treatment varies with ureterocele form and severity of symptoms. Endoscopic puncture is the most common method, whereby an electrode or laser is used to create one or more small incisions and relieve obstruction of urinary flow. 5,6 While this technique is less invasive than open repair, instrumentation may seed bacteria into the urine and lead to a UTI. Furthermore, there are concerns regarding the use of general anesthesia in children, especially neonates. 7
A noninvasive approach to ureterocele puncture may remove such risks from the procedure. Histotripsy is a form of noninvasive therapy that uses focused ultrasound (US) to create controlled mechanical erosion of soft tissues by US-generated cavitation or boiling bubbles. 8 –10 With this technology, the US energy is focused and delivered transcutaneously to the target to cause localized tissue breakdown into subcellular fragments. 11 This method has been successfully applied in animal models for treatment of benign prostate hyperplasia, 12 deep vein thrombosis, 13 and tumors. 14
In the present study, we evaluated the feasibility of using histotripsy to generate a mechanical puncture under US image guidance with a tissue model for the ureterocele wall.
Materials and Methods
A model of the ureterocele wall was developed using freshly excised bovine bladder tissue. The bladder was harvested and maintained in degassed phosphate-buffered saline until use (<12 hours from excision). The bladder was sectioned into 5×5 cm segments. The mucosal and submucosal layers were denuded from the underlying muscle and adventitia to create a membrane 0.5–1 mm in thickness. The mucosal membrane was placed over a circular opening of a polypropylene chamber containing dyed saline. The membrane was fixed with a band around the container such that the membrane sealed the fluid in the chamber without applying tension to the membrane, aside from that caused by the sample's own weight. This model provided an end point for determination of puncture when dyed saline could be observed flowing through the puncture hole in the membrane.
A custom US therapy system constructed in our laboratory was used to deliver focused US energy to the samples. The therapy transducer was a 1 MHz seven-element array with 14.7-cm diameter. Each element of the transducer was focused through a plastic lens, with all lenses focused at the radius of curvature of 14 cm. The transducer was electrically driven by a radiofrequency class D amplifier similar to that used by Hall and Cain, 15 but modified to output high-amplitude pulse durations up to 10 ms. The amplifier output was controlled by an electronic timing board that specified the US pulse duration (PD), pulse repetition rate (PRF), and transducer operating frequency.
The three-dimensional pressure output of the transducer was obtained under free field conditions in a degassed water bath by acoustic holography with a capsule hydrophone (HGL-0085, Onda Corporation, Sunnyvale, CA) recorded at low pressure amplitudes and nonlinear acoustic simulation. 16,17 The focal pressures were confirmed by measurements with a fiberoptic probe hydrophone (FOPH2000, RP Acoustics, Stuttgart, Germany). The linear -6dB focal pressure beam width was 2.0 mm transverse to the acoustic axis by 13.6 mm along the acoustic axis. The focal peak positive pressure of the US pulses applied in this experiment was 100–120 MPa, and the peak negative pressure applied was 17–20 MPa. Pulses between 1–5000 cycles duration were used in the experiments, with the pulse rate selected in each case to fix the duty cycle at 0.5% to 0.6%. Correspondingly, the time-averaged spatial peak intensity of the exposure was between 145–190W/cm2.
A research US imaging engine (V-1, Verasonics Inc., Redmond, WA) with a linear array probe (L7-4, Philips Healthcare, Andover, MA) operated at 5 MHz was used to visualize the treatment area before, during, and after exposure in a subset of the experiments. The imaging was triggered by the therapy system such that the images were synchronized to avoid acoustic and electrical interference from the therapy US pulses. Because of the low duty factor of the therapy output (≤1%), the frame rate of the US imager could be maintained at ≥10 frames per second during treatment.
The sample, along with the therapy and imaging transducers, was positioned in a degassed, filtered water bath (Fig. 1). An alignment laser was used to identify the position of the focus in the water. Next, the membrane was translated by a three-axis motorized positioner (Velmex Inc., Bloomfield, NY) to align the tissue with the therapy transducer focus. A short, 1-second exposure was then used to confirm alignment by visualization of cavitation on the membrane. The imaging probe was aligned off-axis in the water bath in the plane of the therapy focus to observe the treatment region. A digital camera (S8000, Nikon USA, Melville, NY) was used to record a video of each exposure.

Experimental alignment of the sample with the therapy and imaging transducers during exposure. The sample was sealed over a chamber of dyed saline and attached to a three-axis motor positioner to align it with the therapy transducer focus. An imaging probe was positioned at an oblique angle in the focal plane to observe the cavitation activity pre- and postpuncture.
The membrane was exposed under a set of US therapy pulse parameters until a visual puncture through the membrane was observed. In some cases, punctures were falsely identified, and no dye was visualized flowing through the membrane when the therapy was turned off. In these cases, the membrane was further treated until a positive result was achieved for up to 300 seconds total treatment time. After treatments, the punctures were photographed and measured while still attached to the container outside of the water bath.
Results
A localized cloud of cavitation bubbles was observed during US exposure at the focus of the therapy transducer on the sample wall. Puncture was achieved in the samples using three different acoustic parameter sets. Blue dye was visible leaking through the membrane once the treatment was terminated, indicating a communication was formed.
Puncture diameter was consistent for a given set of exposure parameters, even with different sample thicknesses (n=8–16 punctures) (Figs. 2, 3). Puncture diameter was smallest (0.8±0.1 mm, mean±standard deviation) with a short PD of 2 μs delivered at PRF=3000 Hz. Punctures were significantly larger (1.2±0.2 mm, P<0.001) with PD=5 μs delivered at PRF=1000 Hz. The exposure time necessary to achieve a puncture varied with the thickness of the membrane, but was not significantly different between these two parameter sets (151±63 seconds, PD=2 μs vs 131±64 s, PD=5 μs).
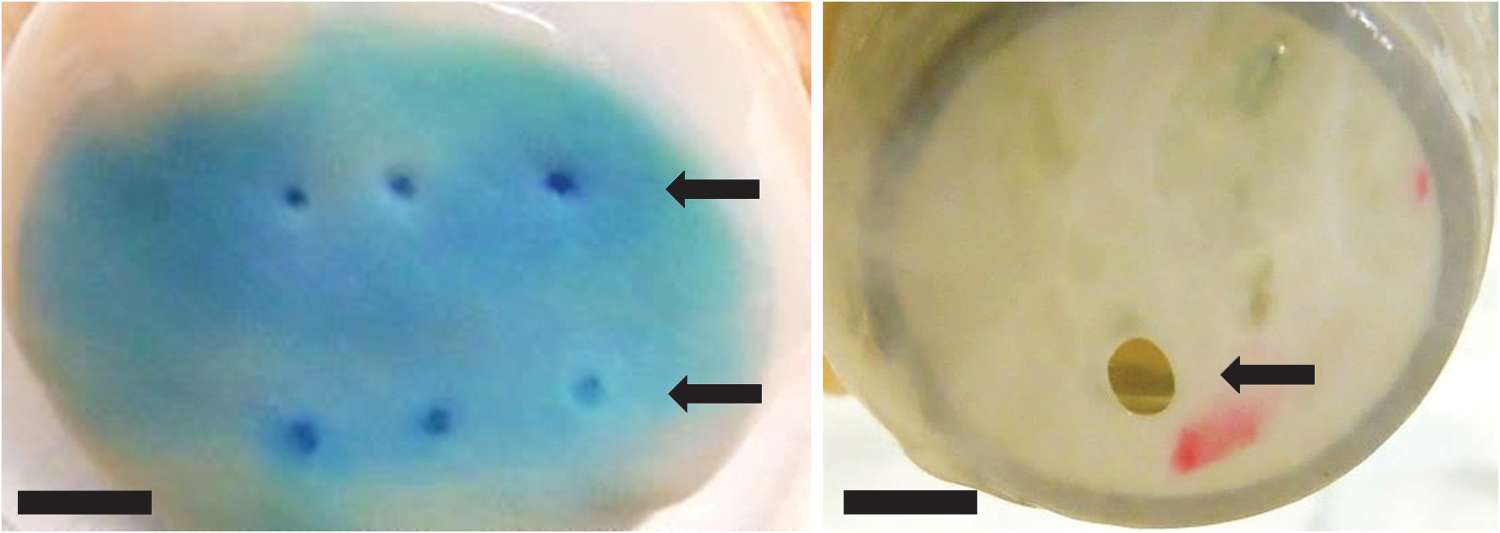
Left, six punctures made in the bladder wall membrane by exposures with a short pulse duration (2 μs). Right, a larger puncture generated by a sequential exposure of 1 μs pulses followed by 5000 μs pulses. The scale bars are both 5 mm.

Mean puncture diameter vs duration of pulses in the exposure. Error bars indicate the range of puncture sizes observed. PD=pulse duration; PRF=pulse repetition frequency.
Exposures using a much longer PD applied at a low PRF did not form a complete puncture within the 300 second time window. Once a small puncture was formed, however, such pulses effectively expanded the perforation diameter. This outcome was demonstrated by first using a short PD (1 μs) at high PRF (5000 Hz), then delivering to the same location pulses with PD=5000 μs at PRF=1 Hz, which expanded the puncture to a final dimension of 2.8±0.4 mm.
US B-mode images indicated the presence of cavitation as an echogenic region at the focal point (Fig. 4). Before puncture, cavitation was limited to the proximal membrane surface (transducer side). Cavitation was visualized, however, penetrating into and eventually through the membrane, forming a narrow jet in the fluid space distal to the surface. The puncture was not visible after treatment as a hypoechoic region in the membrane, as is apparent on bulk tissues treated by histotripsy. 18

Visualization of bladder mucosa puncture by B-mode ultrasound (US) image guidance before treatment
Discussion
Current methods of ureterocele treatment include minimally invasive endoscopic puncture and open surgery. This study identified a potential noninvasive method using focused US to create a puncture in ureteroceles under US image guidance. Ideally, the treatment would be delivered without general anesthesia as an office-based procedure using a hand-held transducer the size of a diagnostic US imager. The current experimental exposure time of ∼2 to 3 minutes, however, may be longer than desirable to avoid anesthesia. The time to puncture varied significantly between samples, possibly because of variation in properties of the sample that were not carefully controlled in this study, such as membrane thickness, tension, and curvature. Puncture may be achievable over a shorter time using acoustic parameters outside of the range tested in our study. The level of pain experienced during such a procedure is not known and will have to be evaluated carefully to determine an appropriate level of sedation.
The treatment times found in our study indicate that the bladder wall needs a significantly greater acoustic dose to disintegrate than that needed to ablate soft, parenchymal tissues with histotripsy. 8,12 Hall and associates 19 similarly found that the more energy was needed to ablate the urethra compared with the surrounding prostatic tissue in a canine model of benign prostate hyperplasia. It is not clear, however, how well the model used in our study mimics the true mechanical properties of the ureterocele wall. Despite the tissue resilience, perforations were reliably achieved with a controllable size and location. The flexibility to alter puncture size may allow the clinician to optimize the technology for individual treatments.
There are currently several techniques used for decompression without an accepted standard. 20,21 Decompression has been achieved with a single puncture as small as 3F, 22 or a transverse incision of 2 to 3 mm. 23 A retrospective analysis found no indication of correlation between puncture technique with outcomes. 21 Recent studies, however, suggest alternate puncture patterns could reduce the risk of vesicoureteral reflux over a simple single incision. 24,25 Future refinement of both the model and the therapy system will aid in better assessing the clinical parameters.
Our results also suggest that US imaging can provide feedback to the operator for precise position of treatment and detection of the puncture. It was possible to detect a perforation when therapy was being delivered with cavitation observed on both sides of the ureterocele. The tendency for formation of a cavitation cloud at the fluid-tissue interface has been noted by Xu and colleagues 26 and possibly arises from bubbles being preferentially pushed into the membrane by acoustic radiation force. On puncture, this force would cause bubbles to flow through the hole, as observed on B-mode images. The hole was not visible directly under B-mode ultrasonography post-treatment, however. Color Doppler US may complement B-mode imaging feedback in providing information on the flow channel created after therapy and help determine a more precise end point.
In addition to neonatal surgery, another appealing possibility would be the management of ureteroceles in utero. Recently, Aoki and coworkers 27 applied high-intensity focused US with a 60-second exposure to create a 1-mm diameter vesicoamniotic shunt in a neonatal rabbit as a model treatment for fetal lower urinary obstruction. The authors noted a small region of thermal necrosis outside the focus but otherwise no collateral injury. In addition, Kim and associates 28 demonstrated targeted delivery of histotripsy therapy to internal organs in a fetal sheep model. These studies suggest that, in addition to perforation of ureteroceles in neonatal patients, noninvasive fetal surgery may be possible if a diagnosis is made during prenatal ultrasonography.
Conclusions
Pulsed focused US can create a mechanical perforation in denuded bladder mucosa, a tissue model for the ureterocele wall. The puncture diameter was repeatable and could be controlled by US exposure parameters. US imaging allowed for real-time targeting and visualization to confirm puncture. These results indicate that histotripsy as a noninvasive method of ureterocele puncture is feasible.
Footnotes
Acknowledgments
The authors wish to thank Rusty Starr, Julianna Simon, Tanya Khokhlova, and Yak-Nam Wang from the Applied Physics Laboratory at University of Washington for their help in obtaining samples. This study was supported by grants from the National Institutes of Health 2T32 DK007779-11A1 and 2R01 EB007643.
Disclosure Statement
No competing financial interests exist.