
Abstract
Purpose:
Shockwave lithotripsy (SWL) induces acute kidney injury (AKI) that extends from the papilla to the outer cortex by causing ischemia and the production of nephrotoxic agents. Direct ischemic damage and the generation of free radicals cause injury to the proximal tubular cells. Kidney injury molecule-1 (KIM-1) is a transmembrane glycoprotein that is upregulated in proximal tubular cells after ischemic or nephrotoxic injury and is not expressed in healthy kidneys. We evaluated the extent of free radical production in response to SWL by measuring urinary total antioxidant capacity (TAC) and total oxidant status (TOS). Furthermore, we investigated the severity of SWL-induced kidney injury by measuring KIM-1 expression levels.
Patients and Methods:
The study population comprised 30 patients who were carefully selected and 30 age and sex matched control subjects. All patients received the same SWL procedure. Midstream urine samples were collected from patients before SWL and at 120 minutes after SWL. Urine KIM-1 levels were measured by enzyme-linked immunosorbent assay, and TAC and TOS were measured via spectrophotometry.
Results:
Mean levels of TAC (2.88±0.56 mmolTxEq/L),TOS (8.27±1.57 μmolH2O2Eq/L), and KIM-1 (0.55±0.08 ng/mL) before SWL were not significantly different from mean TAC, TOS, and KIM-1 levels measured from the control group at 2.81±0.42 mmolTxEq/L, 10.73±1.4 μmolH2O2Eq/L, and 0.51±0.07 ng/mL, respectively. Two hours after SWL, mean urine TAC levels (2.81±0.85 mmolTxEq/L, P=0.02) were decreased and mean KIM-1 expression (0.85±0.11 ng/mL, P=0.01) was significantly increased, but there was no significant difference in mean TOS levels (11.24±1.9 μmolH2O2Eq/L, P=0.627) compared with the control group.
Conclusions:
The increased burden of free radical oxidants in the setting of decreasing antioxidant capacity may be one of the initial indicators of AKI after SWL. Moreover, KIM-1 demonstrates great potential as an early and noninvasive biomarker of SWL-induced kidney injury.
Introduction
K
The extent of damage to the kidney by SWL is evaluated by several parameters. Previous studies revealed that there were no significant discrepancies in renal function tests including glomerular filtration rate, serum creatinine, and electrolyte levels between subjects who did and did not receive SWL. 6 –8 Nevertheless, many studies continue to investigate how to best quantify the effect of acute insults to the kidney by evaluating various noninvasive biomarkers of renal injury. 9,10 The current literature suggests that the most effective biomarkers of renal damage are kidney injury molecule-1 (KIM-1), neutrophil gelatinase-associated lipocalin (NGAL), liver-type fatty acid binding protein, and interleukin-18 (IL-18). 10 KIM-1 is a transmembrane protein that is upregulated in proximal tubule cells after ischemic or nephrotoxic AKI. 10 Ichimura and associates 11 reported that KIM-1 expression increases in rat kidneys that are subjected to ischemic insults. Furthermore, KIM-1 can be detected in the urine immediately after AKI. 12 Various studies proposed that KIM-1 is a promising biomarker for diagnosing AKI and monitoring clinical improvement. 10,13 –15
It was first hypothesized that SWL damages kidney tissues because of direct trauma inflicted by the shockwaves. 1,5,16 –18 In recent studies, however, it has been reported that the adverse effects of SWL are imparted by free radical formation, which is similar to the damage caused by ischemia/reperfusion (I/R) injury. 16,19,20 To determine the degree of I/R injury, levels of malondialdehyde (MDA), superoxide dismutase (SOD), total antioxidant capacity (TAC), and total oxidant status (TOS) are measured. Although KIM-1 expression has been evaluated in many contexts that may result in AKI, it has not been studied in patients who received SWL treatment for kidney stones. In addition, levels of TAC and TOS after performing SWL have been rarely reported in the literature. In this study, we aimed to evaluate the harmful effects of SWL on kidney tissue by measuring KIM-1 expression and levels of TAC and TOS.
Patients and Methods
This randomized, prospective controlled study was performed between January and April 2012. Study subjects included 30 patients who all received unilateral SWL to manage kidney stones and 30 healthy age and sex matched volunteers who served as controls. All patients passed screening for normal renal function and blood pressure. Subjects who had previous renal surgery, a solitary kidney, congenital renal anomalies, illicit drug or medication use, and evidence of other urinary tract disorders such as pyelonephritis or ureteral calculi were excluded from the study. Demographics including age and sex were recorded for all participants. For patients receiving SWL, kidney stone size; lithotripter settings such as energy, shockwave frequency, and shockwave number; postprocedure complications; and hemodynamic parameters consisting of pulse rate, blood pressure, and respiration rate were documented. This study was approved by the Institutional Review Board of Dicle University Medical Faculty, and informed consent was obtained from all subjects preceding their participation in the study. All patients treated with SWL gave their informed consent before the procedure.
Urine samples were collected from patients immediately before SWL and 120 minutes after the procedure. Midstream urine specimens were stored at 20°C until further testing was performed. The Lithostar Modularis Uro-Plus (Siemens Medical Systems, Germany) SWL system was used to obliterate kidney stones for all patients. This model is a third generation electromagnetic lithotripter with an endoscopic treatment table that, according to the manufacturer, has improved shockwave delivery.
Urine samples were all centrifuged, and the supernatant was extracted to determine TAC. Measuring TAC was achieved with a novel automated and colorimetric method developed by Erel. 21 TAC results were expressed as nmol Trolox equivalent/mg protein. The TOS was also determined from supernatant fractions with the colorimetric method developed by Erel. 22 The assay was calibrated with hydrogen peroxide, and the results were expressed in terms of nmol H2O2 equivalent/mg protein. KIM-1 levels were determined by enzyme-linked immunosorbent assay (Aviscera Bioscience Inc. Santa Clara, CA).
The distribution of all parameters was tested using the one-sample Kolmogorov-Smirnov test. The Mann-Whitney U test was applied to compare nonparametric values and the t tests were used to compare parametric values. This was followed by testing statistical significance of repeated measurements with a Wilcoxon signed-ranks test to compare mean TAS, TOS, and KIM-1 levels. All data were expressed as mean and standard deviation. Statistical significance was defined as P-values <0.05. All data were obtained using the SPSS18.0 (SPSS, Inc. Chicago, IL).
Results
Of the patients who comprised the patient group (n=30), 21 were males and 9 were females. In the control group (n=30), there were 20 males and 10 females (P=0.452). The mean age of patients was 49 years while it was 47 years for control subjects (P=0.657). Patients presented with a unilateral kidney stone located either in the left (n=17) or right (n=13) kidney, and the mean stone size was 11.2 mm. The mean SWL procedure duration was 28.7 minutes, and each patient received 2500 shockwaves. The mean energy applied during treatment was 19.6 kV. No serious complications such as hematuria, hematoma, urinary tract infection, or urinary obstruction occurred during or after all SWL procedures. For all patients, this was the first SWL procedure that they had received for kidney stone treatment (Table 1).
SWL=shockwave lithotripsy.
Mean levels of TAC (2.88±0.56 mmolTx Eq/L), TOS (8.27±1.57 μmol H2O2 Eq./L), and KIM-1 (0.55±0.08 ng/mL) before the SWL procedure were not significantly different from mean TAC, TOS, and KIM-1 levels measured from the control group at 2.81±0.42 mmolTx Eq/L, 10.73±1.4 μmol H2O2Eq/L and 0.51±0.07 ng/mL, respectively. Two hours after SWL, mean urine TAC levels (2.81±0.85 mmolTx Eq/L, P=0.02) were decreased, and mean KIM-1 expression (0.85±0.11 ng/mL, P=0.01) was significantly increased (Fig. 1), but there was no significant difference in mean TOS levels (11.24±1.9 μmol H2O2Eq/L, P=0.627) compared with the control group (Table 2).
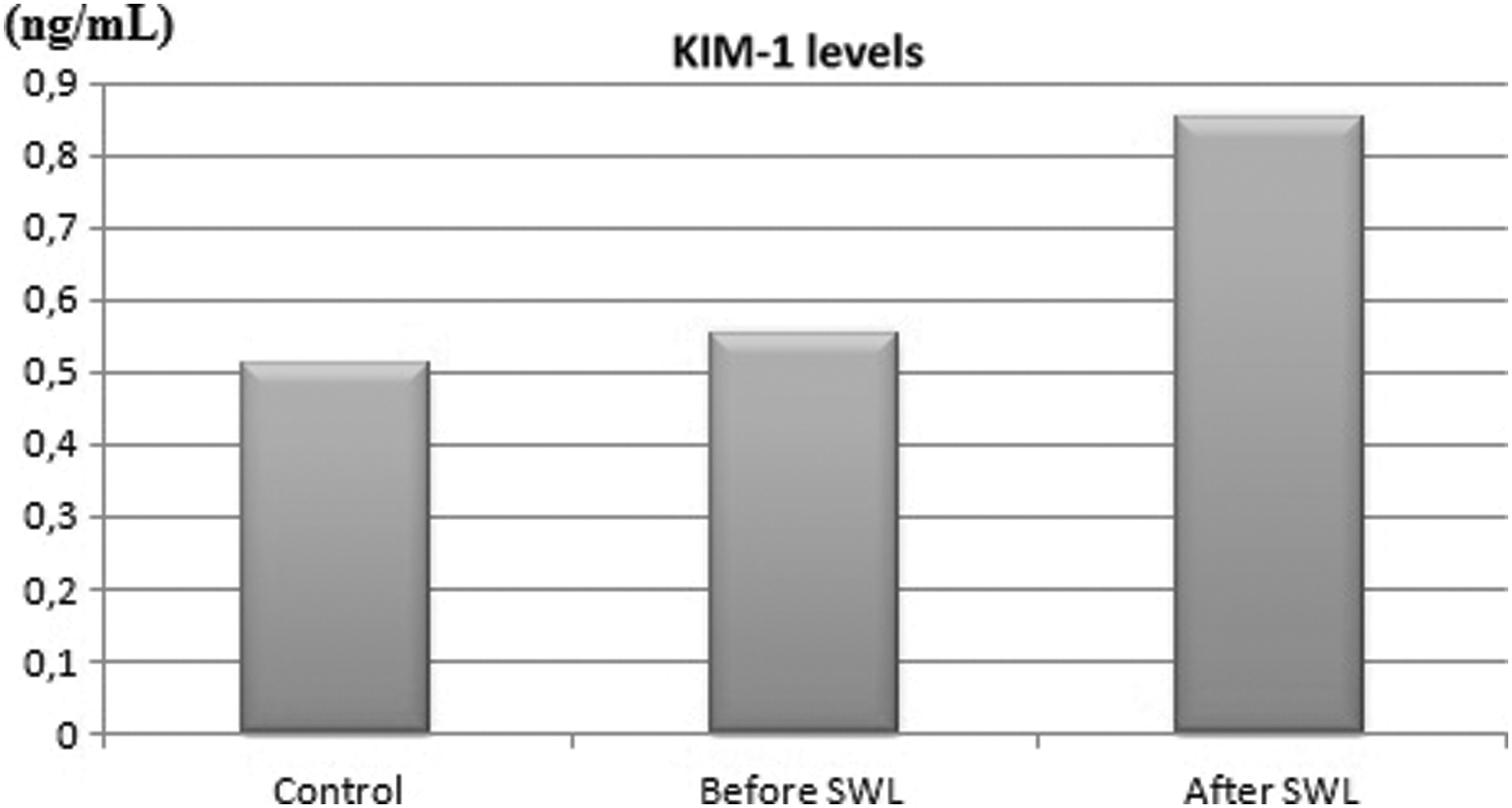
Graphic shows mean kidney injury molecule (KIM) −1 levels in control and patient groups both before and after shockwave lithotripsy (SWL) treatment.
SWL=shockwave lithotripsy; KIM-1=kidney injury molecule-1; TAC=total antioxidant capacity; TOS=total oxidant status.
Discussion
SWL is widely used for the management of stones that are located in the upper urinary tract. Although this procedure is highly effective and safe, it is not completely free from side effects. During SWL, a disruption occurs in the renal capillary system that results in damage from I/R. 23 In a study performed with a porcine model, free radical levels were elevated after SWL compared with the untreated contralateral kidney. 24 Moreover, in another study, it was reported that SWL produces oxidants with an assay that indirectly measured free radical generation by quantifying the amount of fluorescence that remained suspended in cells after the procedure. 25
Kidneys are highly perfused organs; 1 L to 1.5 L of blood passes through these organs every minute. Thus, it was postulated that SWL also affects the blood cells traveling through the kidneys during treatment. Aksoy and associates 23 reported that erythrocyte glucose-6-phosphate dehydrogenase, SOD, and catalase functions were significantly decreased 1 hour after SWL compared with values measured before the procedure. 23 Similarly, Golovanov and colleagues 26 reported that erythrocyte membrane SOD activity decreased and MDA concentrations increased in the erythrocytes of patients with renal urolithiasis who were treated with SWL.
As discussed above, SWL may contribute to kidney injury via a mechanism similar to I/R. It is well understood that free radicals play a central mechanistic role in I/R injury. If an organ is perfused after a period of ischemia, then molecular oxygen acts as an electron acceptor, which causes the generation of two superoxide anions such as hydrogen peroxide and hydroxyl radicals. 27,28 Erel reported that serum concentrations of different oxidant species and antioxidants can be measured separately, but these assays are time-consuming, labor-intensive, costly, and need much technical expertise. 21,22,29
Because measuring different oxidant molecules and antioxidants separately is not practical, methods to measure TOS and TAC were developed. As such, we used these methods to measure TAC and TOS to determine whether SWL induces kidney injury. In a similar study, it was reported that TOS levels were significantly increased, whereas levels of TAC did not change before and after SWL treatment. 16 We found that levels of TAC increased while levels of TOS remained unchanged. These discrepancies between our results and those of that study may be because of differences in urine collection. The previous study collected urine over 24 hours, and we collected spot urine samples 2 hours after the SWL procedure. These data suggest that free radicals are generated early on after SWL and that antioxidants are generated rapidly in response to the higher burden of oxidants.
Urinary KIM-1 is a well-studied biomarker that is expressed in the apical membrane of proximal tubular cells (PTC) and is expressed and released in the setting of kidney injury. 30 When PTCs are damaged, they begin to express molecules that may be used to diagnose and monitor tubular epithelial injury. 31,32 Some of these molecules include KIM-1, NGAL, osteopontin, IL-18, and clusterin. 10,31,33,34 Comparing all of these biomarkers, KIM-1 appears to be most useful indicator of kidney injury. 12,31 In 2008, Zhou and coworkers 35 performed an experimental study with rats that were acutely exposed to gentamicin, mercury, and chromium. Then the authors compared KIM-1 with other biomarkers and reported that urinary KIM-1 had the highest sensitivity and specificity in detecting damage to the kidneys. In addition, it has been reported that KIM-1 levels increase in multiple types of injury, including tubular, interstitial, and glomerular. Further, it was demonstrated that levels of KIM-1 were associated with the severity of kidney injury. 32,36,37
Multiple studies have explored the efficacy of KIM-1 as an indicator of injury in various types of kidney pathology. The effectiveness of KIM-1 as a biomarker of renal scarring has been studied by Toker and colleagues 38 in patients with a diagnosis of vesicoureteral reflux. These authors found a positive correlation between the degree of scarring and KIM-1 levels. In another study, Genc and associates 39 investigated the role of KIM-1 in determining the extent of renal injury in premature infants with respiratory distress syndrome. The study results suggested that serial KIM-1 measurements may be used as a noninvasive indicator of kidney injury in infants as well. Although the study design and population in our investigation differs from these previous studies, KIM-1 levels were significantly higher after the SWL procedure. According to our findings, SWL introduces trauma to the renal tissues and KIM-1 may be a useful biomarker in detecting and monitoring the extent of kidney injury in patients who undergo this procedure.
Although SWL is used worldwide because of its noninvasive nature, it is widely understood that SWL is not free of side effects. To better understand the severity of kidney injury caused by SWL, KIM-1 levels were measured because previous studies indicated that it is a sensitive and specific marker of the degree of kidney damage. After performing a PubMed search, however, we did not find any studies that evaluated KIM-1 as a possible indicator of kidney injury from SWL. As such, this study is the first to address this gap in scientific and clinical knowledge. We plan to investigate further the relationship between various biomarkers of kidney injury after SWL with serial urine collections over a 24-hour period. Therefore, we can say that the main limitation of the study was the lack of gradually measured levels of KIM after the SWL session.
Conclusions
The increased burden of free radical oxidants in the setting of decreasing antioxidant capacity may be one of the initial indicators of AKI after SWL. Moreover, KIM-1 demonstrates great potential as an early and noninvasive biomarker of SWL-induced kidney injury.
Footnotes
Disclosure Statement
No competing financial interests exist.