
Abstract
Purpose:
To analyze the feasibility, safety, and therapeutic effects of retroperitoneoscopic-guided cool-tip radiofrequency ablation (RCRFA) used for the treatment of adrenocortical aldosteronoma.
Patients and Methods:
We performed a retrospective comparison of RCRFA (n=12) and laparoscopic partial adrenalectomy (LPA) (n=26) in the patients with solitary aldosterone-producing adenoma in our center from 2006 to 2009. Intraoperative and follow-up data were reviewed for clinical parameters and hormone levels. Univariate analysis was performed to measure the consistency of these clinical parameters preoperatively and postoperatively.
Results:
All patients presented hypertension, hypokalemia, and high aldosterone/renin ratio (ARR>30) preoperatively and were finally histologically confirmed as aldosteronoma. Technical success rate of these two procedures was 100%. Every patient was followed up for more than 3 years (mean 49.2±15.6 months). There was no evidence of residual or recurrent lesion postoperatively. ARR declined significantly postoperatively compared with preoperatively (54.33±24.90 vs 5.50±3.30 in the RCRFA group and 51.45±29.12 vs 6.67±3.75 in the LPA group, p<0.05). Hypokalemia was resolved in all patients after the surgery. A majority of patients (91.7% in the RCRFA group and 96.2% in the LPA group) were cured without any further need of antihypertensive medication or experienced an improvement in hypertension. Antihypertensive medications reduced significantly after surgical procedures. RCRFA and LPA demonstrated similar therapeutic effects. Compared with LPA, RCRFA provided a shorter operative time (65.6±13.5 minutes vs 86.0±16.5 minutes in LPA, p<0.05), less blood loss (20.0±11.3 mL vs 60.8±52.0 mL in LPA, p<0.05), and lower complication rate (16.7% vs 26.9% in LPA).
Conclusions:
RCRFA might be an alternative for LPA in selected patients with adrenocortical aldosteronoma. Due to limited sample size, more experience is necessary to validate this procedure.
Introduction
T
Despite the development of less-invasive surgical procedures, demand still exists for additional reductions in therapy-related morbidity. Recent technological advances have brought kinds of new, minimally invasive organ-sparing procedures with limited morbidity. Among them, radiofrequency ablation (RFA) therapy has become a safe and efficacious treatment modality for the ablation of neoplasms in a variety of tissues, including the liver, lung, bone, breast, prostate, and kidney. 4 –6 Some reports have also shown a good therapeutic response with RFA on adrenal tumors and metastases. 7,8 Most adrenal tumors are slow-growing benign adrenocortical adenomas, which are good candidates of RFA. Recent studies have mentioned the clinical utility of percutaneous RFA on functional adrenal tumors, such as Cushing's syndrome and primary aldosteronism, and showed promising results. 9 –11 However, there is still a subgroup of patients who may benefit from a laparoscopic rather than a percutaneous approach.
In the present study, we retrospectively analyzed patients' data with single adrenocortical aldosteronoma experienced retroperitoneoscopic-guided cool-tip radiofrequency ablation (RCRFA) for safety and efficacy. Laparoscopic partial adrenalectomy (LPA) through a retroperitoneal approach was also analyzed as control.
Patients and Methods
Patients
From May 2006 to December 2009, we performed RCRFA in 12 selected patients with primary aldosteronism caused by a small (<4 cm), single aldosterone-producing adenoma. Almost all patients were women except for one man, with a mean age of 48.6 years (range 39–60 years). Of 12 tumors, 8 were in the left adrenal gland and 4 were in the right side. During the same period, we did LPA for 26 patients with single aldosterone-producing adenoma, with a mean age of 45.7 years (range 32–65 years). The diagnosis of primary aldosteronism was established by the clinical symptoms, determination of the adrenal hormones in serum and urine and serum electrolytes, contrast-enhanced CT imaging, and the intraoperative biopsy findings. All patients presented clinical symptoms associated with hyperaldosteronism, including hypertension, hypokalemia, and additional symptoms related to hypokalemia (e.g., muscular weakness, paralysis). All patients had elevated aldosterone levels, low renin levels, and were with a serum aldosterone/renin ratio (ARR) of >30. In all cases, CT imaging revealed a well-enhanced mass in the adrenal gland, compatible with adrenocortical adenoma. Adrenocortical adenoma was finally histologically confirmed by biopsy pathology with Tru-Core 22-gauge biopsy needle (Tru-Core™; Medical Device Technology, Gainesville, FL) in the RCRFA group (Fig. 1A).
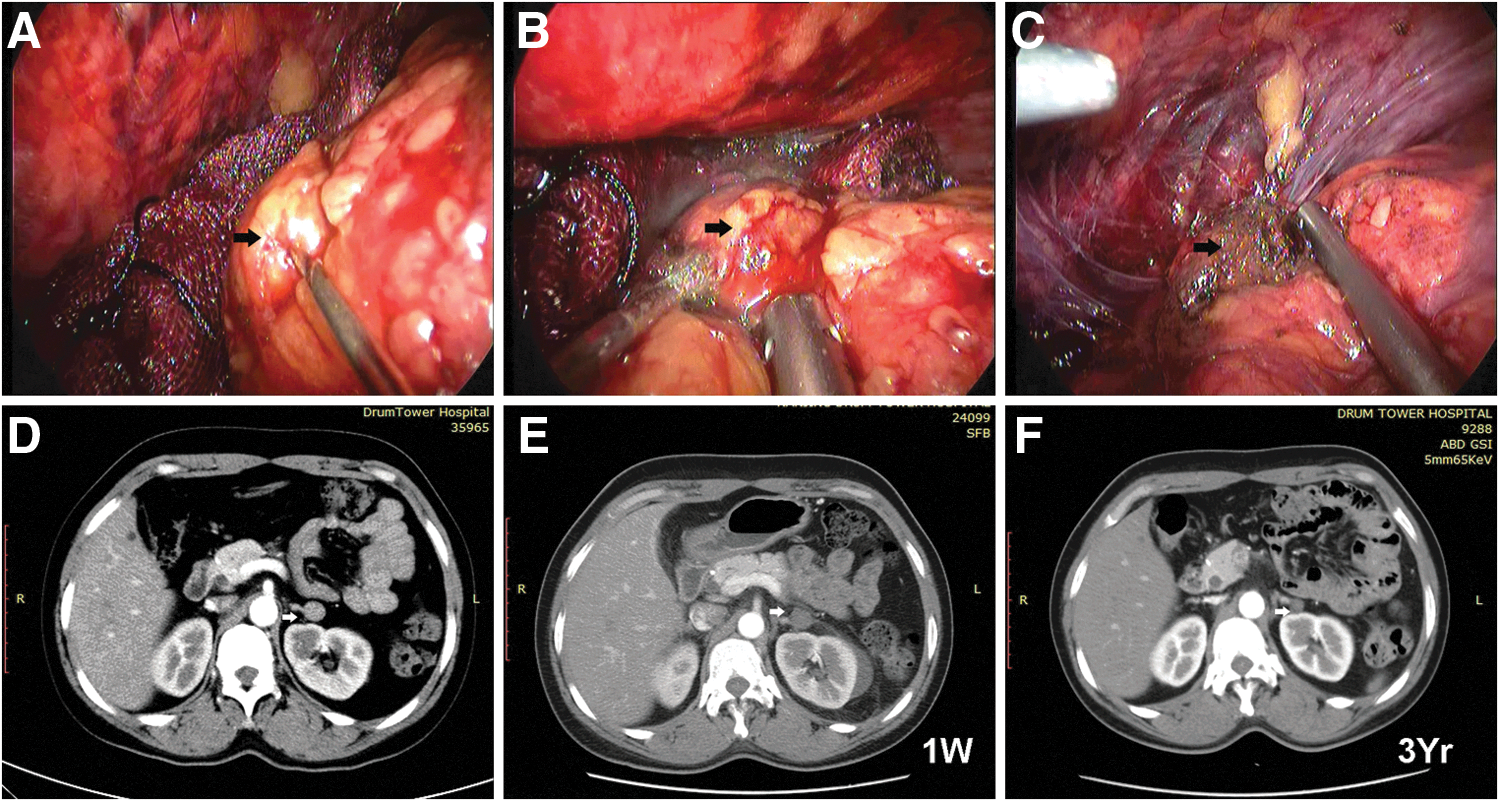
A 43-year-old female patient with a solitary adenoma in the left adrenal gland. The tumor was surrounded by several vital organs (kidney, pancreas, aorta, and intestine).
This study was approved by our institutional review board. All patients provided written informed consent after the nature of the procedures had been fully explained.
LPA (retroperitoneal approach)
All patients were under general anesthesia and were placed in the lateral decubitus position. The creation of a retroperitoneal working space, trocar placement, and the surgical technique of retroperitoneoscopic partial adrenalectomy have been previously described. 12 Gerota's fascia was incised just beneath the diaphragm. Three avascular planes were dissected around the adrenal gland with a Harmonic scalpel. The fatty tissue around the tumor was dissected carefully to identify the margin of the adenoma clearly, and the whole adrenal gland was exposed sufficiently. After clear identification, the adrenal adenomas were resected along with a thin margin of normal tissue using the Harmonic scalpel. After the specimen was removed in an extraction bag, the adrenal gland lesion was confirmed grossly in detail to ensure the adequacy of the excision. A retroperitoneal drainage tube was placed before closing the wounds with absorbable sutures.
Retroperitoneoscopic-guided cool-tip radiofrequency ablation
The cool-tip radiofrequency (RF) ablation system device (Valleylab, a division of Tyco Healthcare Group LP, Boulder, CO) was used as described previously by Arima et al. 13 The patients were under general anesthesia and placed in a latericumbent position. For tumor exposure, we also preferred the same retroperitonescopic approach as LPA but without dissection of the whole gland. Before the start of RF, different types of cool-tip electrode were selected according to varied tumor sizes, which led to varied withering regions. The internally cooled RF electrode (Cool-Tip RF Ablation System; Valleylab) was placed in the center of the tumor under monitoring with laparoscopy and ultrasound. After the electrode was connected with the generator (Series CC-1; Valleylab), RF energy was applied for 3–6 minutes at each site of the tumor using an impedance control algorithm. Cool sterilized water was injected into the retroperitoneal space around the tumor via passageway of laparoscopic sucker to protect the normal adrenal glands and organs or tissues adjacent to the tumor from thermal damage. The water was reabsorbed every 1–2 minutes. The sterilized surgical gauze was placed over the vena cava and other adjacent vital tissues to avoid accidental damage by RF energy.
Follow-up
Routine physical examination and measurement of serum aldosterone, renin, and potassium levels were performed every 3 months postoperatively. Contrast-enhanced CT studies were done 1 week after the surgery and thereafter every 6 months. Tumor enhancement was evaluated by the diagnostic radiologist by measuring CT values. An increase in the CT value of 10 HU or more was considered enhancement. The maximal tumor size was also measured in the RCRFA group. No supplementary hydrocortisone was needed after procedure in all cases.
Technical success was defined as the absence of tumor enhancement on contrast-enhanced CT imaging. Technical failure was defined as an increase in the CT value of 20 HU or more of tumor enhancement. The relapse was defined as a new enhancement of tumor region.
Complications
Postoperative complications were assessed using the revised Clavien–Dindo classification system. Any grade 3 or greater complication was considered a major complication and recorded. 14
Statistics
The data were expressed as the mean±standard deviation. Statistical analysis was performed using SPSS ver. 17.0 (SPSS, Chicago, IL). The Student's t-test was used to compare the mean values of two independent parametric continuous variables. A two-sided p-value of <0.05 was considered to be statistically significant.
Results
The patients' demographics are presented in Table 1. The patients' characters of the two groups were similar. However, the mean tumor size of the RCRFA group is larger compared with the LPA group (2.67±0.54 cm vs 1.81±0.59 cm, p<0.05). Every patient was followed up for more than 3 years (mean 49.2±15.6 months).
Data presented as mean±standard deviation or n (%), unless otherwise noted.
p<0.05 is considered to be statistically significant.
The p-value measures consistency of the parameter preoperative and postoperative.
The p-value measures consistency of the parameter between RCRFA and LPA groups.
Clavien–Dindo grade.
ARR=aldosterone/renin ratio; ASA=American Society of Anesthesiologists; BMI=body mass index; NS=no significance; LPA=laparoscopic partial adrenalectomy; RCRFA=retroperitoneoscopic-guided cool-tip radiofrequency ablation.
All procedures were completed successfully, and no conversion to open surgery was necessary. The RCRFA group showed short mean operating time (65.6±13.5 minutes vs 86.0±16.5 minutes in LPA, p<0.05) and less mean blood loss (20.0±11.3 mL vs 60.8±52.0 mL in LPA, p<0.05). The postoperative hospital stay ranged from 2 to 6 days (mean 2.3±0.65 days in RCRFA vs 3.27±0.92 days in LPA, p>0.05).
The contrast-enhanced CT scan 1 week after the surgery revealed no enhancement in tumor location and a normal blood supply to the remaining normal adrenal tissue in all patients (Figs. 1 and 2 for RCRFA). Technical success rate of these two procedures was 100%. There was no evidence of residual or recurrent lesion in ipsilateral adrenal gland during the following serial contrast-enhanced CT scans. The adrenal tumors in the RCRFA group showed involution over time during the follow-up period. The mean diameter was 1.35±0.28 cm at the end of the follow-up period (p<0.05).
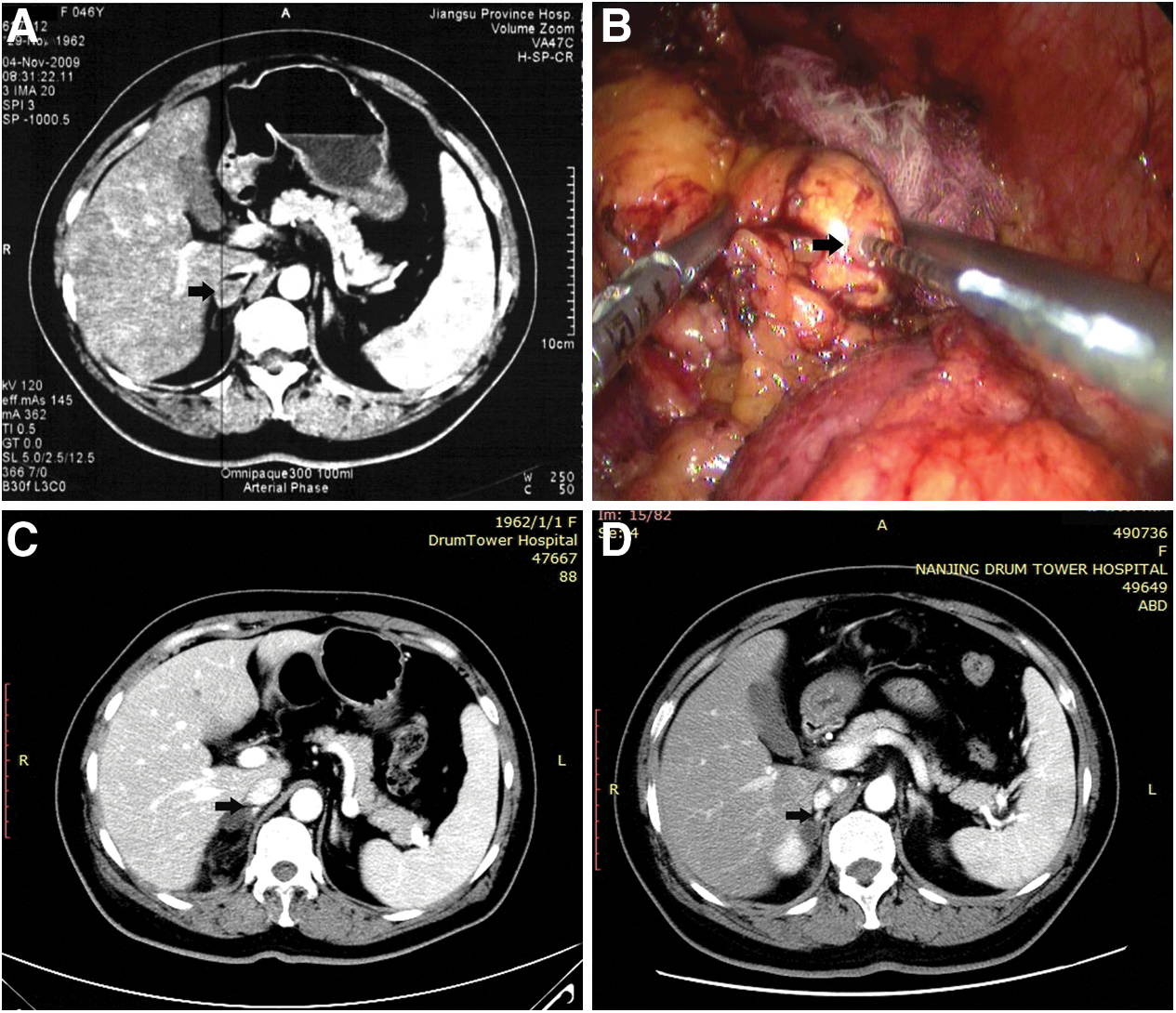
A 46-year-old female patient with a solitary adenoma in the right adrenal gland. The tumor was adjacent to vena cava.
Hypokalemia was resolved in all patients after the surgery. The mean potassium level at the last follow-up was 3.96±0.21 mmol/L in the RCRFA group and 3.82±0.36 mmol/L in the LPA group (p>0.05). Seven patients (58.3%) in the RCRFA group and 15 patients (57.7%) in the LPA group were cured of antihypertensive medications; four patients (33.3%) in the RCRFA group and 10 patients (38.4%) in the LPA group showed improvement of hypertension (fewer antihypertensive medications or reduced blood pressure [BP]); one patient (8.3%) in RCRFA and 1 patient (3.8%) in LPA still suffered unrelieved hypertension (p>0.05). Systolic BP of the RCRFA group decreased from 172.5±11.6 to 137.5±15.6 mm Hg (p<0.05) and diastolic BP from 98.3±8.2 to 81.3±8.6 mm Hg (p<0.05). Meanwhile, systolic BP of the LPA group decreased from 167.3±13.1 to 135.3±14.8 mm Hg (p<0.05) and diastolic BP from 97.1±10.1 to 82.6±7.9 mm Hg (p<0.05). Furthermore, antihypertensive medications could be reduced from 2.25±0.45 to 0.75±0.75 (p<0.05) in the RCRFA group and from 2.11±0.43 to 0.81±0.69 (p<0.05) in the LPA group. The ARR at the end of follow-up decreased significantly compared with the preoperative ARR in both groups (54.33±24.90 vs 5.50±3.30 in the RCRFA group and 51.45±29.12 vs 6.67±3.75 in the LPA group, p<0.05).
Only 2 mild postoperative complications (Clavien–Dindo grade I) occurred following 2 of 12 (16.6%) RCRFA procedures. One patient had paresthesias around the trocar orifice, and the other patient had perinephric hematoma due to intraoperative dissection. They all recovered within 3 months after the surgery. No major complications occurred related to the RCRFA procedures. However, the complications seemed relatively more severe in the LPA group (26.9%). Two patients encountered vascular/tissue (liver) injuries intraoperatively and required further surgical repair. One patient required blood transfusion due to postoperative bleeding (Clavien–Dindo grade II). The remaining four patients had mild postoperative complications (two paresthesias and two perinephric hematoma, Clavien–Dindo grade I) and recovered spontaneously.
Discussion
Laparoscopic adrenalectomy has rapidly replaced open surgery as the gold standard of adrenal surgery since Gagner et al. 15 first described this technique in 1992. In the past decade, LPA has been advocated for small solitary adrenal tumor, which is less traumatic and potentially less hazardous to patients. 3,10,15 –17 Moreover, the preserved adrenal tissue allows total adrenalectomy in cases of future relapse in the contralateral gland. 3,10,16 –18 Therefore, it may offer improved life quality without the need of lifelong hormonal supplementation and reduce long-term morbidity. LPA has been carried out in our hospital since 2000 and it offered very good results, as shown in this article. However, in most cases of LPA, the whole adrenal gland should be exposed sufficiently. When the tumor was located in the venous region of the adrenal gland and normal cortical tissue was identified lateral or proximal to the tumor, the adrenal vein has to be clipped and divided. So in some special cases especially with large tumor sizes, LPA was quite difficult with higher complication rates (vascular/tissue injury and postoperative bleeding) and blood supply to remaining cortical tissue might be damaged, which underscored the need of new organ-sparing treatment modalities.
RFA is a technique that uses alternating RF current to generate localized heat and induces tissue necrosis. 4 The ablated area varied according to the different types of electrode. The damage area can further be adjusted by working power, treatment time, and tissue impedance. 19 Unnecessary normal tissue loss could be limited by choosing proper type of electrode and working parameters. Besides this, RFA also has following additional advantages: RFA has an effect of hemostasis, which could prevent bleeding postoperatively; RFA can even be performed under conscious sedation, which increases the likelihood of the procedure being performed on an outpatient basis. 20 Percutaneous RFA under image guidance has been proposed as an option for adrenal neoplasms by radiologists. Wood et al. 8 first described in 2003 that percutaneous RFA was a safe and well-tolerated procedure for the treatment of unresectable primary and metastatic adrenocortical carcinoma. Arima et al. 13 reported CT image-guided RFA for adrenocortical adenoma with Cushing syndrome as a feasible, safe, and promising treatment. More recently, Liu et al. 21 treated 28 aldosterone-producing adenomas with CT-guided RFA and showed a success rate of 95.8%.
The success rate of percutaneous RFA was influenced by several factors. Among them, tumor size is one of the most important factors. Although percutaneous RFA had been reported to treat adrenal cortical tumors as large as 9 cm in diameter 8 ; in most centers, only the tumors with diameter of <4 cm were selected. On one side, the theoretic damage area of available electrodes was no more than 3 cm, so the tumors larger than 3 cm need more than one session ablation, which increases the possibility of tumor residual. On the other side, the tumors larger than 4 cm are more likely to be malignant (25%), which are not candidates for RFA. 22 Besides the tumor sizes, the tumor location could also influence the success rate of percutaneous RFA for adrenal tumors. 9 For example, some tumors are surrounded by vital organs (e.g., kidney, liver, pancreas, and colon), which will increase the difficulty of electrode placement and the risk of major complications. Another common reason for treatment failure is due to the “heat sink” effect of large vessels (aorta, renal vein, and vena cava) next to the tumors. These vessels are known to dissipate heat, reducing the effectiveness of the ablation procedure. 23
Compared with percutaneous RFA, RFA of adrenal neoplasms through laparoscopic approach could be theoretically carried out with more accuracy and higher success rate in some difficult situations analogous to favoring laparoscopic over percutaneous RFA for the treatment of liver neoplasms. 24 The biggest advantage of the laparoscopic approach is laparoscopic monitoring. The RF electrode could be placed to the ideal site from various directions under laparoscopic and intraoperative ultrasound guidance or by moving the tumor, which is more accurate than percutaneous approach. Meanwhile, laparoscopic approach could help to protect adjacent vital structures during ablating procedure. 24,25 In our early experience, only tumors at the left side were included for fear of thermal damage of vena cava. Then, several protective methods were used in our subsequent practice to avoid possible thermal injury related to RFA. For example, cold water cycling and gauze isolation was engaged to avoid thermal damage of adjacent tissues. If necessary, the tumor was dissected away from big vessels to avoid heat sink effect and damage to the vessels. With these protective methods, laparoscopic RFA was also safely applied in 4 tumors at the right side. In laparoscopic approach, the surgeon can easily observe the developing thermal damage directly or under endo-ultrasound. RFA could be performed easily for an extra cycle or in another site if ablation is considered incomplete. When malignancy was suspected in some rare situation, conversion to laparoscopic adrenalectomy was very convenient. Also, laparoscopic approach is more preferred to urologists than percutaneous approach, as they have relatively more experience with it. Compared with LPA in our institution, RCRFA needed less dissection of the adrenal gland, preserved more blood supply to adrenal gland, and provided a shorter operative time, less blood loss, and less complication. So we trend to use RCRFA to the relatively larger adrenocortical aldosteronoma rather than LPA.
Because the ablative lesions are still left in the body after RCRFA, it is very important to confirm ablative completeness and define local recurrence. Currently, the success of probe ablation is defined as the absence of enhancement at tumor site on serial follow-up contrast-enhanced CT imaging. 8,9,21 Nevertheless, long-term radiographic and clinical follow-up will be required to verify the therapeutic effect of RFA. In present study, the size of ablative lesions was followed up as an indirect parameter of tumor control. The shrunken ablative lesion over time can suggest good tumor control. 26 Meanwhile, the disappearance of relative symptoms, such as hypertension, hyperaldosteronism, and hypokalemia, was also indirect proof of complete ablation. Hypokalemia and endocrinal disorders (high aldosterone and low renin) in all patients were restored immediately after RCRFA, further authenticating the therapeutic effect of RCRFA. However, hypertension was not cured in all patients, which was consistent with the results of laparoscopic adrenalectomy studies. 27,28 The persistence of hypertension in primary hyperaldosteronism patients after surgery was assumed to be caused by an underlying essential hypertension component. One study showed that the prevalence of hypertension was almost the same in these postoperative patients as the prevalence of essential hypertension in a random population of the same age. 29 Patients with long history of hypertension, more than three hypertensive drugs, and elevated serum creatinine levels have an increased risk of persistent hypertension after the surgery. 28
In this retrospective study, there are two noteworthy limitations: small sample size and patient selection bias (tumor size and location). A prospective trial with larger sample size will be carried out in our center to obtain more accurate results.
Conclusions
RCRFA makes it possible to eliminate the lesion without dissection of the whole gland, with short operative time and limited blood loss. It might be an alternative for LPA in selected patients with adrenocortical aldosteronoma. Continued follow-up of patients will provide the long-term efficacy, sequelae, and appropriate patient selection criteria. The results obtained in our preliminary observations indicate that additional evaluation of this procedure by further prospective comparative study would be worthwhile.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Foundation of China (No. 81000247) and Nanjing health distinguished youth fund (JQX-2004).
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.