
Abstract
Purpose:
To evaluate the cost-effectiveness of shockwave lithotripsy (SWL) vs ureteroscopic lithotripsy (URS) for patients with renal stones <1.5 cm in diameter.
Methods:
Patient age, stone diameter, stone location, and stone-free status were recorded for patients treated with SWL or URS for renal stones <1.5 cm in maximal diameter over a 1-year period. Institutional charges were obtained from in-house billing. A decision analysis model was constructed to compare the cost-effectiveness of SWL and URS and using our results and success rates for modeling. Three separate models were created to reflect practice patterns for SWL.
Results:
One hundred fifty-eight patients were included in the study—78 underwent SWL and 80 underwent URS as primary treatment. Single procedure stone-free rates (SFR) for SWL and URS were 55% and 95%, respectively (P<0.0001). Decision analysis modeling demonstrated cost-effectiveness of SWL when SWL single procedure SFR were 65% to 67% or when URS single procedure SFR was 72% to 84%.
Conclusions:
This retrospective study revealed superior SFR results for renal stones <1.5 cm for URS compared with SWL. Our decision analysis model demonstrates that for SWL SFR less than 65% to 67% or for URS SFR greater than 72% to 84%, SWL is not a cost-effective treatment option. Based on these findings, careful stratification and selection of stone patients may enable surgeons to increase the cost-effectiveness of SWL.
Introduction
S
Patients and Methods
Patient identification and selection
Our study was approved by the Institutional Review Board of Rhode Island Hospital before the collection of patient data. All patients who underwent SWL or URS for renal stones of diameters <1.5 cm between June 2010 and July 2011 at Rhode Island Hospital or its affiliate, The Miriam Hospital, were retrospectively identified for possible inclusion in the study. Included patients had data available on sex, age, stone diameter, any follow-up procedures or complications, diagnostic kidneys-ureters-bladder (KUB) plain radiography or CT imaging, a 30-day follow-up KUB or CT scan for evaluation of residual stone burden, and cost.
For the sake of consistency, patients were retrospectively selected such that those whose stone was visible on KUB preoperatively were imaged with KUB postoperatively, and patients whose stone was imaged with CT preoperatively were imaged with CT postoperatively. The standard postoperative pain medication regimen for either procedure at our institution is a 10-day course of hydrocodone-acetaminophen, creating no difference in medication cost between the two treatment groups. Primary outcomes were stone-free status and cost, with stone-free status being defined as no visible stone fragment on the imaging modality of choice (KUB vs CT) at follow-up. Patients with stones not visible on KUB were excluded from the study. All stones proximal to the ureteropelvic junction (i.e., stones in the intrarenal collecting system or renal pelvis) were included for analysis.
Treatment modality was determined by patient preference. Patients were categorized by initial treatment modality into two groups. Group 1 patients underwent SWL under managed anesthesia care with a Medispec EH Lithotripter™ using a power ramping protocol that ramped up through voltages of 15-17-22 kV with rates of 90 per minute (protocols are standardized with regard to rate, targeting, and coupling technique). Group 2 patients underwent URS under general anesthesia with a flexible ureteroscope (no semirigid ureteroscopy was performed) with in situ lithotripsy using a holmium:yttrium-aluminum-garnet (Ho:YAG) laser. Lower pole stones were relocated for lithotripsy.
Chi-square statistics were calculated for categorical variables with the Fischer exact test used to calculate P value, with continuous variables being tested with the Student t and analysis of variance with posttest confirmation of significance via Neuman Keuls. P values were two-sided, and <0.05 was statistically significant.
Decision analysis model
A decision analysis model was constructed using TreeAge Software (Williamstown, MA) to compare the cost-effectiveness of URS vs SWL. The success rates of either procedure in the model were based on our own success rates reported above. Expected value calculations were used to determine whether SWL would be cost-effective compared with URS in managing renal stones. For each treatment, residual stone was considered the failing condition and stone free was considered the successful condition.
Costs per procedure were obtained from the in-house billing department of Rhode Island Hospital whereas professional fees were calculated by the amount charged because there was less variation from patient to patient. Charges included were surgeon's fee, anesthesia fee, facility fee, stent placement, and any auxiliary procedures. Our billing center calculated the costs to include disposable costs and average equipment costs per case, so equipment degradation and eventual cost for maintenance and repairs were amortized and included in the cost per procedure. Imaging fees were not included in the calculations because the same imaging was needed of both patient groups.
We constructed three separate models to represent the various practice patterns for SWL of renal stones (Fig. 1):

Decision analysis models for shockwave lithotripsy (SWL) vs ureteroscopic lithotripsy (URS). Three models represent least, moderately, and most cost-effective algorithms and are based on the practice of whether a physician chooses to perform SWL one, two, or three times before treating with URS.
• Model 1. Least cost effective protocol—three SWL treatments performed before performing URS (assuming stone does not fragment with SWL treatment)
• Model 2. Moderately cost-effective protocol—two SWL treatments performed before performing URS (assuming stone does not fragment with SWL treatment)
• Model 3. Most cost-effective protocol—one SWL treatment performed before performing URS (assuming stone does not fragment with SWL treatment)
Results
Stone-free rates (SFR) and procedure costs
We identified 78 patients for inclusion in group 1 (SWL) and 80 patients for inclusion in group 2 (URS). The same urologist performed all URS procedures, and 37 of 78 SWL procedures, with the remainder of the SWL procedures being split between six other urologists (each of whom perform at a minimum 10 SWL procedures per year and all of whom were overseeing the same, experienced SWL technician). There were no significant differences between group 1 and 2 in age (54±15 vs 47±11, P=NS), percent of lower pole stones (23 of 78 vs 34 of 80, P=NS), or stone diameter (7.00±0.27 vs 7.27±0.27, P=NS).
Of the 78 patients in group 1, 43 (55%) were stone free after initial SWL, while 76 of 80 (95%) patients in group 2 were stone free after initial URS (P<0.001). A total of 10 (12.8%) patients in group 1 and 4 (5.0%) patients in group 2 underwent additional procedures for residual stone fragments (P=0.16), while the remaining 25 patients in group 1 had small residual stone burden on imaging but were asymptomatic and chose not to receive further treatment. There were no Clavien class III or higher complications in either group, nor did any patients need admission for re-treatment, instead obtaining re-treatment on an outpatient basis. There were also no significant differences in the ratio of patients imaged with KUB vs CT between group 1 and 2 (1.80 vs 1.65, P=NS).
Average costs per SWL procedure included the $608 surgeon's fee charge, $1684 anesthesia fee charge, $875 facility cost, and $164 cost for stent placement (13 patients in group 1 received stents) for an average per-procedure cost of $3167. Average costs per URS procedure were $456 surgeon's fee charge, $2475 anesthesia fee charge, $1375 facility cost, and $164 cost for stent placement (all but four patients in group 2 received stents) for a total of $4470. Because there were no significant differences in the imaging modalities used to diagnose and follow up each group, radiologic costs were not included in the analysis.
Decision analysis
Based on our decision analysis model that was created using SFR described above, the SFR for SWL that are necessary to make SWL a cost-effective treatment ranged from 65% (model 3) to 67% (model 1). Alternatively, SWL becomes cost-effective if the SFR for ureteroscopy are less than 72% to 84% (Fig. 2). Put another way, if a urologist using our setup were able to achieve a 67% SFR using SWL, it would be more cost-effective to perform that procedure. Alternatively, if SFR using URS were to fall to 71%, it would not be cost-effective to perform URS as a first-line treatment.
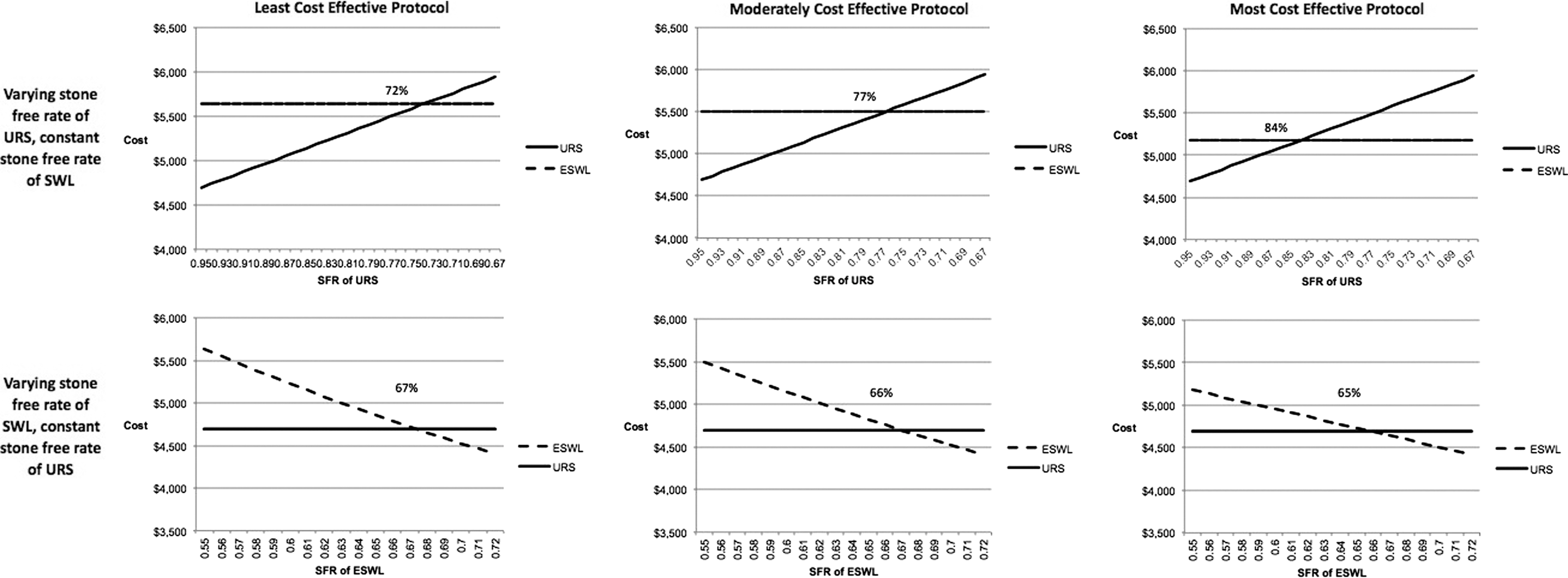
Stone-free rates needed for shockwave lithotripsy (SWL) and ureteroscopic lithotripsy (URS) for SWL to be cost-effective. Calculations made for least cost-effective (three SWL treatments) moderately cost-effective (two SWL), and most cost-effective (one SWL) protocols.
Discussion
SWL and URS are the primary treatment options for patients with renal stones <1.5 cm in diameter, and both are well-tolerated, outpatient procedures. Because the medical and political climate is such that there is increasing consciousness of healthcare costs at large, cost per efficacious treatment is rapidly becoming a critical data point for all treatment modalities. We have identified six studies of the cost-effectiveness of URS in relation to either percutaneous nephrolithotomy (PCNL) or to SWL in the United States between 1995 and 2012 that reported both outcomes relevant to cost-effectiveness of a stone treatment modality (SFR and cost). Of those, three were based on literature reviews for patient data, 3 –5 one compared PCNL with SWL, 6 and one compared PCNL with URS. 7 The sole remaining study was a direct comparison of URS with SWL, but only considered proximal ureteral stones. 8
As with the study by Parker and associates, 8 which examined proximal ureteral stones, our study demonstrated lower costs per stone-free patient using URS as a first-line treatment vs SWL, despite what in our case were higher per-treatment costs for URS. To our knowledge, ours is the first study in the United States to present cost data for renal stones and to calculate cost-effectiveness from our own data set (vs meta-analyses or literature searches) while also providing a decision analysis model demonstrating the effectiveness cutoffs necessary to make either treatment modality cost-effective. In other words, our cost-effectiveness data and predictive models use our own SFR for SWL and URS as predictors instead of relying on historically published data.
In other decision analysis models, other authors have used meta-analyses for prediction of success rates. We deliberately used our own success rates to judge cost-effectiveness in our methodologically consistent practice. We think that by seeing these “real-world” numbers as examples, surgeons in our practice and others can use their own numbers to perform a relative self-assessment of their own SFR with SWL and URS to better make informed decisions on cost-effectiveness.
One interesting aspect of our study is that our data clearly show that cost-effectiveness will be affected by both the efficacy of the lithotripter and also by the efficacy borne out by the surgeon's own skill set. Studies have shown variability of success rates based on the SWL machine used, including many of the machines commonly used today. 9,10 In addition, studies have also demonstrated variation in SFR in series of semirigid and flexible ureteroscopy. 11 Based on the results of our study, we think that it is incumbent on the urologist to evaluate his or her success rates using his or her own equipment and standardized methods and consider the success rates needed in our decision analysis model when considering the cost-effectiveness of a given treatment.
Our study has several limitations. Ours was a retrospective, nonrandomized, patient/surgeon-driven treatment study. There were no significant demographic differences between our groups, however, and because the study was initiated after the completion of all patient encounters, there was no overt selection bias. An additional limitation is that a single urologist performed all of the URS procedures vs multiple urologists performing SWL, but all urologists performing SWL perform enough per year (and are overseeing the same SWL technician who performs SWL as his primary job function) that interurologist skill level should not have played a difference.
Our study took place at only two hospitals, but this enabled us to calculate highly granular charge instead of extrapolating systemically. Our calculated charges failed to take into account convalescence, calls to the nursing triage line, additional clinic visits, or other societal costs (such as missed days at work, patient emotional stress from painful ureteral colic, other), although the medical costs likely far outweigh societal costs.
We also acknowledge that while the aim of this study was cost-effectiveness, patient preference plays a large role in surgical decision making, and that from the patient perspective, there are both pros and cons to either SWL or URS. 12 We are not suggesting that the decision between SWL and URS should be based on cost alone, but we do think that as the healthcare climate continues to pay increasing attention to the effective use of resources, that cost-effectiveness may play a larger role in these decisions in the future.
As noted elsewhere, 5 more high quality cost-effectiveness studies are needed to fully evaluate the optimal management of urologic stones. Unanswered questions include the necessity of achieving a stone-free state and the costs to society of the various approaches.
Conclusions
Our study demonstrated that URS with Ho:YAG lithotripsy yields greater SFR than SWL for renal stones, although both treatment modalities have a low risk of major complication. In addition, if SWL is not successful greater than 65% of the time or if URS is successful more than 72% to 84% of the time, URS becomes the more cost-effective treatment in our model. Given its superior clinical and cost-effectiveness, URS could be considered as the first-line treatment option for patients with renal or ureteral calculi <1.5 cm in diameter who desire a stone-free state.
Footnotes
Acknowledgments
We would like to thank the billing departments of Rhode Island Hospital and The Miriam Hospital for their invaluable assistance in calculating charges.
Disclosure Statement
Dr. Eisner is a consultant for Boston Scientific, Olympus/ACMI, PercSys, and Radius Pharmaceuticals and an owner of Ravine Group. Dr. Pareek is a principal in PRIME Biomedical. For the remaining authors, no competing financial interests exist.