
Abstract
To facilitate robotic nerve-sparing radical prostatectomy, we developed a novel three-dimensional (3D) surgical navigation model that is displayed on the TilePro function of the da Vinci® surgeon console. Based on 3D transrectal ultrasonography (TRUS)-guided prostate biopsies, we reconstructed a 3D model of the TRUS-visible, histologically confirmed “index” cancer lesion in 10 consecutive patients. Five key anatomic structures (prostate, image-visible biopsy-proven “index” cancer lesion, neurovascular bundles, urethra, and recorded biopsy trajectories) were image-fused and displayed onto the TilePro function of the robotic console. The 3D model facilitated careful surgical dissection in the vicinity of the biopsy-proven index lesion. Geographic location of the index lesion on the final histology report correlated with the software-created 3D model. Negative surgical margins were achieved in 90%, except for one case with extensive extra-prostate extension. At postoperative 3 months, prostate-specific antigen levels were undetectable (<0.03 ng/mL) in all cases. The initial experience of the navigation model is presented.
Introduction
I
Cancer abutting or focally extending beyond the prostate capsule increases the risk of a positive surgical margin. 2,3 Thus, intraoperative knowledge of the three-dimensional (3D) location of the biopsy-proven cancer lesion may further improve oncologic outcomes of robot-assisted radical prostatectomy. During preoperative surgical planning and intraoperative decision-making, the only option currently available to prostatectomy surgeons is preoperative imaging (transrectal ultrasonography [TRUS], CT, MRI). As such, considerable intraoperative mental imagination is needed on the part of the surgeon to literally guess the precise location of the prostate cancer lesion.
To facilitate robotic nerve-sparing radical prostatectomy, we developed a novel 3D surgical navigation model that is displayed on the TilePro™ function of the da Vinci® surgical system (Intuitive Surgical, Sunnyvale, CA). The initial feasibility of the technique is presented.
Technology
Technique
Digitalized 3D prostate data and each biopsy trajectory were acquired during prostate biopsy with a 3D end-fire TRUS probe (3D5-9EK TRUS probe and an Accuvix-V10 US machine, Samsung Medison America, Cypress, CA) using an external computer workstation (Urostation®, Koelis, La Tranche, France). In patients who had undergone prebiopsy prostate MRI, we performed biopsies using MR/TRUS elastic image-fusion guidance. 6 Using our team's developed prototype computer software, we reconstructed a 3D model by fusing five key anatomic aspects: 3D surface rendered prostate (pink), TRUS or MRI-visible, biopsy-proven index cancer lesion (orange), neurovascular bundles (yellow), urethra (blue), and color-coded biopsy trajectories (green/red) (Fig. 1). When there were multifocal image-visible biopsy-proven lesions, a 3D model of the nonindex lesions could be additionally reconstructed.

Schematic drawing of the process of creating a three-dimensional (3D) surgical navigation model. Using our developed prototype computer software, 3D surgical navigation models are reconstructed to fuse five key anatomic aspects: 3D surface rendered prostate (pink), image (transrectal ultrasonography [TRUS] or MRI)-visible biopsy-proven cancer (orange), neurovascular bundles (yellow), urethra (blue), and color-coded biopsy trajectories (green/red). Each biopsy trajectory was digitally recorded in real time using 3D TRUS with Urostation® software (Koelis). By image-fusion technique based on the digital coordinates of each recorded needle trajectory corresponding with the coordinates of visible index lesion, we reconstructed a 3D model of the pathologically confirmed index cancer lesion. Note that the distal end of each core was inked at the time of biopsy to orient the biopsy specimen; thus, the extent and location of cancer in the biopsy core can be color-coded as the cancer (red) and benign (green) regions in each biopsy core.
At the time of biopsy, we inked the distal end of each core to orient the biopsy specimen; thus, the pathologist could precisely document the extent and location of cancer in the biopsy core. We digitally color-coded the cancer (red) and benign (green) regions on each biopsy core. Finally, by image-fusing the coordinates of each recorded needle trajectory from the volume data set, we reconstructed a digital image of the pathologically confirmed index cancer lesion.
Segmentation of the five key anatomic models was performed manually using TRUS (gray scale) or MRI (diffusion weighted/apparent diffusion coefficient [ADC]-map or T2-weighted) images. During robotic prostatectomy, the 3D model was presented to the surgeon on the TilePro display of the robotic console simultaneously alongside the intraoperative endoscopic image of the da Vinci surgical system. Orientation of the 3D model was performed manually using a computer mouse by an experienced urologist, in sync with the surgeon's endoscopic view.
3D surgical navigation
The 3D surgical navigation, intraoperatively displayed on the TilePro, enhanced surgeon confidence, specifically while mobilizing the prostate in the vicinity of the biopsy-proven index cancer lesion. (Note: Given that the organ-confined cancer lesion is intraprostatic, it is therefore completely invisible to robotic visualization. It can only be visualized on TRUS and/or magnetic resonance [MR].) As such, the 3D-reconstructed model, based purely on preoperative TRUS/MR, provides the surgeon with a uniquely novel insight as to the actual location of the intraprostatic cancer lesion, thus, in a sense, allowing the surgeon to “look beyond what he/she can see.” This in turn enhances intraoperative capability. TilePro navigation images demonstrated good matching with the actual robotic laparoscopic view (Figs. 2, 3).
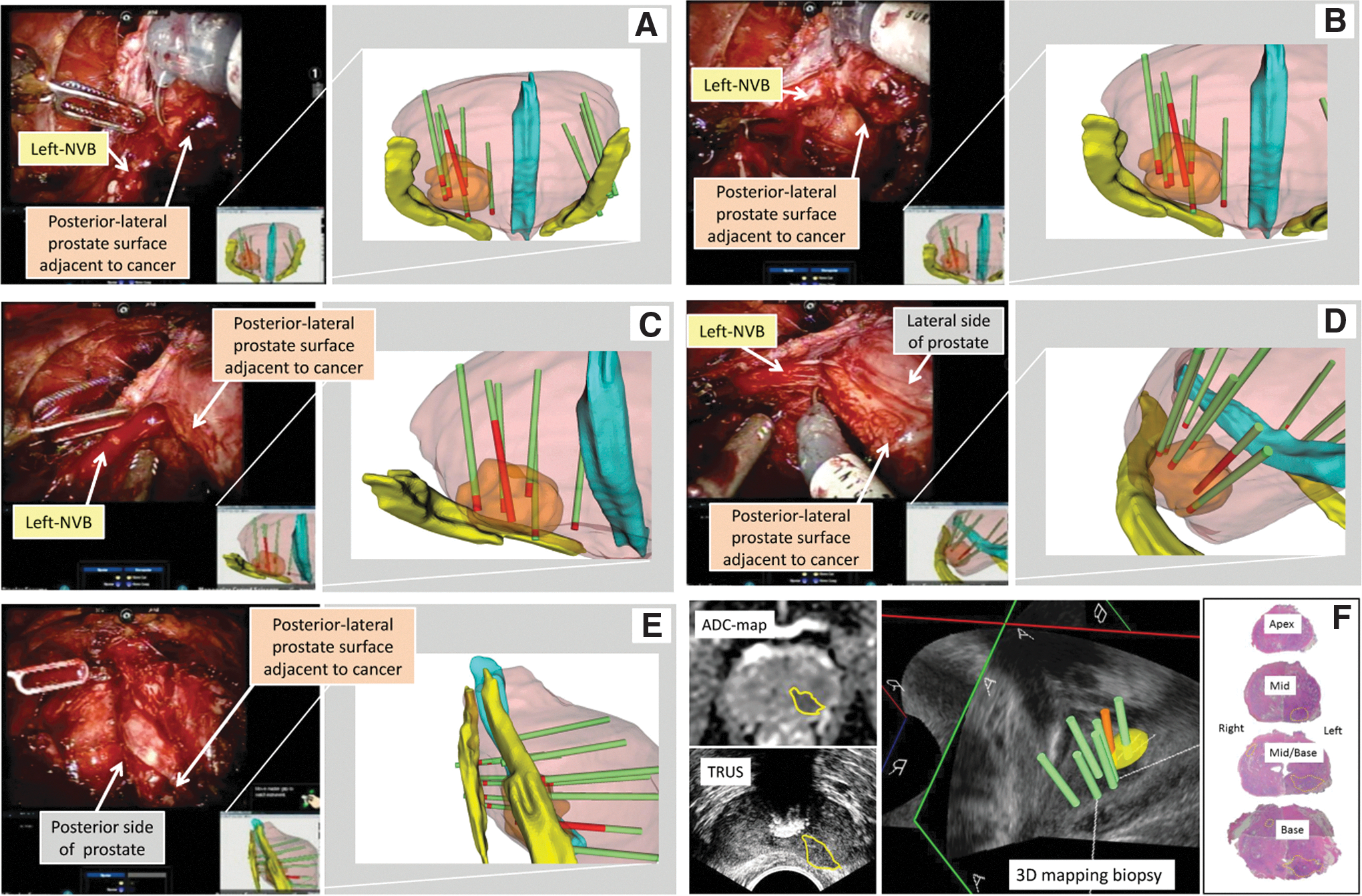
A 71-year-old-man had a prostate-specific antigen level of 5.6 ng/mL and multiple Gleason score 3+4=7 cancer with up to 70% core involvement with visible index lesion, suggestive of extracapsular extension. Surgical navigation provided detailed three-dimensional (3D) geographical location of the index cancer with potential extracapsular extension in contact with the left neurovascular bundle (NVB) (
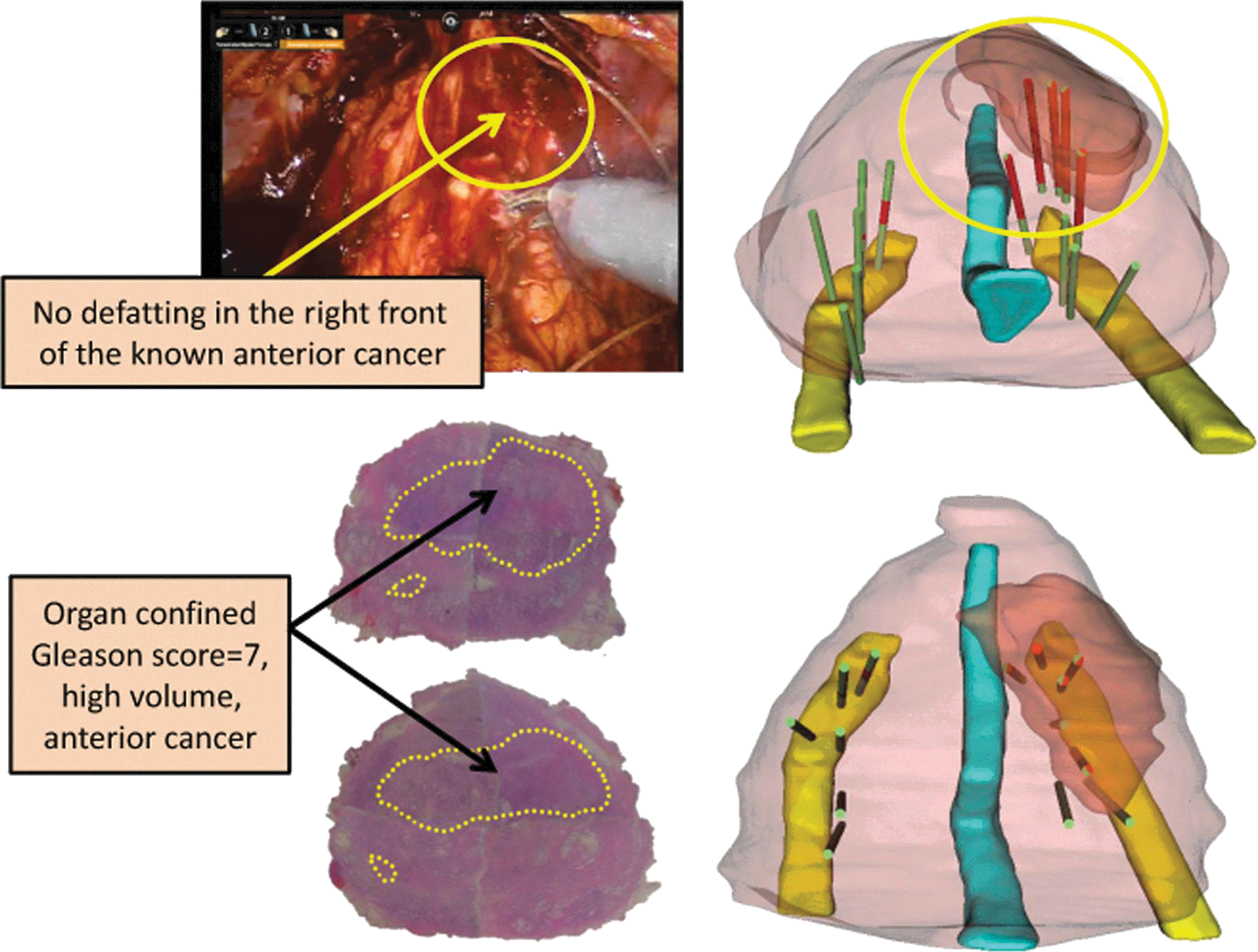
A 69-year-old-man had a prostate-specific antigen level of 7.4 ng/mL and bilateral Gleason 4+3=7 cancer with 60% to 90% core involvement in 7 of 14 biopsy cores using MRI/ultrasonography fusion targeted biopsy. Surgical navigation provided three-dimensional geographical location of the high-volume Gleason 7 cancer located in contact with the right anterior surface of the prostate, with potential risk of extracapsular extension in the right apex. Because the surgeon was preemptively informed about the location of the high-volume Gleason score 7 cancer, the surgeon omitted defatting the right-anterior surface (yellow circle in the surgical view, right figure), thus achieving negative surgical margins.
Additional information regarding extracapsular extension of cancer, which was overlaid with color-coded biopsy trajectories, provided useful information to the surgeon regarding how close to the prostate capsule could the dissection be performed.
Subjects
Ten patients with T1c/T2a prostate cancer diagnosed by 3D TRUS mapping biopsy underwent robot-assisted radical prostatectomy. Median patient age was 71 years (range 51–76 years), serum prostate-specific antigen (PSA) level was 6.3 ng/mL (range 4.6–32.5 ng/mL), biopsy Gleason score was 3+4=7 (range 6–7), mean of cancer core involvement from the index cancer was 60% (range 5–90), and number of positive cores was 4 (range 1–11 of total 13 or 14 cores) (Table 1).
Preop=preoperative; PSA=prostate-specific antigen; RP=radical prostatectomy; postop=postoperative.
Results
Surgical navigation facilitated robotic dissection in the area of the biopsy-proven cancer lesion; to wit, negative surgical margins were achieved in 9 of 10 (90%) cases, except for one case with extensive extraprostate extension.
At postoperative 3 months, PSA were undetectable (<0.03 ng/mL) in all cases. No intraoperative complications (Clavien classification, any grade) and no additional time for surgical procedures were noted. Geographic location of the biopsy-proven index cancer lesion in the simulated models correlated well with pathologic step-sectioned prostatectomy specimens in all cases (Figs. 2, 3). In this series, because no targeted biopsies from secondary lesions were positive, only index lesion per case was created without the model of any secondary lesions. Preoperatively, neither TRUS nor MRI visualized the exact location of the macroscopic extraprostate extension; however, the 3D model intraoperatively demonstrated the area of the biopsy-proven cancer in contact with the prostate capsule, where the potential risk of microscopic extraprostate extension was alerted to the surgeon.
We found that MR-based 3D modeling was superior to TRUS-based 3D modeling. Specifically, TRUS underestimated index lesion volume vis-a-vis MR-based modeling. As such, TRUS-modeled index lesion volume of Case 1 was only 48% of the actual pathologic index lesion volume in step-sectioned radical prostatectomy specimens. The addition of multiparametric MR (additional use of the ADC-map to T2-weighted) improved tumor volume estimation (Fig. 4A); MR-modeled index lesion volume was 82% of the actual pathologic index lesion volume. Finally, when we superimposed digital data of biopsy-proven cancer core length (color-coded in red) (Fig. 4B), modeled lesion volume estimation improved to 90% of actual pathologic volume.

Multiparametric magnetic resonance imaging (MRI) (additional use of apparent diffusion coefficient [ADC]-map to T2-weighted image) improved the tumor volume estimation from 48% to 82% in Case 1 (
Discussion
Recent advances in 3D reconstruction from digitalized images now make it possible to provide intraoperative surgical navigation. Thus, critical anatomic structures that lie beyond the surgical view (for example, an intraprostatic cancer lesion) can now be presented to the surgeon in real time. 2 –6 Providing a real-time two-dimensional navigation image in the TilePro display of the da Vinci surgical system has been reported as a promising approach for surgical navigation. 4,6 To our knowledge, this 3-D model navigation for robotic TilePro display is novel, in that it simultaneously displays 3D surgical navigation images alongside the actual endoscopic surgical view.
The 3D display of the biopsy-proven cancer lesion is based on our MR/TRUS fusion targeted biopsy protocol. 7 Characterization of the clinically important index cancer lesion may be improved by modern, image-guided biopsies compared with the conventional, image-blinded systematic random biopsies. 7,8 Importantly, we are able to digitally record the trajectory of each biopsy within the 3D prostate volume data set. This prostate volume data set is created by 0.3 mm step-scanning with 3D TRUS in real time. Automated 3D TRUS provides an almost continuous scan of the prostate gland, based on which we create a smooth-surface rendered 3D model.
Depiction of these reconstructed images in real time on the da Vinci console provides a potential advantage to the robotic surgeon. For example, knowing the precise geographic location of the index cancer lesion can alert the surgeon to either avoid iatrogenic capsulotomy (at the site where the cancer lesion abuts the capsule), or intentionally perform a measured wider dissection (at the site of focal extracapsular extension) while still achieving partial nerve preservation.
This pilot study has limitations. First, only feasibility of the initial 10 patients with preoperative data is presented to demonstrate proof-of-concept. Second, used as a single modality, gray-scale TRUS significantly underestimates tumor volume. To correct for this, we overlaid the reconstructed digitalized image of the biopsy-proven cancer. Additional uses of fused digitalized MRI data potentially further improve the tumor contouring. Another limitation of our study is that intraoperative orientation of the 3D model on the TilePro display was performed manually not by the robotic surgeon, but by another experienced urologist. To address this, we are developing real-time prostate tracking with a novel TRUS robot that is controllable by the robotic surgeon, with the goal of achieving dynamic 3D navigation. 4 Although promising, additional studies with increased numbers of patients with longer-follow-up data in comparison to conventional technique are necessary.
Conclusion
We seek to render the “invisible” intraprostatic cancer lesion digitally “visible” to the robotic surgeon, thereby potentially improving surgical precision and negative margins during robotic prostatectomy. Based on 3D TRUS-guided prostate biopsies, we reconstructed a 3D model of the TRUS-visible, histologically confirmed index cancer lesion. Five key anatomic structures (prostate, image-visible biopsy-proven index cancer lesion, neurovascular bundles, urethra, and biopsy trajectories) were 3D image-fused and displayed onto the TilePro function of the robotic console. Presented here is a novel concept of displaying reconstructed 3D surgical navigation images on the TilePro system during da Vinci prostatectomy.
Footnotes
Disclosure Statement
Osamu Ukimura is an advisory board member of SonaCare Medical. For the remaining authors, no competing financial interests exist.