
Abstract
Objective:
To determine the preoperative and perioperative predictive factors of morbidity/mortality in patients undergoing percutaneous nephrolithotomy (PCNL), using the Clavien's classification.
Materials and Methods:
We performed a retrospective chart review of patients who underwent PCNL between January 2005 and January 2012. Preoperative and postoperative factors, such as age, obesity, surgical risk, Charlson comorbidity index, stone complexity, access calix, type of dilator used, and surgery time, were evaluated as predictors of complications.
Results:
A total of 354 patients were included in the study. Of these, 56% were women, with the average age of 47±12.5 years. Stone-free rate for noncomplex calculi was 85% and for complex calculi it was 68%. A total of 103 complications were recorded (29.3%). According to the modified Clavien classification system, 32 (9%) were grade 1, 39 (11%) were grade 2, 16 (4.5%) were grade 3A, 8 (2.3%) were grade 3B, 3 (0.8%) were grade 4A, 1 (0.3%) was grade 4B, and 4 (1.1%) were grade 5. In multivariate analysis female gender (odds ratio [OR] 3.1, confidence interval [CI] 1.1–8.0), Charlson score of ≥3 (OR 23.2, CI 3.5–151.1), complex stone (OR 4, CI 1.6–9.6), and duration of surgery of ≥120 minutes (OR 2.9, CI 1.2–6.9) were associated with major complications.
Conclusions:
PCNL is a safe procedure with acceptable efficacy for the resolution of renal calculi. The safety of the procedure should improve, especially to reduce the presence of severe complications (Clavien ≥3). We identified factors that are associated with severe complications: female gender, high Charlson, complex calculi, and surgical length ≥120 minutes.
Introduction
T
Since the first successful percutaneous removal of a renal calculus in 1976, 6 percutaneous nephrolithotomy (PCNL) has become the surgery of choice for kidney calculi >2 cm. 7,8 Despite the advantages compared to open surgery or extracorporeal lithotripsy, the incidence of complications associated with PCNL is reported from 16% to 52.5%, major complications representing only 4.7% in tertiary referral centers. 9 –12 Preoperative factors, such as stone size, location, urinary tract infections (UTIs), and staghorn calculi, have been associated with an increased risk of complications. 13 –16 To standardize surgical outcomes of PCNL in an objective and reproducible way, the Clavien classification system has been modified for PCNL and it is currently considered the standard for reporting surgical outcomes of PCNL. 17,18
In this study we retrospectively evaluated our surgical outcomes of PCNL performed in a tertiary center where PCNL has been performed since 1994. 19 The aim of the study was to determine the preoperative and perioperative prognostic factors of complications associated with PCNL using the modified Clavien classification system.
Materials and Methods
Patients
With the approval of the internal institutional review board, a retrospective chart review was performed on all patients who underwent PCNL by seven surgeons between January 2005 and January 2012.
Only first time, scheduled, elective percutaneous procedures were included. Cases without postoperative nephrostomy (tubeless) and multitract cases were excluded. Patients with bilateral or recurrent lithiasis were considered new events if at least 90 days passed from the initial PCNL procedure. It was considered a single procedure if the PCNL was carried out with a subsequent access through the same tract, even if it was a different surgical time. Patients with positive urine culture received appropriate antibiotic therapy for 48 hours according to susceptibility before surgery; rest of them were given a prophylactic antibiotic (third-generation cephalosporin) 30 minutes before surgery.
Patient clinical characteristics, including age, gender, body mass index (BMI), American Society of Anesthesiologist (ASA) score, past surgical and medical history, Charlson comorbidity index (CCI), UTI, stone characteristics, access calix, dilators, and surgical time, were collected.
Patient's age was grouped as >60 and ≤60 years; BMI was divided into normal (19–25), overweight (25–29.9), and obese (>30). The comorbidities were grouped according to the Charlson rating 20 (classified into three score categories: ≤2, 3–4, and ≥5). Additionally, surgical risk was grouped using the ASA score as <3 and ≥3; it was considered positive for infection if there was a positive urine culture prior to the procedure.
The following surgical variables were analyzed: duration of surgery (divided into <120 and ≥120 minutes from the moment of puncture until the nephrostomy tube was inserted), whether access was through the posterior-inferior calix or another one, and the type of dilator used, with metallic dilators considered the least risky. Analysis of complications was performed according to surgeon experience.
The presence of hydronephrosis was determined through excretory urogram or noncontrasted computerized tomography of the abdomen, and the characteristics of the stone were analyzed, those with volume ≥400 mm2 (stone burden=width×length×π×0.25) 21,22 and those found in three or more collectors or present in kidneys with anatomical alterations being considered complex.
Surgical technique
The percutaneous access was obtained under fluoroscopic guidance in two planes with the patient in decubitus prone position; after puncturing the desired calix, a rigid guide rod was inserted. Dilation of the tract was done with telescopic dilators, which were serial or balloon dilators, depending on the preference of the surgeon; nephroscopy was done through an Amplatz sheath. Ballistic lithotripsy was used for all procedures. At the end of the procedure, a nephrostomy tube was inserted under fluoroscopic monitoring.
Outcome
An adverse outcome was defined as complications within the first 30 days after the procedure, with these categorized in accordance with de la Rosette 18 using the modified Clavien classification system. In the event of complications with the second procedure through the same tract, the more serious complication was used for the analysis. As a secondary outcome, the stone-free rate was considered, this being defined as lack of clinically significant calculi (>4 mm) on a simple abdominal X-ray or noncontrasted computerized abdominal tomography (patients with radiolucent stones) after the third week from the procedure, or if a secondary procedure is not required (shock wave lithotripsy [SWL], ureterorenoscopy, or other PCNL through a new tract).
Statistical analysis
Bivariate analysis was performed calculating the relative risk (RR) (with 95% confidence interval [CI]) to determine the relationship of the preoperative and transoperative factors to complications globally or Clavien <3 or ≥3. The factors that were analyzed were as follows: age >60 years, BMI ≥25, ASA ≥3, positive urine culture, CCI, complex stone, access through a calix other than posterior-inferior, balloon dilator, and duration of surgery ≥120 minutes.
Multiple logistic regression (MLR) was used to determine the specific weight of the factors and a risk index by points was designed to predict complications taking into account the factors that turned out to be significant.
Statistical significance for the bivariate analysis was p<0.05, and for MLR it was p<0.10. The statistical program SPSS version 19, from IBM (Chicago, IL), was used.
Results
Patients and their characteristics
A total of 392 PCNL procedures were performed between January 2005 and January 2012. A total of 354 procedures on 312 patients who met our inclusion criteria were included in this study; of these 174 patients (55.8%) were women. The average age was 47±12.5 years.
Overall, 279 (78.8%) patients were rendered stone free after one procedure, and 71 of these (20.1%) required a second-stage procedure through the same tract for resolution of the residual stones. Stone-free rate for noncomplex and complex stones was 85% and 68%, respectively (Table 1).
ASA=American Society of Anesthesiologist risk score; BMI=body mass index; CCI=Charlson comorbidity index; COPD=chronic obstructive pulmonary disease; SD=standard deviation.
Thirty-eight patients were lost for follow-up. There were no hospital readmissions or deaths recorded.
Postoperative complications
Overall, 103 (29.3%) procedures were associated with adverse events.
Of the 354 procedures, there were 99 complications after first PCNL procedure (1 to 6 complications per patient), including fever in 48, acute renal failure in 14, a Double-J stent due to perforation of the collector system in 13, and Double-J stent due to a leak in the nephrostomy orifice in 12.
Of the 71 procedures that required a second procedure, only 10 (14%) experienced complications, including fever in 7, acute renal failure in 1, blood transfusion in 1, and intensive care requirement in 1. The overall transfusion rate was 1.4%.
Using the modified Clavien classification, those with ≤3 were categorized as follows: grade 0, 251 (70.9%); grade 1, 32 (9%); and grade 2, 39 (11%).
Patients with Clavien complications ≥3 were categorized as follows: grade 3A, 16 (4.5%); grade 3B, 8 (2.3%); grade 4A, 3 (0.8%); grade 4B, 1 (0.3%), and grade 5, 4 (1.1%) (Table 2).
Stratifying complications according to surgeon experience (≥10 and <10 years) were as follows: patients undergoing surgery by the most experienced group (n=129) showed up Clavien rating <3 in 21.7% and Clavien ≥3 in 9.3% and by the less-experienced group (n=225) had Clavien <3 in 19.1% and Clavien ≥3 in 8.8%. It should be noted that the less-experienced group had only 36% complex calculi and its counterpart had 42%.
Prognostic factors
The majority of patients (74.9%) were overweight or obese, 27.4% had high blood pressure, and 12.7% had diabetes; the CCI was low in 85.5%, moderate in 11.3%, and high in 3.2%. Of all patients, 29.1% had a positive urine culture prior to surgery, 38.9% had complex calculi, and 31.4% had hydronephrosis.
Access was via the inferior calix in 96.6% of cases, serial metallic dilators were used in 91% of cases, and duration of surgery was ≥120 minutes in 42.4% of cases (Table 1).
Relationship of factors to comorbidity
Overall, female gender (RR 1.3, 95% CI 0.96–1.9), high CCI (RR 2.6, 95% CI 1.7–3.9), complex stone (RR 2.01, 95% CI 1.4–2.7), hydronephrosis (RR 1.4, 95% CI 1.01–2), and duration of surgery ≥120 minutes (RR 1.8, 95% CI 1.3–2.5) are the prognostic factors associated with overall complications. In the MLR, being a woman (odds ratio [OR] 1.5, 95% CI 0.9–2.5), high CCI (OR 6.5, 95% CI 1.5–27.8), complex stone (OR 2.3, 95% CI 1.4–3.9), and duration of surgery ≥120 minutes (OR 2, 95% CI 1.2–3.3) maintained their prognostic weight as independent factors.
High CCI (RR 2.8, 95% CI 1.3–5.3), complex stone (RR 1.9, 95% CI 1.2–2.8), and duration of surgery ≥120 minutes (RR 1.8, 95% CI 1.1–2.7) were associated with Clavien complication rating <3; the MLR demonstrated that the factor with the greatest impact was complex stone (OR 1, 95% CI 1.1–3.5).
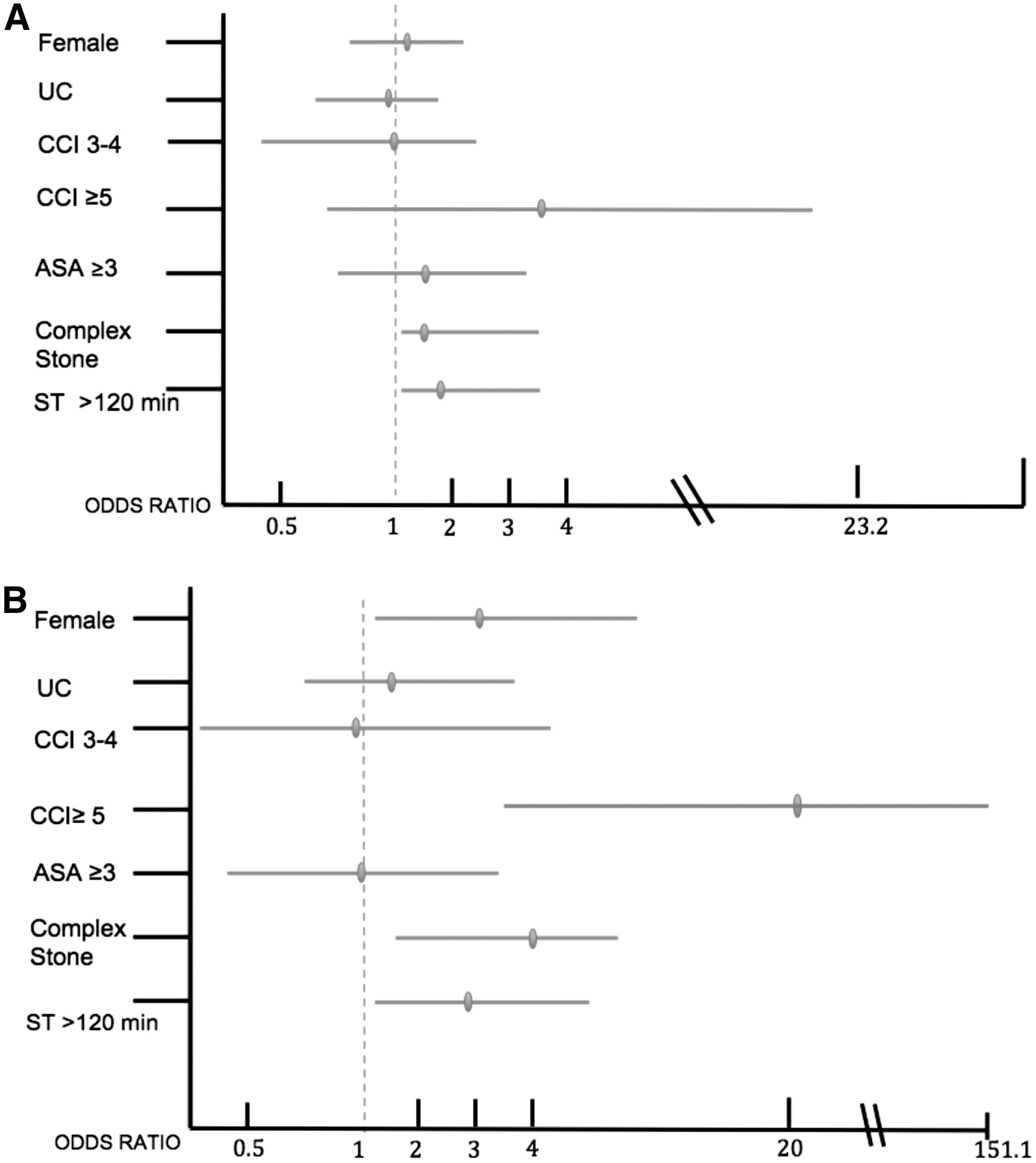
For the presence of a Clavien rating ≥3, being a woman (RR 2.6, 95% CI 1.1–5.9), having a positive urine culture (RR 2.2, 95% CI 1.1–4.1), high CCI (RR 5.3, 95% CI 2.6–11.2), complex stone (RR 3.4, 95% CI 1.7–6.8), and duration of surgery ≥120 minutes (RR 2.5, 95% CI 1.5–5) are factors associated with complications. In the MLR, being a woman (OR 3.1, 95% CI 1.1–8.0), high CCI (OR 23.2, 95% CI 3.5–151.1), complex stone (OR 4, 95% CI 1.6–9.6), and duration of surgery ≥120 minutes (OR 2.9, 95% CI 1.2–6.9) maintained their relationship (Table 3 and Fig. 1).
Risk was calculated excluding the Clavien ≥3.
Risk was calculated excluding the Clavien <3.
CI=confidence interval, RR=relative risk, NA=not available.
An index was designed to predict the risk of Clavien complication ratings <3 and ≥3. It was determined through the following point system: being a woman=1 point, duration of surgery ≥120 minutes=2 points, complex stone=4 points, Charlson ≥5=8 points. The sum of the points determined three levels of risk: slight (1–4), moderate (5–6), and severe (7–8). Overall, patients with slight risk have complications in 14.1% of cases, moderate in 27.6% (OR 2.3, 95% CI 1.2–4.4, p<0.012), and severe in 47.1% (OR 5.4, 95% CI 2.9–9.9, p<0.0005) (Table 4).
Each risk factor has a value that is added if the factor is present. Women=1, surgical time >120 minutes=2, complex stone=4, Charlson ≥3= 8. For example, a woman with a complex stone has a 1+4=5 risk score.
OR=odds ratio; PCNL=percutaneous nephrolithotripsy.
Discussion
According to American Urological Association Guidelines on urolithiasis, PCNL is the procedure of choice for large kidney stones. 23
Our overall stone-free rate was 85%, which is similar to contemporary PCNL series published in the literature. The global PCNL study that included over 5800 patients from 96 centers around the world reported a stone-free rate of 76%, 11 similar to what we found in our study.
The Clavien classification used in our project is the one recently published by de la Rosette et al., 18 in which the specific type of complications are detailed for each grade, noting that the series referenced in what follows used the prior classification in which the particular complication for each grade is not indicated. 9
In the Tefekli series, which had characteristics similar to ours, the Clavien 2 characteristics were the ones reported most frequently, 12 similar to what we found in our study; this is due to the use of antibiotics in addition to prophylactics, which means it gets classified as Clavien 2. Fever secondary to UTIs was reported in different series between 10.5% and 39%, including the percutaneous nephrolithotomy global study (PCNLGS) 16 with a cut-off point for fever (≥38°C).
Clavien complications ≥3 were between 4.13% and 10.9% in the two studies with the greatest number of patients, 12,13 similar to what was found in this study. The cases of death secondary to the surgery were reported at a rate between 0.1% and 0.03% in the different series. In our study, there were four deaths (1.1%): two due to septic shock, one because of bleeding of the upper digestive tract, and the other because of heart failure secondary to pneumonia; in the series in which deaths have been reported, the causes of these have not been indicated. It is notable that we had higher mortality compared with what was reported, although only two of these were considered to be a direct result of the surgery (urosepsis) and two due to medical complications within 30 days of the procedure.
Selection and adequate preparation of the patients prior to the surgical procedure is important to reduce complications. Various published studies have attempted to identify the risk factors that could predict complications. On average, 46% of the population of the studies with larger numbers of patients were women. 11,12 In contrast, in our study 55.8% were women. This is significant since we had a higher number of complications in women compared with men, and a higher risk of complications with Clavien rating ≥3. The studies reported in the literature have not shown differences between men and women on the prevalence of serious complications among women. We found more complex stones and prolonged surgical time in these cases; however, the most significant difference was the presence of a positive urine culture. In our country due cultural and socioeconomic factors, we hypothesize that women have suboptimal nutritional status and a delayed access to health services. 24 –26
Obesity continues to be a major problem for many minimally invasive procedures as a risk factor for complications. Fuller et al. 15 in the PCNLGS study reported that patients with BMI >40 had increased risk of complications with Clavien grade of ≥3 (3.7% vs. 10.5%, p=0.049) compared with patients with normal BMI ranges. Conversely, despite most patients in our series were overweight or obese to some degree, we did not find BMI as a significant predictor of complications. This may be due to advanced skills of our surgeons who have been performing PCNL procedures routinely at a tertiary referral center. This is consistent with previous reports that there is inverse correlation between the number of procedures performed annually and incidence of complications.
The PCNLGS reported 16.2% positive preoperative urine cultures and it was found to have a significant correlation with postoperative fever in multivariate analysis. 16 In our series, it had a tendency toward significance in the bivariate analysis.
Recently, Unsal et al. 20 reported similar study using CCI in patients who underwent PCNL, and demonstrated an increase in complications in patients with CCI >2 (RR 4.4, 95% CI 2.1–9.1); they only referred to complications that required medical treatment. In our series, high CCI was the most important independent factor for predicting a complication with Clavien grade of ≥3.
Tefekli et al. considered 47.7% of cases with complex calculi and they were associated with grade 2 or 3 complications. However, the PCNLGS only indicated whether the calculi in the risk analysis were staghorn or not, finding that complications, positive urine cultures, and longer duration of surgery were associated with the presence of a staghorn calculi. 14 In this study, 138 cases were considered complex calculi, of which 42% resulted in some type of complication. The presence of complex calculi was also shown to be a predictive factor for Clavien complication grade ≥3.
Various studies 12,13,27 have demonstrated that prolonged duration of surgery is a risk factor for complications; in our patients we noted that procedure duration ≥120 min was associated with complications. For this reason, a procedure in two parts might be a better option in those cases in which the duration of surgery might be prolonged.
A greater surgeon experience has been shown to improve surgical outcomes. 28 In our analysis there was no difference in complications between the surgeons with different number of procedures. However, the most experienced group of surgeons performed more complex and challenging cases. All surgeons, but one, had completed their learning curve (60 cases) prior to the start of series included in the study.
Careful patient selection and surgical planning (control of the identified comorbidities) are crucial for successful surgical outcomes. Efforts should be made to limit the operating time to no more than 120 minutes. This can be achieved by compiling a team and their training. For patients with challenging staghorn stones, we recommend to perform a staged surgery. It is preferable to perform a two-step surgery than one extended with potential severe complications. With the intention of having a useful clinical tool for predicting which cases will have complications, we designed a risk index applicable to our population. It involves four risk factors and three risk categories were established. This is the first clinical index reported that attempts to predict the occurrence of complications.
More prospective studies are needed using the Clavien classification proposed by the PCNL global study 18 in order to validate and elucidate its predictive ability. There is controversy that if there is a need for auxiliary treatment at a later time, then extracorporeal lithotripsy and ureteroscopy should be considered part of overall treatment or whether they should be considered a complication, as has already been suggested. 12 We believe that when there were procedures that had not been planned, these should be considered complications 3A and 3B, and we considered them as such in the analysis of our results.
Retrospective design of this study is the main limitation. However, we used standardized methods of data collection and recording of complication to minimize variations and limitations in the study. Prospective studies are needed that would establish the risk factors that could determine the prognosis for patients undergoing this surgery, as well as establish whether female gender is a factor that could indicate whether or not there will be complications.
Conclusions
Percutaneous nephrolithotomy is an efficient and safe procedure with acceptable complication rate. Defining of preoperative factors will help to better select patients and prevent complications and improve surgical outcomes. In our study we identified risk factors that were associated with serious complications, such as female gender, high CCI, complex calculi, and duration of surgery ≥120 minutes. Much attention should be given to these factors in order to reduce the risks of complications after PCNL.
Footnotes
Acknowledgment
The authors would like to thank Dr. María Ocharán from the Instituto Politécnico Nacional for her support during this study.
Disclosure Statement
The authors have nothing to disclose.