
Abstract
Aims and Objectives:
The optimal management method of upper ureteral stones >2 cm is still a challenge. We performed a prospective randomized comparison between laparoscopic ureterolithotomy (LU) and ureteroscopic lithotripsy for upper ureteral calculus >2 cm to evaluate safety and efficacy of both procedures.
Materials and Methods:
Between January 2010 and May 2012, 110 patients with a single radiopaque upper ureteral calculus >2 cm were included in the present study. Randomization was done in two groups—group A: LU was performed and group B: Ureteroscopy (URS) was performed using a 6/7.5F semirigid ureteroscope (Richard Wolf) with holmium laser intracorporeal lithotripsy. Statistical analysis was performed regarding demographic profile, success, retreatment, auxiliary procedure rates, and also complications.
Results:
Out of the total 110 patients, 54 patients were enrolled in group A and 56 patients were enrolled in group B. Mean stone size was 2.3±0.2 cm in group A versus 2.2±0.1 cm in group B (p=0.52). The overall 3-month stone-free rate was (50/50) 100% for group A versus (38/50) 76% for group B (p=0.02). The retreatment rate was significantly greater in group B than group A (8% vs. 0%, respectively; (p=0.01). Auxiliary procedure rate was higher in group B than in group A (26% vs. 0% respectively; p=0.001). The complication rate was 12% in group A versus 26% in group B (p=0.001).
Conclusions:
For upper ureteral stones of size greater than 2 cm, LU has a greater stone clearance rate, comparable operating time, lesser need for auxiliary procedure, and complication rate as compared to URS.
Introduction
T
The optimal management of upper ureteral stones larger than 2 cm is still to be defined.
Ureteroscopic lithotripsy is minimally invasive. However, its efficacy decreases and complication rate increases in upper ureteral stones larger than 2 cm. 3 Laparoscopic ureterolithotomy (LU) has been used for large upper ureteral stones. Although it is more invasive, it gives a chance of complete stone clearance in a single sitting. 4
Prospective randomized studies comparing ureteroscopic lithotripsy and LU are very few. So, we conducted a prospective randomized study comparing the outcome, safety, and efficacy of ureteroscopic lithotripsy and LU for single upper ureteral stones larger than 2 cm, to establish the optimal treatment modality.
Materials and Methods
Institutional ethics committee clearance was taken for the study protocol and all the procedures. Between January 2010 and May 2012, consecutive patients attending the urology outpatient department with a single upper ureteral radiopaque calculus larger than 2 cm, who satisfied the eligibility criteria and were planned for either LU or URS, were enrolled in this prospective randomized study. The upper ureter was defined as the segment of ureter between the pelviureteric junction and the upper border of the sacroiliac joint. Exclusion criteria were stone less than 2 cm, bleeding disorders, radiolucent stones, active urinary tract infection, age >60 years and <15 years, weight >100 kg and <40 kg, comorbid cardiovascular and respiratory illnesses, pregnancy, fever >37°C, serum creatinine >1.5 mg/dL, total leukocyte count >12,000/dL, solitary kidney, coexisting ureteral pathology, including tumor/stricture, and inability to give informed consent.
The eligible patients were randomized into two groups (group A and B) using computer-generated randomization table; group A: laparoscopic ureterolithotomy (LU) and group B: ureteroscopic lithotripsy with holmium laser (URS). Initial evaluation included a detailed clinical history, blood and urine investigations, including complete hemogram, liver function test, kidney function test, serum calcium, serum phosphate, serum uric acid, urine routine microscopy, and urine culture and sensitivity. A 24-hour urine analysis, including calcium, phosphate, and uric acid, was obtained as a routine metabolic workup. Ultrasound kidney, ureter, and bladder (KUB), a noncontrast computed tomography with three-dimensional reconstruction (to know the location and size of the calculus), and X-Ray KUB (to assess radio-opacity of the calculus) were done.
In group A patients, general anesthesia was used. Under cystoscopic and fluoroscopic guidance, a ureteral catheter was placed just distal to the stone. Then, the patient was placed in a flank position. The procedure is performed through three ports. A 10-mm camera port was inserted just superior to the umbilicus. The second 10-mm working port was placed in the iliac fossa. The third 5-mm working ports were placed in the hypochondrium. The arrangement was such that all three ports made an isosceles triangle. After reflection of the colon, the ureter is identified, mobilized, and the stone was located and extracted through a vertical ureterotomy. Using a stone grasper, the stone was extracted through the 10-mm port. Ureterotomy was closed with interrupted 4/0 Vicryl sutures after placement of the Double-J stent through ureterotomy. A small drain is inserted through the 5-mm port. The Double-J stent was removed after 3 weeks. Stone analysis was done in all cases.
In the group B patients, the procedure was performed under regional anesthesia. The procedure was performed using a 6/7.5F semirigid ureteroscope manufactured by Richard Wolf. The holmium laser (Lumenis versa plus 100 W, manufactured by Lumenis Ltd.) was used for intracorporeal lithotripsy. The power setting of holmium laser was 0.6 to 1.2 J. The pulse rate was set between 5 and 15 Hz. Dilatation of the ureteral orifice was done as per requirement and a Double-J stent was placed after the procedure, which was removed at a 3-week follow-up. Stone analysis was done in all cases.
Patient demographics, stone characteristics, and treatment details were the parameters that were studied in both the groups. The outcome variables were the retreatment rates, the stone-free status at 3 months, modified efficiency quotient (EQ), and auxiliary procedure rates. Stone-free status (detected at 3 months by CT scan) after LU or URS was defined as radiological absence of stone, asymptomatic patients with stone fragment less than 3 mm, and sterile urine culture at 3 months or earlier. Modified EQ was used to distinguish between patients who became stone free by LU/URS alone and those who were stone free by any auxiliary procedure. All patients underwent DTPA san and intravenous urography at 3 months and 1 year to check for ureteral stricture.
Microsoft Excel spreadsheet (Microsoft) was used to arrange and record the observations. Data analysis was done by SPSS software version 17.0. The chi-square test was used for categorical variables. Student's t-test and Wilcoxon rank-sum test (group A/B, A1/A2, B1/B2) were used for continuous variables. p-Values less than 0.05 were considered as significant.
Results
A total of 134 patients reported with a single upper ureteral radiopaque calculus larger than 2 cm. Of them, 24 patients were excluded as they failed to satisfy the eligibility criteria. The rest (110 patients) were included in the study and randomized into two groups using computer-generated randomization table: 54 patients in group A (LU) and 56 patients in group B (URS). Ten patients (4 from LU group and 6 from URS group) were lost to follow-up. A total of 100 patients were analyzed in the study (Fig. 1).
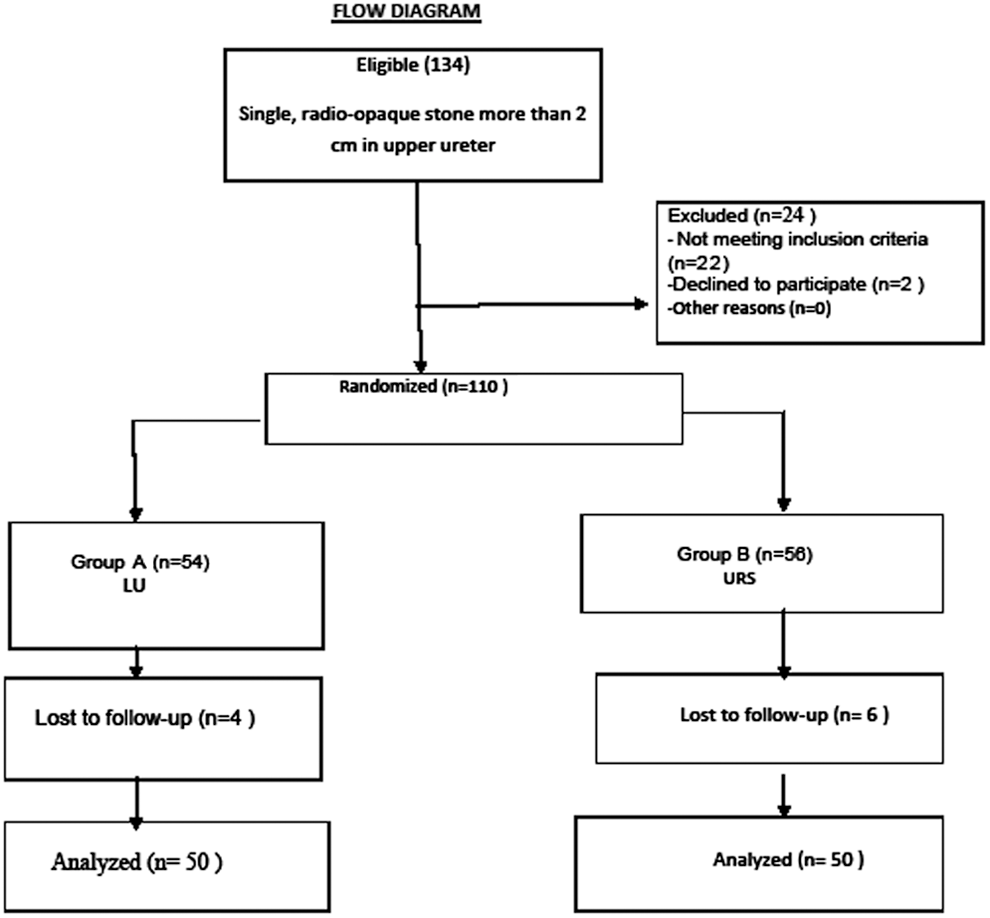
Flow diagram through the phases of trial. LU=laparoscopic ureterolithotomy.
The demographic characteristics, stone location, and stone size of the patients are listed in Table 1. The mean age, sex ratio, height, weight, stone location (right/left), and stone size of the study subjects were comparable between the groups.
Data in mean±SD.
Data in number.
NS=not significant.
The treatment outcomes are summarized in Table 2. The operating time and hospital stay between the groups were not significantly different. The retreatment rate and number of auxiliary procedures required were significantly higher in group B (URS). The stone-free rate at 3 months was significantly higher in group A (LU). There was no conversion from laparoscopy to open surgery in the LU group. Modified EQ, which includes the retreatment rate of each patient for complete stone clearance, was significantly higher in group A (LU) as compared to group B (URS).
Data in mean±SD.
Data in number (percentage).
Data in percentage.
EQ=efficiency quotient; S=significant.
The stone composition and degree of hydronephrosis between the groups were comparable (Tables 3 and 4) and this had no effect on the treatment outcome. The complication rates between the subgroups are summarized in Table 5. In group A, the most common complication was pain, but could be managed with oral and parenteral analgesics and in group B, it was urinary tract infection, managed with oral antibiotics and stone upmigration, needing auxiliary procedures (percutaneous nephrolithotomy). The rate of urinary tract infection and stone upmigration were significantly higher in group B patients. Out of 100 patients, only 2 patients, 1 in each group had hematuria, but it could be managed conservatively without any blood transfusion. The overall complication rate in group B was significantly higher than group A. There were no deaths in either group.
Data in number (percentage).
Data in number.
Data in number (percentage).
Complication grade: grading is as per the Clavien–Dindo classification of surgical complications.
Discussion
The management of upper ureteral stone depends mainly on the size of the stone, associated intensity and duration of pain, obstructed or nonobstructed drainage, cost and availability of instrument. 5 Stones less than 5 mm are more likely to be expulsed by medical expulsive therapy. Most of the upper ureteral stones require intervention because the spontaneous expulsion rate is only 22%. 6
SWL is commonly used for treatment of upper ureteral stones. Its advantages are noninvasiveness, safety, and no requirement of any anesthesia. It can be done as an outpatient procedure. With the newer generation machines, the analgesic requirement and complication rate have decreased. 7 There is a high success rate of SWL as first-line management for stones less than 1 cm but for stones larger than 1 cm, it may require multiple sessions and has a lower success rate. The high initial cost of establishment is also a disadvantage. 8,9
URS is one of the most common modalities used for upper ureteral stones. It is minimally invasive, has a good stone clearance rate, and cosmetic value. Ureteroscopy with holmium laser lithotripsy is less affected by the stone size; the efficacy has been well established for stones larger than 1 cm. The disadvantages being stone upmigration and a higher retreatment rate for larger stones. 10,11
LU can be done through the transperitoneal or retroperitoneal route. The initial series reported the retroperitoneal approach but subsequently, the transperitoneal approach also became popular and both the approaches have established themselves in the management of upper ureteral calculi. 12 –16 The advantage of LU is complete stone clearance in a single sitting. 16 Bove et al. compared retroperitoneal and transperitoneal LU and suggested that in expert hands, both the approaches are feasible, and the choice depends on personal preference. 17
Literature comparing LU and URS is sparse. Ko et al. compared 71 patients of LU with 32 patients of ureteroscopic ureterolithotripsy in patients with stone size over 1.5 cm. They concluded that LU has advantage over the latter due to a high stone clearance rate (100% vs. 77%) in a single procedure. 18 Fang et al. included 50 patients in a study comparing LU and ureteroscopic holmium laser lithotripsy. In their study, LU had a higher stone clearance rate and shorter operation time compared with ureteroscopic lithotripsy. 3 In a prospective study, including 48 patients with stone size more than 1 cm, Lopes Neto et al., compared SWL, LU, and URS. The stone clearance rate was significantly higher in the laparoscopy group (93.3%) as compared to the URS (62.5%) and SWL (35.7%) group. 19 In our study, we compared LU with URS for upper ureteral stones larger than 2 cm. In our study, the stone clearance rate was 100% in the LU group and 76% in the URS group at 3 months of follow up.
As far as complications are concerned, stone migration into the kidney, ureteral perforation, open conversion, and ureteral stricture were observed more frequently in the URS group, but the difference was not statistically significant. LU required a prolonged operative time, longer hospital stay, and more blood loss. 3,18 –20 In our study, the operative time and hospital stay were not significantly different between two groups, whereas the stone upmigration, need for auxiliary procedure, and overall complication rate in the URS group were significantly higher compared to the LU group.
Our study showed that, for upper ureteral stones larger than 2 cm, LU provided a better chance of cure in a single setting with fewer retreatment and complication rates. Further prospective randomized studies with more number of cohorts are required to establish the role of LU as a primary treatment modality in such cases.
Conclusion
For upper ureteral stones of size greater than 2 cm, LU as compared to URS has a greater stone clearance rate, comparable operating time, and lesser need for auxiliary procedure and complication rate. We support the use of LU as a primary modality for upper ureteral stones >2 cm.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.