
Abstract
Purpose:
To provide clinical outcomes of the Resonance metallic ureteral stent in patients with malignant ureteral obstruction, as well as clinical factors predicting stent failure.
Methods:
Cancer patients who have received Resonance stents from July 2009 to March 2012 for ureteral obstruction were included for chart review. Stent failure was detected by clinical symptoms, image studies, and renal function tests. Survival analysis for stent duration was used to estimate patency rate and factors predicting stent failure.
Results:
A total of 117 stents were inserted successfully into 94 ureteral units in 79 patients. There were no major complications. These stents underwent survival analysis and proportional hazard regression. The median duration for the stents was 5.77 months. In multivariate analysis, age (P=0.043), preoperative serum creatinine level (P=0.0174), and cancer type (P=0.0494) were significant factors associated with stent failure. Cancer treatment before and after stent insertion had no effect on stent duration.
Conclusions:
Resonance stents are effective and safe in relieving malignant ureteral obstructions. Old age and high serum creatinine level are predictors for stent failure. Stents in patients with lower gastrointestinal cancers have longer functional duration.
Introduction
U
A unique design of ureteral stent is the Resonance metallic ureteral stent (Cook Medical, Bloomington, IN). Made of a continuous unfenestrated coil of nonmagnetic nickel-cobalt-chromium-molybdenum alloy, the full-length stent allows a 1-year indwelling time, according to the manufacturer.
The use of the Resonance stent was first reported in 2006 in a 64-year-old woman with metastatic breast cancer, 7 followed by a series including both benign and malignant diseases. 8 –18 Eight of these studies have included the follow-up results regarding malignant ureteral obstructions in up to 27 patients 8 –15 ; only three of them have analyzed risk factors of stent failure. We hereby provide our experience on stent duration with clinical factors predicting stent failure.
Methods
The local Institutional Review Board approved this retrospective study and waived the informed consent requirement.
In our hospital, the antegrade method of stent insertion is performed by radiologists under local anesthesia, and the retrograde method by urologists under general anesthesia. Routine follow-up studies include urinalysis, renal function test, plain radiography, and renal ultrasonography. Additional studies such as urine culture, antegrade pyelography, computed tomography (CT), or magnetic resonance imaging (MRI) are performed if clinically indicated.
All cancer patients who have received Resonance stents from July 2009 to March 2012 for malignant ureteral obstruction were included for chart review. Patients with only failure attempts of insertion were not included. Bilateral ureters in the same patient were viewed as individual ureteral units (UUs), and repeated stent insertions into the same UU at different times were counted separately. Patient profiles and laboratory data were collected. Stent-related complications were reviewed. Urinary tract infection (UTI) was defined by a positive culture with urinary symptoms. Images before and after the procedure were reviewed to confirm the resolution and the recurrence of obstruction.
The Kaplan-Meier model was used for survival analysis of the stents. The duration of each stent was counted from the day of insertion to the day of removal, or to the day when percutaneous nephrostomy (PCN) was performed. For those who decided not to have the stent removed because of terminal disease status, the date of stent failure was defined as the date of progressive hydronephrosis confirmed by image study. For patients who died or missed the follow-up before stent failure, the data were considered censored in survival analysis.
Patient factors regarded as possible risk factors for stent failure include: Age (as continuous variable), age ≥60 years (as dichotomous variable), serum creatinine level (as continuous variable), serum creatinine ≥2 mg/dL (as dichotomous variable), cancer types, and treatment for cancer before and after stent insertion (operation, radiotherapy, chemotherapy, and target therapy). These were included for univariate and multivariate analysis using the Cox proportional hazard regression model.
Statistical analyses were performed using free software (R® version 2.14.1). All statistical tests were two-tailed, with P<0.05 considered to indicate significance. To account for potential correlation between multiple stents in the same patient, we used methods that account for correlated data when plotting the Kaplan-Meier curve with robust variance estimates. Also, P-values from Cox models were based on robust variance, which accounts for correlated data.
Results
From July 2009 to March 2012, 79 cancer patients with malignant ureteral obstruction underwent Resonance stent insertion in our hospital. These patients were followed until the end of May 2012. The male-to-female ratio was 22:57. The mean±standard deviation (SD) age was 59.9±12.2 years (range 32–85 years). The mean±SD body height was 157.7±7.3 cm (range 130–174.2 cm), and the mean±SD body weight was 55.2±13.7 kg (range 35.8–108.2 kg). The mean±SD body mass index body mass index was 22.1±4.76 kg/m2 (range 14.5–35.7 kg/m2). Cervical cancer was the most frequent type of malignancy (19 patients), followed by colorectal cancer (17 patients), gastric cancer (9 patients), and ovarian cancer (9 patients) (Table 1).
GYN=gynecologic; UGI=upper gastrointestinal; LGI=lower gastrointestinal; GU=genitourinary.
A total of 117 stents were inserted successfully into 94 ureteral units in 79 patients. There were 74 stent failures (8 from UTI, 3 because of severe pain, 3 from migrations, and 60 because of progressive hydronephrosis) during follow-up. Of the management of these failures, 38 stents were replaced, 17 ureters underwent pigtail external drainage, 1 ureter received an ipsilateral stent, and 18 ureters had conservative treatment. The median functional duration was 5.77 months (95% confidence interval [CI] 4.03–8.7 months) (Fig. 1). The 3-month and 6-month patency rates were 65.16±5.71% and 44.4±6.69% (Table 2).
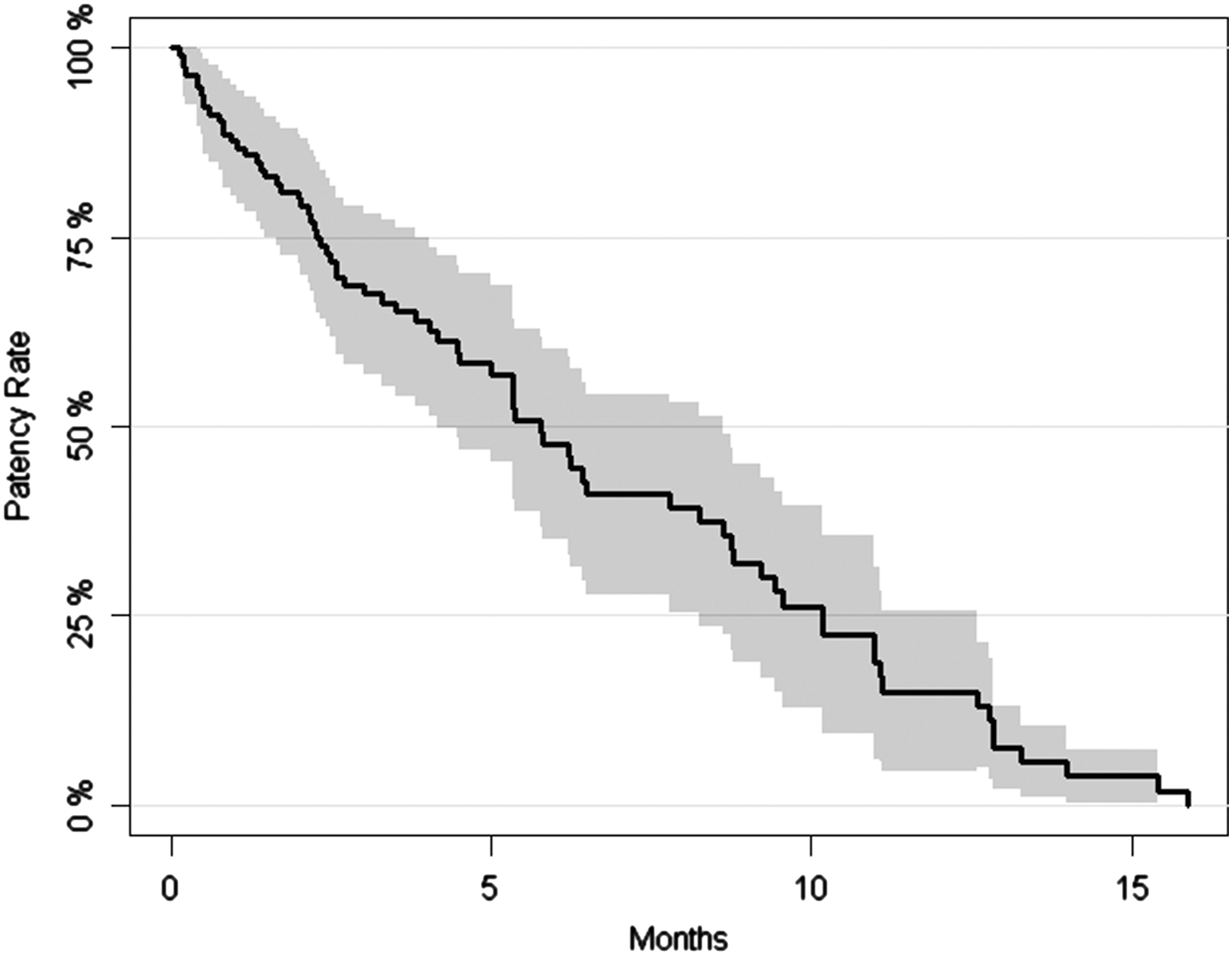
Kaplan-Meier curve for all stents (with 95% confidence interval).
CI=confidence interval; LGI=lower gastrointestinal; Cre=creatinine.
Possible risk factors for stent failure were analyzed with Cox regression model. Age and serum creatinine level were both significant in univariate analysis. The hazard ratio was 1.938 (95% CI 1.079–3.482) for age ≥60 years and 2.599 (95% CI 1.42–4.757) for serum creatinine ≥2 mg/dL, respectively. Sex, degree of hydronephrosis, treatment for cancer, and occurrence of UTI were not significant (Table 3). After controlling for age and preoperative creatinine level, lower gastrointestinal (GI) cancer showed a lower risk than genitourinary (GU) cancer (P=0.0494) (Table 4). The Kaplan-Meier curves showed differences of the duration of stents according to cancer types, age, and preoperative creatinine level (Figs. 2 –4). The median functional duration and patency rates of different groups were shown in Table 2.
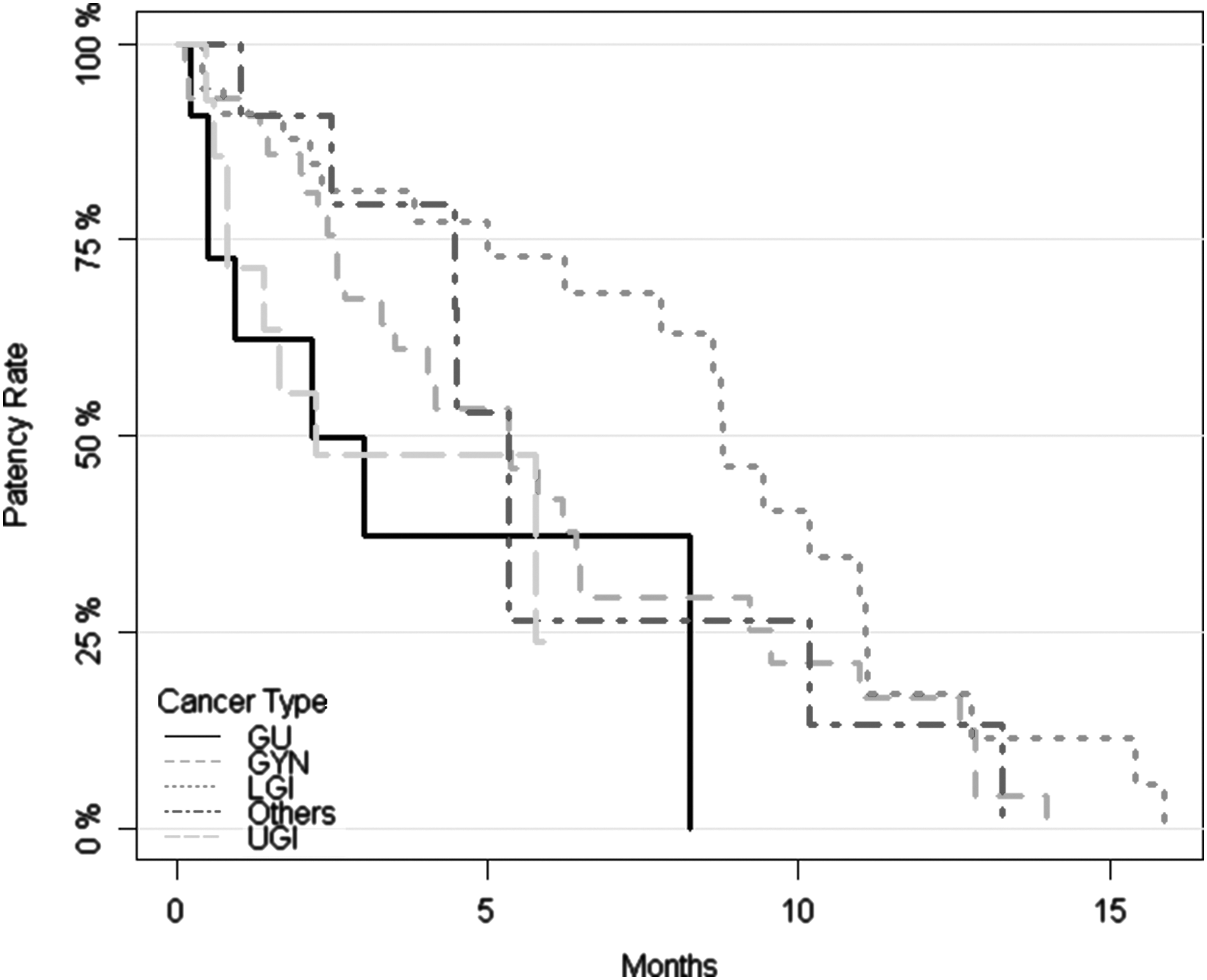
Kaplan-Meier curve of stents grouped by cancer types. GU=genitourinary; GYN=gynecologic; LGI=lower gastrointestinal; UGI=upper gastrointestinal.
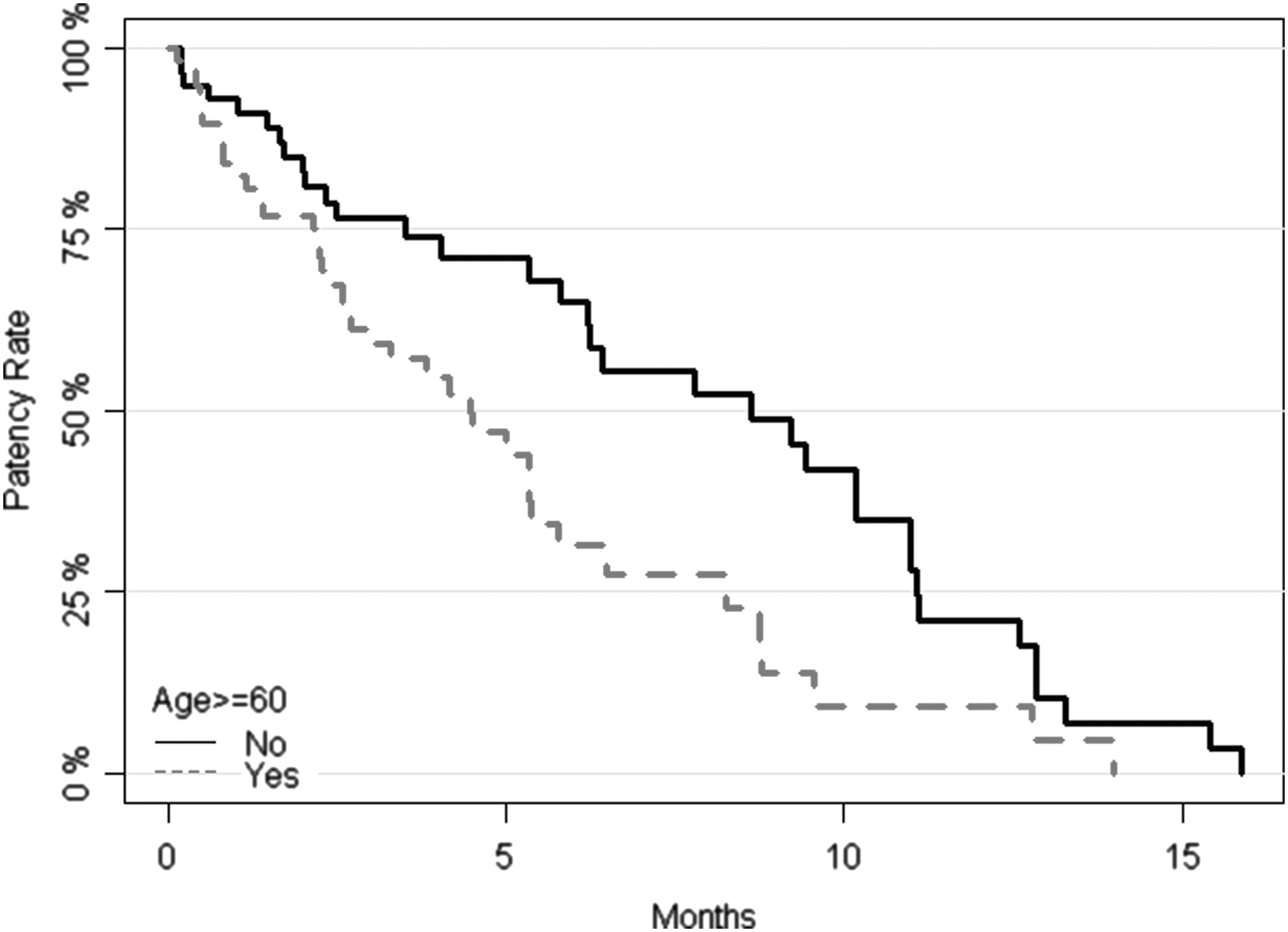
Kaplan-Meier curve of stents grouped by age.

Kaplan-Meier curve of stents grouped by preoperative creatinine level.
* p-value <0.05; ** p-value <0.01.
CI=confidence interval; Cre=creatinine; GYN=gynecologic; UGI=upper gastrointestinal; LGI=lower gastrointestinal; GU=genitourinary; UTI=urinary tract infection.
* p-value <0.05.
CI=confidence interval; GYN=gynecologic; UGI=upper gastrointestinal; LGI=lower gastrointestinal; GU=genitourinary.
No major complications were reported. From the 117 stents, there were 10 patients with gross hematuria, 8 with dysuria, 3 with flank pain, and 5 with urinary frequency. UTI developed in 25 patients in 33 stents. There were three stent migrations in two patients.
Discussion
In our study of 117 Resonance stents in 79 patients with malignant ureteral obstruction, the overall median functional duration was 5.77 months. Age, preoperative creatinine level, and cancer type were independent risk factors for stent failure in multivariate analysis. Sex, degree of hydronephrosis, cancer treatment before and after stent insertion, and occurrence of UTI were not associated with functional duration of the stents.
The Resonance stent, with its unique design, is expected to offer longer durations against extrinsic compressions. The first report of successful clinical use of the Resonance stent was in a patient with retroperitoneal fibrosis resulting from metastatic breast cancer, and the stent lasted 4 months. 7 In most series, the median duration ranged from 3.5 to 11 months. 9 –13 In our study, the median duration for the Resonance stent was 5.77 months. Including the present study, no major complications have been reported. Although the results vary between the studies because of obvious differences in the patients' backgrounds, sample size, and etiology of malignancy, the safety and efficacy of the Resonance stent is established.
Before our study, three studies had assessed the risk factors associated with the failure of Resonance stents. In a cohort of 19 patients including malignant and benign obstructions, Wang and associates 12 indicated that the proportion of patients with previous radiation therapy was significantly higher in the failure group. On the contrary, by analyzing 25 patients with malignant ureteral obstruction, Goldsmith and colleagues 13 found that radiation was not associated with stent failure. They also found that GU cancer was a predictor of stent failure, but age was not in univariate analysis. 13 Brown and coworkers 14 observed more UTI in the obstruction group than in the patent group.
In our study, age was an independent risk factor for stent failure in multivariate analysis, and radiation before or after stent insertion had no effect on stent duration; neither did UTI. Stents in patients with GU cancer had shorter duration compared with other types of cancers, and after further dividing cancers into different groups, stents in patients with lower GI cancer had significantly longer duration. The effect of preoperative creatinine level was not assessed in the previous studies and was shown to be related to stent failure for the first time.
From our results, age, preoperative creatinine level, and cancer type were associated with stent duration. The effect of age on stent duration can be multiaspect. In cancer patients, older age might be related to more advanced disease and more rapid cancer progression, thus affecting stent durations. Patients with older age might also have more comorbidities and be more susceptible to UTI, resulting in more prompt stent replacement or external drainage than younger patients.
The relation between high preoperative serum creatinine level and stent failure might be inadequate urine production, which could cause encrustation on the stents more easily and thus affect stent duration. Liatsikos and colleagues 10 observed encrustation in 12 of 54 stents in patients with benign and malignant disease, but the effect of encrustation on stent duration was not analyzed. Because of insufficient information about stent encrustation from medical records, we could not analyze it either.
In our cohort, patients with lower GI malignancies had significantly longer stent durations, while treatment modality did not appear to be related. One possibility is that lower GI malignancies, either primary or metastatic, have texture and composition softer than other types of malignancies and cause less compression to ureters. Therefore, the Resonance stents could be more sustainable in patients with lower GI malignancies. These possible explanations remain only hypotheses, and further study is needed to investigate the association between these factors and stent duration.
No studies yet have compared directly different metallic ureteral stents. One of the widely used metallic ureteral stents is the Memokath stent (PNN Medical, Denmark). The dual expansion stent is a semi-permanent, nickel-titanium alloy spiral stent of varying lengths (120–200 mm) with a lumen. 19 In a series that consisted of 73 patients, the average indwelling time of an individual Memokath was 11.2 months. 20 One major structural difference between the Memokath stent and the Resonance stent is that the Memokath stent has a lumen, but the Resonance stent does not. Further study is needed to investigate the advantages of metallic stents with or without lumens. Nonetheless, the unique design of the Memokath 051 stent produced significantly less stent-related urinary symptoms compared with conventional Double-J–shaped stents. 21
The definition and detection of stent failure is largely clinical: We take both imaging and functional studies into account when deciding to remove a stent or place a PCN. For those who need hospice care and refuse further diversion (which consisted of 18 stents in 14 patients in our cohort), the date of progressive hydronephrosis was defined as the date of stent failure. The progressive hydronephrosis was often detected earlier than marked elevation of serum creatinine. One explanation could be the compensation of the contralateral functioning kidney, stabilizing overall renal function after stent failure in one side. Another explanation could be the intentionally infrequent blood test in those patients, resulting in a delayed confirmation of creatinine elevation. In any case, stable residual hydronephrosis would not be regarded as a sign of stent failure.
To confirm the occurrence of stent dysfunction is not always easy in clinical practice and to accurately define the specific time point of stent failure is even more challenging. In our retrospective study, the date of stent removal or PCN insertion was used as an approximation or surrogate of the actual failure date, and this is also the definition used by previous series. Using the same criteria is helpful for comparison between different studies. To better define stent failure, however, a strict follow-up protocol in a prospective cohort is needed.
The decision whether to receive a Resonance stent should be made between the patient and the clinician. The aim of our study is to provide more information regarding the functional outcome of the stent and possible risks of failure. Whether these outcomes meet the expectation of the patient could vary between individuals. Patients older than 60 years (median patency 4.47 months) might still benefit more from the Resonance stent than regular stents or external drainage, while the benefit might be less significant in patients with a preoperative serum creatinine level >2 mg/dL (median patency 2.57 months). Permanent PCN seems to affect quality of life more; therefore, it is often reserved as a second-line therapy.
Compared with the other studies, there are several advantages of our study: A relatively large patient number receiving Resonance stents, a relatively homogenous cohort consisting of only cancer patients, the use of survival analysis for duration of the stents instead of crude failure rate, and the use of a multivariate regression model to control confounding factors.
Our study does have some limitations, however. First, this is a retrospective study. Second, instead of receiving Resonance stents as soon as hydronephrosis developed, most patients had failure of regular polymeric stents before they had metallic stents. This delayed use of a metallic stent might make the duration of the stents shorter than it should have been; the cancer might have progressed, so there is a potential selection bias from the cohort. Third, there were three migrated stents that could have stayed longer in the ureter if they had not migrated. Whether a migrated stent should be considered a failure remains controversial, and the functional duration would be slightly increased if it were regarded as functioning. Finally, the number of cases was too small to analyze all possible factors. Future studies can adopt a prospective protocol to find more factors that might influence stent duration, and these factors can be examined in patients receiving other types of stents.
Conclusion
The Resonance ureteral stent is safe and effective in relieving malignant ureteral obstructions. Age and preoperative serum creatinine level were independent risk factors for stent failure. Lower GI cancers had longer stent duration than GU cancers. The benefits of Resonance stents can be maximized under careful patient selection.
Footnotes
Acknowledgments
We would like to express our appreciation to Chia-Yen Chen from Harvard School of Public Health for his help in statistical analysis and Joanna Yeh from Sphera International for language supports.
Disclosure Statement
No competing financial interests exist.