
Abstract
Purpose:
To evaluate the impact of maximal urethral length preservation (MULP) technique in comparison with posterior urethral reconstruction and anterior bladder suspension (PRAS) technique on the continence rates (CR), time to achieve continence among patients with prostate cancer (PCa) undergoing robot-assisted laparoscopic prostatectomy (RALP).
Patients and Methods:
We prospectively analyzed the CR, time to achieve continence, pre- and postoperative prostate-specific antigen (PSA) levels, rates of positive margins among three groups of continent men with PCa undergoing RALP from whom consent was obtained. Each group consisted of 30 patients: PRAS was performed in group A, combined MULP and PRAS in group B, and MULP in group C. Continence was measured by patient self-reporting of the number of pads/24 h.
Results:
No differences were detected in the age, preoperative PSA levels, biochemical recurrence, prostate volume, and positive margins for the three groups. Men in groups B and C had marked improvement in CR 1, 3, and 6 months after catheter removal vs group A (50% and 70% vs 10%, 90% and 96.66% vs 23.3% and 100%, 100% vs 53.3%, respectively, P<0.0001). The average and median times to continence were significantly shorter in group B (5.4 and 4 weeks) and C (3.8 and 3 weeks) vs group A (27.4 and 22.5 weeks), P<0.00001. Using Cox regression analysis, only MULP and MULP+PRAS techniques were significantly correlated with continence outcomes 1, 3, and 6 months after catheter removal.
Conclusions:
MULP rather than PRAS confers higher postoperative CR and shorter time to achieve continence among patients with PCa who underwent RALP without increasing risk of positive margin.
Introduction
P
PPI is attributed solely to intrinsic sphincter deficiency in 90% of cases. Five principles can potentially ensure early return of continence, such as minimal damage to the sphincters, maximal urethral length, watertight vesicourethral anastomosis, fascioligamentous support of anastomosis and rhabdosphincter, and minimal bladder descent. It is difficult to achieve all these aforementioned principles. Two types of continence techniques have been used in RRP: (1) Posterior bladder and urethral reconstruction with or without anterior suspension and (2) maximizing the membranous urethral length. Each technique has its pros and cons, with no consistent advantages on CR. Posterior reconstruction (PR) theoretically minimizes bladder descent and supports vesicourethral anastomosis, maintaining the integrity of the rhabdosphincter.
Maximal urethral length preservation (MULP) was first used in RRP 2 –4 and LP 5 and was shown to ensure early return of continence. Its use in RALP, however, has not been reported. In this prospective controlled study, we report our modified technique of MULP by retroapical dissection to preserve urethral length and examine its impact on postoperative continence in men undergoing RALP.
Patients and Methods
After obtaining Institutional Review Board ethical approval, 90 from a total pool of 207 consecutive patients undergoing RALP by a single surgeon with a high volume of procedures for localized PCa at our institution between December 2011 and March 2013 were divided into three groups (30 in each group) and were prospectively studied to examine CR using three techniques (Table 1); 107 patients were excluded from our study based on our exclusion and inclusion criteria.
CT=computed tomography; MRI=magnetic resonance imaging; XRT=radiotherapy; HIV=human immunodeficiency virus.
The inclusion criteria included continent men with a diagnosis of localized PCa who had not undergone previous therapies such as surgery, radiotherapy, hormonal therapy, and cryotherapy and had no comorbidities. The exclusion criteria are shown in Table 1. These men were divided into three main age and prostate-specific antigen (PSA) matched groups: Group A (n=30), in whom posterior urethral reconstruction and anterior suspension (PRAS) was performed; group B (n=30), in whom MULP was performed in combination with PRAS; and group C (n=30), in whom only MULP was performed.
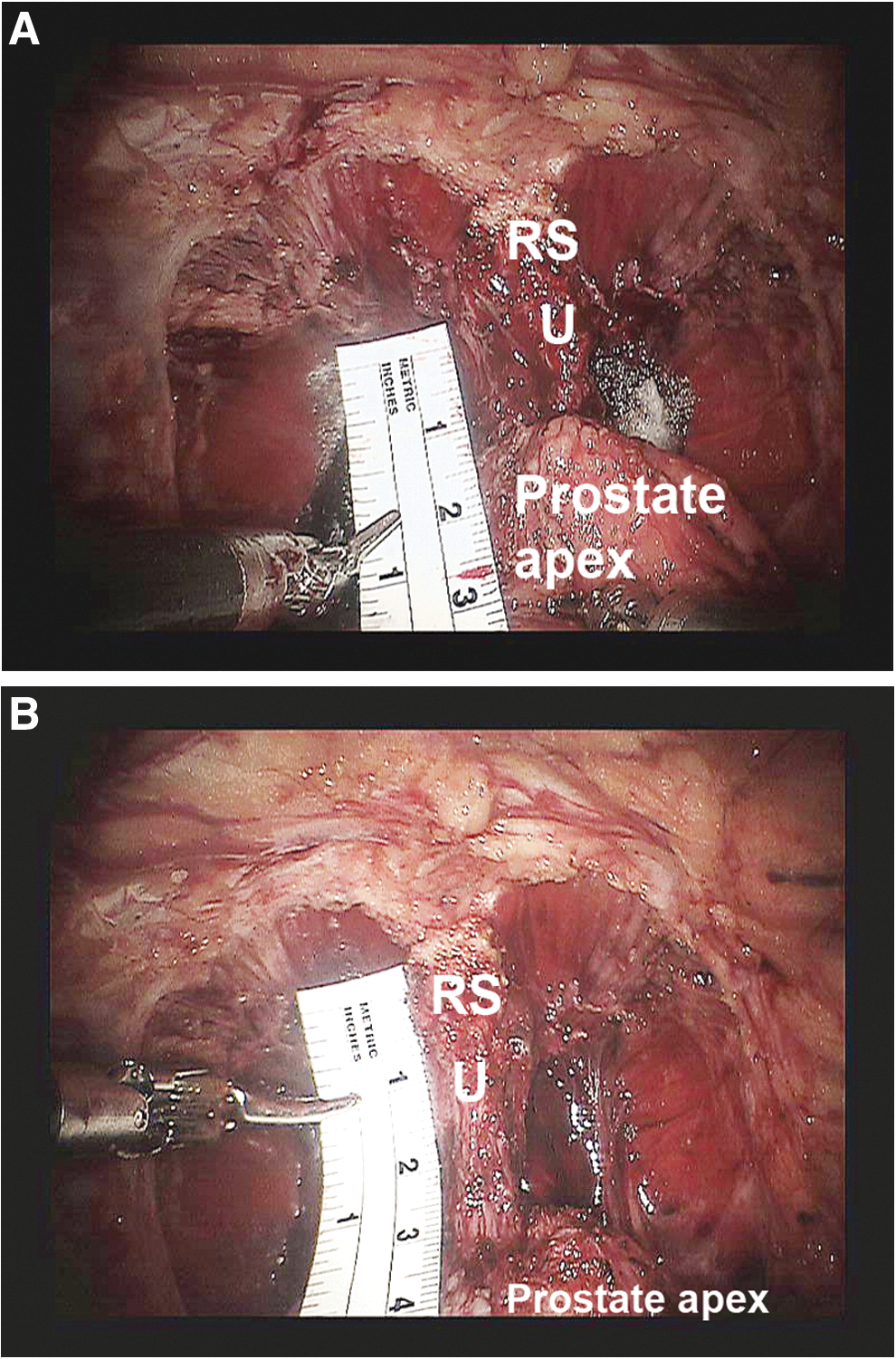
Preoperatively, the assessed parameters included age, PSA level, Gleason score, and continence status (based on ICS-Q30 male questionnaire and no pads use) (Table 2). Intraoperatively, in groups B and C in whom MULP was performed, we measured the extra urethral length (achieved by retroapical dissection) added to the membranous urethra using a graded device (the extra length measured from the proximal edge of the rhabdosphincter to the verumontanum) (Fig. 1B.) Postoperatively, we assessed PSA level (3, 6, and 12 months after Foley catheter removal), prostate volume, rate of overall and apical positive margins, presence of nerve sparing, and continence status—determined by satisfying the two measures: Subjectively by a validated and self-assessed ICS-Q30 male questionnaire, conducted through direct patient interview in the clinic and objectively by reporting the number of pads used, if any, per 24 hours 1, 3, and 6 months after catheter removal. The use of no pad was defined as “continent,” and all other amounts of pad use as having varying degrees of “incontinence.” The definition of continence was based on the two assessment methods.
MULP=maximal urethral length preservation; PRAS=posterior urethral reconstruction and anterior suspension; SEM=standard error of the mean; preop=preoperative; PSA=prostate-specific antigen.
Operative technique
Once the deep venous complex is dissected, the prostatic apex and rhabdosphincter are seen (Fig. 1A). The apex is carefully dissected along the retroapical plane using the robotic endoshear, beginning from the visible prostatic-rhabdosphincter junction, by dividing the striated and the smooth muscle fibers sweeping from the apex toward the membranous urethra. Twisting and rotating the prostate from side to side with the fourth robotic arm enables distinct visualization of the anatomy of the prostatic apex, which in turn prevents inadvertent capsulotomy and a positive margin. Subsequently, division of the flimsy posterior fibrous connections at the apex of the prostate allows the release of the posterior lip of the prostate, thereby exposing an additional length of intraprostatic urethra, which is then preserved and adds to the MULP (Fig. 1B). Completion of this dissection and division of the urethra at the “new” prostatourethral junction results in preservation of a long urethral stump. A standard Van Velthoven vesicourethral anastomosis completes the procedure.
PRAS was performed by suturing the posterior bladder wall and residual Denonvilliers fascia to the rhabdosphincter and median fibrous raphe. Then, after completion of the urethrovesical anastomosis, anterior suspension was accomplished by approximation of the puboprostatic ligaments to the anterior bladder neck.
Statistical analysis
The primary end point is achievement of continence. Based on power of 80%, α=0.05, effect size of 10%, the least sample size needed in each group is 24. Statistical comparison among the three study groups was conducted using the SPSS 12.0 (SPSS Inc., Chicago, IL) by applying the chi-square test and one-way analysis of the variance. Cox regression analysis was used to examine the probable predictive role of different factors such as surgical techniques, age, Gleason score, preoperative PSA level, and neurovascular bundle preservation in anticipation of continence outcomes. Probability value <0.05 was considered statistically significant. Kaplan-Meier survival plot was used to examine the cumulative incidence of continence among the three study groups. Receiver operator characteristics (ROC) curve analyses were used to calculate area under the curve (AUC), critical cutoff value for the extra urethral length, which resulted in early continence at 1, 3, and 6 months after catheter removal.
Results
Postoperative data such as the age, PSA level, Gleason score, and prostate volume among the three groups were assessed. Using chi square, CR at 1, 3, and 6 months after catheter removal in groups B (50%, 90%, and 100%) and C (70%, 96.6%, and 100%) showed significant improvement vs group A (10%, 23.35%, and 53%) (Table 3). There were no significant differences in the 1, 3, and 6 month CR between groups B and C (P=0.11, 0.27, and 1, respectively). Shorter time to achieve continence was reported in groups B (mean and median times were 5.4 weeks and 4 weeks, respectively) and C (mean and median times were 3.8 weeks and 3 weeks, respectively) vs group A (mean and median times were 27.4 weeks and 22.5 weeks, respectively), P<0.05, P<0.05, respectively. Again, no significant differences were seen in the mean time to achieve continence between groups B and C, P=0.883 (Table 3).
PSA=prostate-specific antigen; NVB=neurovascular bundle; MULP=maximal urethral length preservation; PRAS=posterior urethral reconstruction and anterior suspension; postop=postoperative.
The postoperative PSA level <0.2 at 3, 6, and 12 months was comparable in all groups (group A: 93.3%, 90%, 90%), (group B: 93.3%, 93.3%, and 93.3%), and (group C: 100%, 100%, and 96.66%) (P=0.351, P=0.351, P=0.585). The rates of overall and apical positive surgical margins were not significantly different between the groups (group A: 20% and 6.6%; group B: 10% and 10%; group C: 10% and 10%; P=0.487, P=0.894, respectively). The mean values of extra length achieved in MULP and MULP+PRAS were 13.93 and 14.4 mm, respectively (P=0.23).
Using Cox regression analysis, only MULP and MULP+PRAS techniques were significantly associated with continence outcomes at 1 and 3 and 6 months after catheter removal. At 1 month, the odds ratio (OR) for continence by MULP vs PRAS was 9.85, 95% confidence interval (CI) (2.85–34), P=0.0003, and the OR for MULP+PRAS vs PRAS was 6.2, with 95% CI (1.75–22.5), P=0.005 (Table 4). At 3 months, the OR for continence by MULP vs PRAS was 105.6, CI (13.7–813.6), P=0.00001 and for MULP+PRAS vs PRAS was 61.8, 95% CI (8–470), P=0.0001 (Table 5). At 6 months after catheter removal, the OR for continence by MULP vs PRAS was 15.7, CI (6.6–37), P<0.000001 and for MULP+PRAS vs PRAS was 8.97, 95% CI (4–20), P=0.0000001 (Table 6). By using the same regression analysis, no significant predictive effects of age, preoperative PSA level, Gleason scores, prostate volume, and neurovascular bundle preservation on the 1, 3, and 6 month CR were detected (P>0.05).
CI=confidence interval; OR=odds ratio; NVB=neurovascular bundle; PSA=prostate-specific antigen; MULP=maximal urethral length preservation; PRAS=posterior urethral reconstruction and anterior suspension.
CI=confidence interval; OR=odds ratio; NVB=neurovascular bundle; PSA=prostate-specific antigen; MULP=maximal urethral length preservation; PRAS=posterior urethral reconstruction and anterior suspension.
CI=confidence interval; OR=odds ratio; NVB=neurovascular bundle; PSA=prostate-specific antigen; MULP=maximal urethral length preservation; PRAS=posterior urethral reconstruction and anterior suspension.
A Kaplan-Meier plot among the three study groups clearly showed the differences in the CR between MULP and MULP+PRAS groups on one side and PRAS on the other side (Fig. 2).
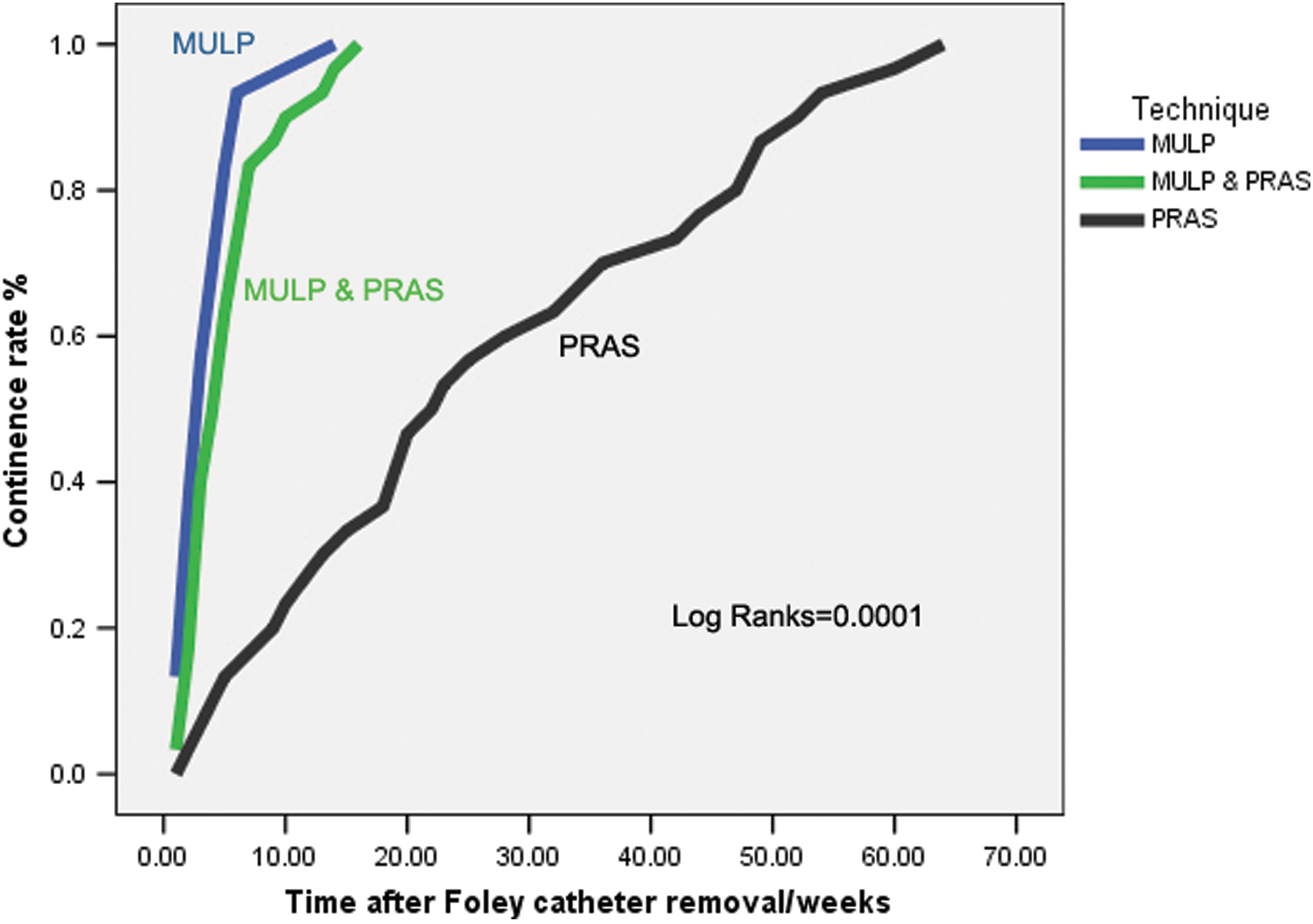
Kaplan-Meier plot for the improvement in continence rates among the three study groups. MULP=maximal urethral length preservation; PRAS=posterior urethral reconstruction and anterior bladder suspension.
Using ROC analysis, critical cutoff extra urethral length achieved by MULP, which led to early return of continence in 1 month, is 13.5 mm with sensitivity of 84.6% and specificity of 82% (AUC=0.84, 95% CI=0.76–0.93, P=0.0002) (Fig. 3). Whereas, for continence at 3 and 6 months, the critical cutoff extra urethral lengths were 10.5 mm with 87.3% sensitivity and 88.9% specificity (AUC=0.89, 95% CI=0.78–0.96, P=0.0002) and 5 mm with 79% sensitivity and 100% specificity (AUC=0.895, 955 CI=0.83–0.95, P=0.00029).

Receiver operator characteristics curve showing area under the curve (AUC), cutoff, sensitivity, specificity of critical extra urethral length predicting early return of continence at 1 month after catheter removal.
Discussion
We evaluated the impact of our modified approach of MULP using retroapical dissection in RALP on return of early continence. We found that preservation of extra urethral length of 13.93 to 14.4 mm (obtained from intraprostatic urethra and added to the membranous urethra) can lead to CR in 50% to 70% of patients at 1 month, in 90% to 96.66% at 3 months, and in 100% of patients 6 months after catheter removal.
Several anatomic, functional, and radiologic reports indicated that a considerable proportion of the male external urethral sphincter (EUSC) is located between the verumontanum and the distal edge of the prostate apex, and this part plays a substantial role in continence. 6 –8 We were able to measure and preserve this extra length of intraprostatic urethra and EUSC, which added to the membranous urethral length, thereby contributing to the overall continence mechanism.
MULP can lead to successful achievement of the all surgical principles necessary to attain continence. It minimizes surgical damage to the two components of the rhabdosphincter (i.e., the smooth and the striated muscular portions and their nearby nerves). The long urethral stump facilitates faster and easily accessible vesicourethral anastomosis and provides support to the bladder, minimizing the bladder descent.
The 1, 3, and 6 month CR after catheter removal among our patients who underwent RALP and MULP with or without PRAS were higher than other series that examined the post-RALP functional outcomes using 0-pad or 0–1 pad definitions of continence. 9 Alternatively, Menon and associates 10 reported a higher 1-month CR (75%–80%) in their controlled randomized study using the 0-1 pad definition than what our results showed.
What was especially interesting regarding this technique was not only that higher proportions of our patients became dry but also there was a shorter period to attain the dry state (the mean and median times for continence return for MULP were 3.8 and 3 weeks, respectively; the mean and median times for MULP+PRAS were 5.4 and 4 weeks, respectively). As such, our patients were able to return to their daily life activities with minimal morbidity. Our mean and median times to achieve early continence were shorter than what was reported by Tewari and colleagues 11 (median time: 44 days), Kim and coworkers 12 (median time: 3.7 months), and Woo and colleagues 13 (mean time: 90 days).
No previous series on RALP has striven for surgical preservation of the urethral part that is covered by the prostatic apex nor examined the significance of this part in continence return. Meanwhile, several reports on RALP have recognized the importance of each millimeter of membranous urethral length in postoperative continence. In our study, we found that adding extra urethral length of at least 13.5 mm can predict early return of continence at 1 month after catheter removal with sensitivity of 84% and specificity of 82%, whereas, extra urethral lengths of 10.5 mm and 5 mm can predict return of continence at 3 and 6 months, respectively.
Our results agreed with previous studies on radical prostatectomies that examined the role of maximal urethral length in promoting continence. Van Randenborgh and associates 2 reported that careful open preservation of the long membranous urethral stump, including the 1 cm from the distal intraprostatic part, can lead to significant return of continence in 88.84% of all patients compared with 76.02% without preservation of the long stump. Furthermore, they reported an even shorter time to achieve continence (one-third were continent in 4 weeks vs 15%). 2 Similarly, Schlomm and colleagues 14 reported that using careful open apical dissection respecting the individual length of the intraprostatic part of the urethral sphincter with fixation of the rhabdosphincter can lead to continence in 50% and 96.9% of patients after 1 week and 12 months of Foley catheter removal vs 30.9% and 94.7% of patients in whom apical dissection was not performed. The authors did not mention, however, the mean of the extra length added to the membranous urethra.
Hakimi and coworkers 15 using RALP did not find a significant association between the urethral length (intraoperatively measured stretched [mean 2.17 cm] and cut [2.20 cm], as well as preoperatively measured urethral length by endorectal MRI [1.46 cm]) and the CR (measured up to 15 months after surgery) (P=0.07, P=0.40, P=0.41, respectively). Hakimi and coworkers 15 did show, however, that the stretched and cut urethral length is associated with a shorter period to pad-free status (mean time: 5.2 months) (P=0.03, P=0.04, respectively). Mizutani and colleagues 5 noted a significant relationship between MULP (2.2±0.3 cm) performed during LP, measured by transrectal ultrasonography and CR 1, 3, and 6 months after catheter removal (P<0.05). 5
Nguyen and associates 3 and Paparel and coworkers 4 used preoperative and postoperative MRI to measure the membranous urethral length in men undergoing RALP and open radical prostatectomy, respectively. Nguyen and associates 3 reported that postoperative 14-mm length is correlated with higher continence rates (90%) at 6 months compared with men with shorter stumps (47%), whereas Paparel and coworkers 4 found that preoperative length of 14 mm and postoperative length of 13 mm are significantly associated with higher continence rates. Other studies have also pointed out the importance of membranous urethral length for achievement of continence. 5,16 Alternatively, Borin and colleagues, 17 using RALP, did not find significant association between the urethral length (measured intraoperatively) and CR. Borin and colleagues 17 preserved only 3 to 6 mm of UL, however, proximal to the prostatourethral junction.
In our study, we found that longer extra urethral lengths of 13.5 mm and 10.5 mm were associated with shorter time to continence at 1 and 3 months after catheter removal, respectively. Only 5 mm of extra urethral length, however, may be sufficient to achieve pad-free status at 6 months. Such findings may highlight the role of healing in the surgical field, which minimizes excessive bladder descent, and complete functional recovery of rhabdosphincter, which probably was transiently damaged by thermal and or mechanical factors.
The most challenging anatomic factor in our technique is the apical prostate shape. We noticed a posteriorly extending apical lip in most of our patients that necessitated meticulous retroapical dissection along the side walls of the urethra to avoid having positive apical margins. Furthermore, the level of urethral transection was made distal to the verumontanum. More recently, with further refinement of our MULP technique, we were able to add an extra length of as much as 2 cm to the membranous urethra.
The main theoretical and potentially inherent risk of our procedure is an increase in the chances of positive apical or urethral margins because MULP might breach the PCa zone during retroapical dissection. Therefore, we routinely performed transitional zone biopsy on our patients, and men with PCa involving the apex and transitional zones were excluded from the study. Such a practice might help us minimize but not theoretically eliminate the possibility of cutting into the cancer.
For the selected patients, no significant differences were noticed in the rates of overall and apical positive margins in men undergoing MULP vs men who did not. Again, after a 12-month follow-up period, no significant variations were detected in terms of biochemical recurrence in groups B and C vs group A. Our results are concordant with other reports that preserved extra length to the membranous urethra and did not recognize an increase in the rates of overall and apical positive margins. 2,5,14,15
In the PRAS group, six (20%) patients had overall positive and two (6.6%) had positive apical margins. In MULP+PRAS and MULP groups, three (10%) patients in each had positive apical margins. We usually observe PSA dynamics for these persons and reserve radiation for those who demonstrate biochemical recurrence. In the PRAS group, three patients had biochemical recurrence, and only one of them had a positive posterolateral margin. Two of them received combined hormonal and radiation therapy whereas the third one received radiation therapy. The three patients couldn't attain pad free status after 6 months of postoperative follow-up. In the MULP+PRAS group, three patients had positive apical margin and only one of them had biochemical recurrence and received radiation therapy and antiandrogen therapy. This single patient was continent at 1 month after Foley catheter removal and maintained his continence despite radiation therapy. In the MULP group, none of three patients with positive apical margins had biochemical recurrence, and their PSA dynamics were observed.
What is more, no discernible advantages were seen with the PRAS technique. Our results are in agreement with the recent systematic review by Rocco and coworkers 18 that could not recognize any efficacy on postoperative CR.
PRAS was initially used in retropubic radical prostatectomy such as the Pagano suture 19 and the Rocco technique 20 with no long-term studies showing any distinct advantages. Moinzadeh and colleagues 19 reported in an uncontrolled retrospective study that posterior bladder neck plication performed during RRP resulted in early return of continence (within 3 weeks) in 63.5% of patients and late return (within 15 months) in 99.55% of patients. Rocco and associates 20 sutured the posterior semicircumference of the external sphincter to the Denonvilliers fascia and fixed it to the posterior bladder wall 1 to 2 cm cranial and dorsal to the new bladder neck. The authors compared the study group, which included 161 patients, to historical groups consisting of 50 patients who underwent RRP without the anterior suspension procedure. Rocco and associates 20 reported early return of continence in 72%, 78.8%, and 86.3% of patients at 3, 30, and 90 days, respectively, after the procedure.
Subsequently, PR with or without anterior suspension was used in RALP in the last 4 years, and 11 published articles have examined its role in early return of post-prostatectomy continence. While six controlled studies were in favor of this technique in terms of shorter time to continence and significant proportions of continent men, 21 –26 five studies, including a randomized controlled study, reported no role of PR in continence. 10,13,27 –29 Two recent systematic reviews showed no or only a slight benefit of PR in postoperative continence. 18,30
In our study, we found that PRAS combined with MULP led to insignificant worsening of CR compared with MULP alone. There may be a detrimental effect of PRAS on the continence mechanism. This technique might help minimize bladder descent ensuring adequate transmission of the increased intra-abdominal pressure during coughing or sneezing to the bladder neck area but not to the midurethra, resulting in higher intravesical pressure than midurethral pressure and stress incontinence.
Furthermore, we retrospectively noticed dramatic improvement in the frequency and time to achieve continence in men undergoing MULP vs no intervention (unpublished data). Such findings, combined with the results of our study, strongly demonstrate the role of MULP in post-RALP continence.
Interestingly, in contrast to other reports, 16 our results did not find any significant role of patient age, Gleason score, preoperative PSA level, prostate volume, or neurovascular bundle preservation in prediction of the CR at 1, 3, and 6 months after catheter removal. We believe that MULP can mitigate the effect of age on postoperative continence because our study's older patients (>65 years) attained early continence.
The implication of our technique is to redefine the proximal level of the membranous urethra and suggest the verumontanum rather than the prostate apex as an important defining anatomic landmark. This definition coincides with the cystoscopic view of urethral parts and anatomic reports that showed that a significant proportion of the EUSC is located in the urethral wall extending between the verumontanum and lower edge of the prostatic apex.
The technical advantages of RALP are minimal surgical trauma, relatively bloodless field, manual surgeon dexterity to dissect tissues along surgical planes that are inaccessible by open or even conventional laparoscopic means, and enhanced CR. These advantages facilitate augmentation of the membranous urethra by an extra length of urethra that is hidden by the prostate apex, which in turn appears to be the most powerful predictor of CR after RALP.
Conclusions
Our modified technique of maximal urethral length preservation achieved through meticulous prostatic apical dissection leads to significantly higher CR and a shorter period to pad-free status in men undergoing RALP. This technique is effective and safe because there was no increased risk of positive apical or overall margins. In addition, no discernible advantages on continence were seen when performing PRAS.
Footnotes
Disclosure Statement
No competing financial interests exist.