
Abstract
Aim:
To determine optimum duration of intraurethral 2% lidocaine jelly for pain relief during outpatient rigid cystoscopy.
Materials and Methods:
This prospective randomized study was conducted between June 2012 and November 2013. Four hundred consecutive adult males requiring diagnostic rigid cystoscopy were randomized into four groups depending on intraurethral 2% lidocaine jelly dwell time before rigid cystoscopy: jelly was instilled 5, 10, 15, and 20 minutes before start of the procedure in group A, B, C, and D patients, respectively. The patients' age, patient-reported preoperative anxiety score, patient-reported intraoperative pain score, the surgeon-reported patient's pain score, and the duration of rigid cystoscopy were recorded and analyzed.
Results:
The mean age, patient-reported preoperative anxiety score, and duration of rigid cystoscopy were similar between the four groups with no significant difference noted between them. The least and highest mean patient-reported and surgeon-reported intraoperative pain scores were reported in group C (1.49±0.82 and 1.58±0.67) patients and group A (4.86±1.24 and 4.04±1.11) patients, respectively, while no significant difference was found in these scores between group C and D patients.
Conclusion:
For male patients undergoing diagnostic rigid cystoscopy, an intraurethral dwell time of 15 minutes (of 20 mL 2% lidocaine jelly) provided optimum pain relief.
Introduction
E
Materials and Methods
The study protocol and all procedures were approved by the institutional ethics committee. Between June 2012 and November 2013, consecutive patients attending the urology outpatient department, who satisfied eligibility criteria (inclusion/exclusion criteria) were enrolled in this prospective randomized study. Inclusion criteria were (a) adult male ≥18 years of age, (b) requiring diagnostic rigid cystoscopy. Patients with (a) active urinary tract infection, (b) known case of stricture urethra or history of urethral surgery, (c) cystoscopy for purpose other than diagnosis, (d) neurological disease, and (e) patients who did not provide written informed consent, were excluded from the study. Initial evaluation included a detailed clinical history, physical examination, urinalysis, and ultrasonography at the least. Eligible patients were randomized into one of the four groups (group A, B, C, D). Randomization was done using computer generated randomization tables of equal numbers.
Surgical procedure
One of the resident urologist described rigid cystoscopy procedure in detail to the patient and then gave a self-report 10-point scale (Fig. 1) to the patient to assess the preoperative anxiety level. In all patients, before start of the procedure, 20 mL 2% lidocaine jelly at room temperature was instilled into the urethra over a period of 10 seconds by one of the resident urologists. The jelly was instilled 5, 10, 15, and 20 minutes before start of the procedure in group A, B, C, and D patients, respectively. A penile clamp was placed for the allocated period, during which time the patient lay supine. Rigid cystoscopy was performed by one of the three consultant urologists in the department. All three surgeons performed nearly equal number of cases and were blinded to the patient group. A 17F rigid cystoscope, 30° lens, and 0.9% saline irrigation were used for cystoscopy. Patients, in whom, urethral stricture was diagnosed during the procedure or any form of additional procedure (urethral dilatation, meatoplasty, etc.) was performed, were excluded from the subsequent analysis.

Preprocedure self-report anxiety scale.
After the cystoscopy, a self-report 10-point visual analogue pain scale (VAS) (Fig. 2) was given to the patient to mark their pain score during the procedure. The surgeon performing the rigid cystoscopy, unaware of the patient group, recorded his perception of patient's pain during the procedure on a similar 10-point VAS (Fig. 2).
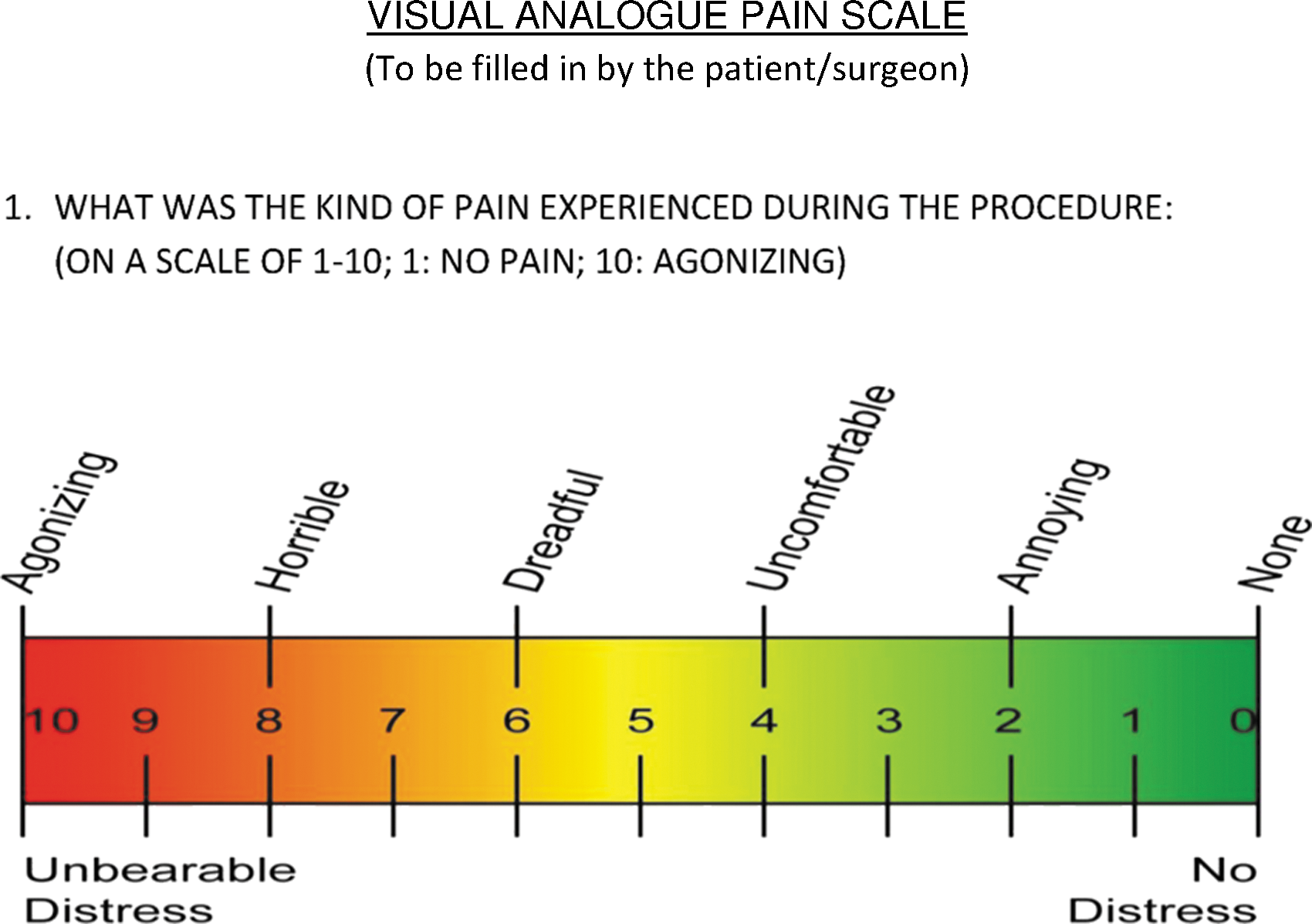
Visual analogue pain scale.
The parameters recorded were age, patient-reported preoperative anxiety score, patient-reported intraoperative pain score, the surgeon-reported patient's pain score, and the duration of rigid cystoscopy (the duration for which the cystoscope was inside the urethra).
Primary outcome measures for group analysis included the following: a. Patient-reported preoperative anxiety score. b. Patient-reported intraoperative pain score.
Secondary outcome measures for group analysis included the following: a. Surgeon-reported intraoperative pain score.
Statistical analysis
Observations were recorded and arranged on a Microsoft Excel spreadsheet (Microsoft, Seattle, WA) and analyzed by SPSS Version 12.0 (SPSS, Inc., Chicago, IL) software package. The calculated sample size was 300 patients (75 per arm) with a power of 80%. The parametric outcomes are expressed as the mean±SD of the group. The one-way ANOVA test was used as a statistical tool to see the significance level between the four groups, whereas the two-tailed Student's t-test was used to see the significance level between the two groups. p-Values <0.05 were considered statistically significant.
Results
Of 480 consecutive male patients who were planned for rigid cystoscopy, 400 satisfied the eligibility criteria and were randomized into 4 equal groups. Of 100 patients in each group, 11, 13, 15, and 15 patients in group A, B, C, and D were subsequently excluded leaving 89, 87, 85, and 85 patients in group A, B, C, and D, respectively, for analysis. Figure 3 summarizes the allocation and dispersion of the patients.
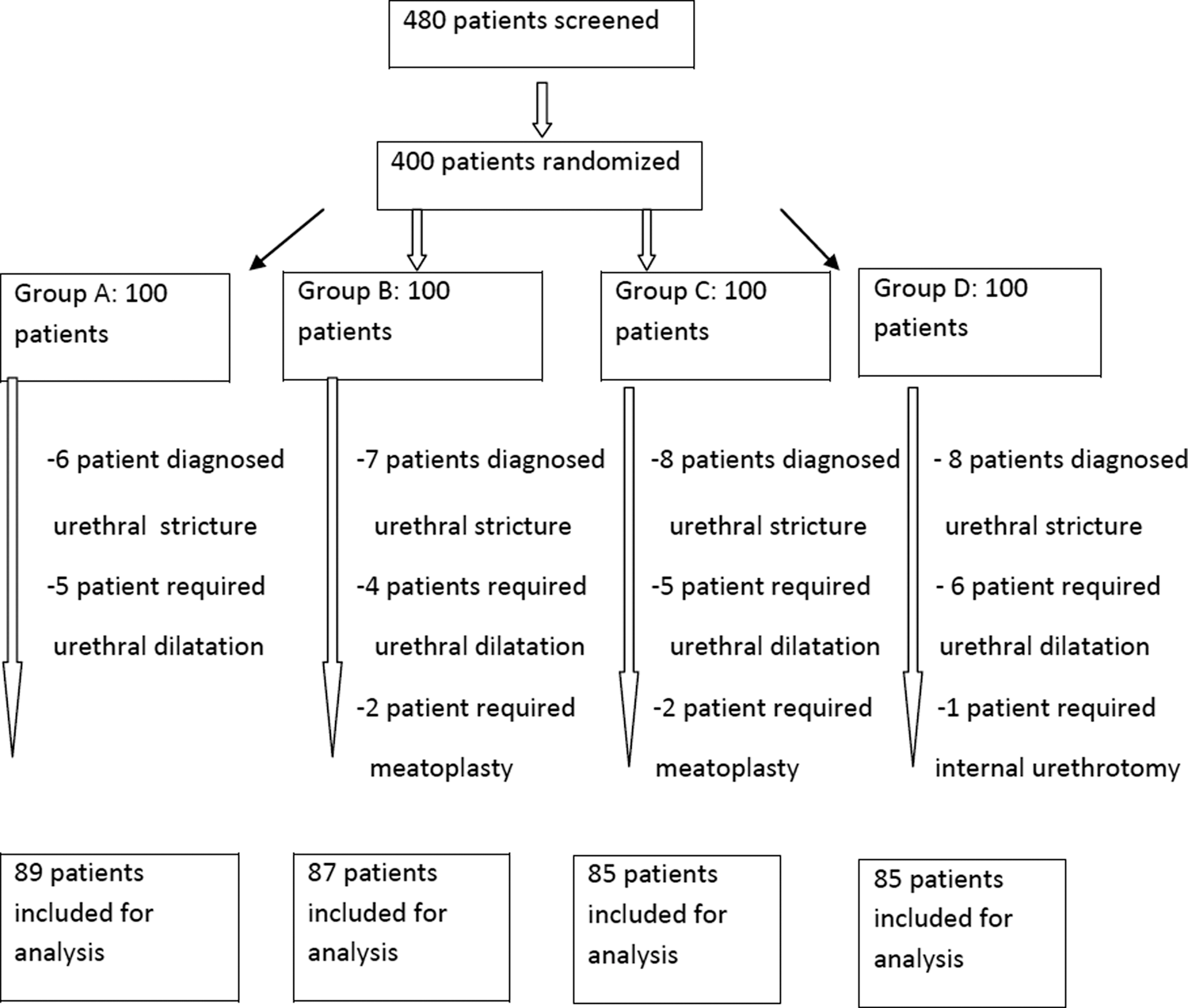
Allocation and dispersion of patients.
Table 1 summarizes the results of the study. The mean age, patient-reported preoperative anxiety score, and duration of rigid cystoscopy were similar between the four groups with no significant difference noted between them. The least mean patient-reported and surgeon-reported intraoperative pain scores were reported in group C patients, while the maximum mean patient-reported and surgeon-reported intraoperative pain scores were reported in group A patients. There was no significant difference in the mean patient-reported and surgeon-reported intraoperative pain scores between group C and D patients; however, the difference was significant between group A and B, group A and C, group A and D, group B and C, and group B and D (Table 1). The individual urologist's responses were consistent across all treatment groups.
Jelly was instilled 5, 10, 15, and 20 minutes before start of the procedure in Group A, B, C, and D patients, respectively.
One-way ANOVA test.
Student's t-test.
pAB=p-value between group A and B; pAC=p-value between group A and C; pAD=p-value between group A and D; pBC=p-value between group B and C; pBD=p-value between group B and D; pCD=p-value between group C and D; VAS=visual analogue pain scale.
Discussion
Lidocaine jelly (2%), a local anesthetic, is effective in reducing pain during male diagnostic rigid cystoscopy 1 –3 Local anesthetics, by direct interaction with voltage-gated Na+ channels, reversibly block conduction by decreasing or preventing the large transient increase in the permeability of excitable membranes to Na+. 8
With regard to cystoscopy, the extent of pain relief afforded by intraurethral lidocaine jelly (2%) instillation is affected by (a) the volume of jelly used, (b) speed of jelly instillation, and (c) intraurethral jelly dwell time before start of the procedure.
For the purpose of this study, 20 mL volume of jelly was used since various authors have reported this volume as optimum. 1,5,9 Slow instillation was chosen for this study as it has been reported that a slow rate of jelly instillation is associated with less pain. 6 In our study, patients in group A (5 minutes intraurethral dwell time) and B (10 minutes intraurethral dwell time) experienced significantly more pain as compared to patients in group C (15 minutes intraurethral dwell time) and D (20 minutes intraurethral dwell time). However, the pain scores were similar in patients of group C and D (p=0.85). Hence, 15 minutes dwell time seems optimum with no more benefit obtained by waiting longer.
Other authors who have looked at the intraurethral dwell time have reported similar results. Goldfischer et al. in a prospective, randomized, double-blind study suggested that intraurethral 2% lidocaine jelly dwell time of 20 minutes significantly decreased pain perception in men during rigid cystoscopy. 1 Tzortzis et al. in review of literature observed that intraurethral anesthetic jelly dwell time of 10–20 minutes is optimum for pain relief in men undergoing rigid cystoscopy. 10
Literature review on the effectiveness of local anesthetic jelly for pain relief during male flexible cystoscopy shows conflicting results. Patel et al., in their meta-analysis, reported on 817 patients from nine eligible trials. 11 They found no evidence to suggest a statistically significant difference in the efficacy of pain control between lidocaine gel and plain gel lubrication in men during flexible cystoscopy. Aaronson et al. did another meta-analysis, which included two double-blind and two single-blind studies, involving a total of 411 patients. 12 They reported that subjects who received anesthetic-impregnated gel were 1.7 times more likely not to experience moderate to severe pain than subjects who did not have intraurethral instillation of gel.
One limitation of this study is that it included even those patients who had previously undergone cystoscopy under local anesthesia. It may be possible that patients undergoing repeated cystoscopies report a pain score that may be biased depending on previous experiences.
Conclusion
In this study of male patients undergoing diagnostic rigid cystoscopy, an intraurethral dwell time of 15 minutes (of 20 mL 2% lidocaine jelly) provided optimum pain relief. Shorter intraurethral dwell times were associated with significantly more pain, whereas a longer intraurethral dwell time did not give any additional benefits.
Disclosure Statement
No competing financial interests exist.