
Abstract
Purpose:
We assessed our experience performing retrograde ureteroscopy (URS) in patients with a continent urinary diversion.
Methods:
A retrospective review was performed of patients with a continent urinary diversion necessitating URS for diagnostic or therapeutic purposes from 2002 to 2013.
Results:
We identified 11 male and 1 female patients with a continent urinary diversion with a mean age of 62.5 years (27–77) who underwent 13 procedures on 17 renal units. Indication for URS was diagnostic in 10 (77%), stone disease in 2 (15%), and stricture in 1 (8%). URS was attempted a median of 6.2 years (1.3–14.5) after diversion creation. Retrograde URS was attempted in 17 renal units with 10 (59%) accessed successfully. One procedure was staged with antegrade wire access obtained before retrograde URS. Inability to identify the afferent limb or ureteral orifice one (20%), tortuosity of afferent limb two (40%), angulation one (20%), and length of the afferent limb one (20%) were causes for unsuccessful retrograde URS. Of the successfully attempted retrograde URS, 75% occurred within the past 5 years. There were no complications in the successful retrograde URS group. Ureteral stents or nephrostomy tubes were left in place postprocedure in six (50%) patients.
Conclusion:
While technically challenging, retrograde URS can be performed successfully in patients with an orthotopic neobladder once the learning curve for the procedure is overcome.
Introduction
T
The location of the orthotopic neobladder allows for easy access into the diversion by means of the urethra, but once inside, the anatomic landmarks used in endoscopy to locate the ureteral orifices (UO) are lost, making retrograde access and subsequent retrograde ureteroscopy (URS) extremely challenging. Retrograde URS in continent diversions without urethral access has been reported and performed during other percutaneous endoscopic procedures. 4 The challenges of retrograde ureteral access in an orthotopic continent urinary diversion, however, have made antegrade access and staged techniques the common initial treatment of upper tract abnormalities in this patient population. Antegrade access to the upper tract, although minimally invasive, does carry with it risk of hemorrhage, sepsis, and injury to nearby organs. 5 Furthermore, most patients undergoing percutaneous renal access are observed overnight in the hospital, and thus their procedure cannot be performed on an outpatient basis.
Previous small series data would suggest that retrograde access and URS ureteroscopy are feasible with relatively high success rates ranging from 77% to 90%. 2,6 We sought to review our experience and describe the technique for retrograde access in patients with continent urinary diversion.
Methods
After Institutional Review Board approval, a retrospective review was performed of patients with a continent urinary diversion necessitating URS for diagnostic or therapeutic purposes from 2002 to 2013. Procedures were performed by multiple surgeons. While the technique has evolved over time, with initial attempts not using an access sheath, we describe the most common technique to gain successful retrograde ureteral access. The decision to attempt retrograde access vs staged procedure or antegrade access was surgeon dependent. Operative reports from the urinary diversion surgery were reviewed before intervention. Ileal neobladder diversion at our institution is performed in a previously described manner, 7 and ureteroileal anastomosis is performed in an end-to-side fashion previously described by Bricker. 8 Patients are counseled preoperatively regarding the risk of failure of retrograde access necessitating an anterograde (percutaneous) procedure.
Technique
Preoperatively, all patients provide a urine culture and receive 1 week of culture specific antibiotics before the procedure. Patients are placed in the lithotomy position, and flexible cystoscopy is performed. The afferent limb is identified and a 0.035 in Sensor (Boston Scientific) guidewire is advanced into the afferent limb. The cystoscope is removed, and a 10F dual lumen catheter is advanced over the wire. A loopogram is performed with contrast instilled using a 60 mL syringe under manual pressure at this point to aid in identification of ureteral anastomotic sites because all anastomoses are refluxing. While the amount of contrast used is specific to each patient and the size of the diversion, between 120 and 300 mL is usually instilled. The loopogram also provides information on the length and tortuosity of the afferent limb of the diversion. A second guidewire is advanced through the second lumen and a 12/14F ureteral access sheath is advanced to the end of the afferent limb. Flexible ureteroscopy is performed through the access sheath using pressurized irrigant to locate the ureteral anastomosis. Intravenous indigo carmine is also used, if necessary, to help in identification of the ureteral anastomosis.
Once identified, a Sensor or hydrophilic glidewire is advanced through the ureteroscope under fluoroscopic guidance to the renal pelvis. The ureteroscope and access sheath are removed, and a 6F ureteral catheter is advanced over the wire to exchange the wire to a superstiff wire. The superstiff wire aids in straightening a torturous ureter and afferent limb. The 10F dual lumen catheter is then used to place a safety wire, and the 12/14F access sheath is advanced to the proximal ureter over the superstiff wire. URS is then performed per standard protocol. The distal ureter is evaluated last as the access sheath is slowly withdrawn.
At the conclusion of the procedure, a ureteral stent is placed in situ with the attached suture removed. Because many of the procedures were for suspected UTUC, once pathology is confirmed, the stent is removed cystoscopically in 2 to 4 weeks, depending on the degree of ureteral edema, amount of dilation needed, and mucosal irritation visualized during removal of the ureteral access sheath. Stent diameter in established urinary diversions (>1 year) ranges from 6F to 8F. If there is concern for mucus occlusion, a larger diameter stent can be deployed. A long ureteral stent that can traverse the afferent limb and reside near the bladder neck is necessary to allow for cystoscopic removal in the office setting. Patients undergo renal ultrasonography 4 to 6 weeks postprocedure and, if URS was performed for stone disease, radiography of the kidneys, ureters, and bladder as well.
Results
We identified 11 men and 1 woman with a continent urinary diversion (11 neobladder, 1 Indiana pouch) with a mean age of 62.5 years (27–77 years) who underwent 13 procedures on 17 renal units. Indication for diversion was for malignancy in 11 patients and benign disease in 1 patient. Type of diversion included: Right colonic 1, Indiana pouch 1, and ileal neobladder 10. Indication for URS were diagnostic for abnormal cytology or filling defects noted on urography in 10 (77%), stone disease in 2 (15%), and stricture in 1 (8%). One patient underwent two procedures for multiple ureteral recurrences. URS was attempted a median of 6.2 years (1.3–14.5) after diversion creation. Retrograde URS was attempted in 13 with 10 renal units accessed (59%) successfully. One procedure was staged with antegrade wire access obtained before retrograde URS because of surgeon and patient preference. Inability to identify the afferent limb or ureteral orifice 1(20%), tortuosity of afferent limb 2 (40%), angulation 1 (20%) and length of the afferent limb 1 (20%) (Fig. 1) were causes for unsuccessful retrograde URS. Of the successful retrograde URS, six (75%) occurred within the past 5 years.
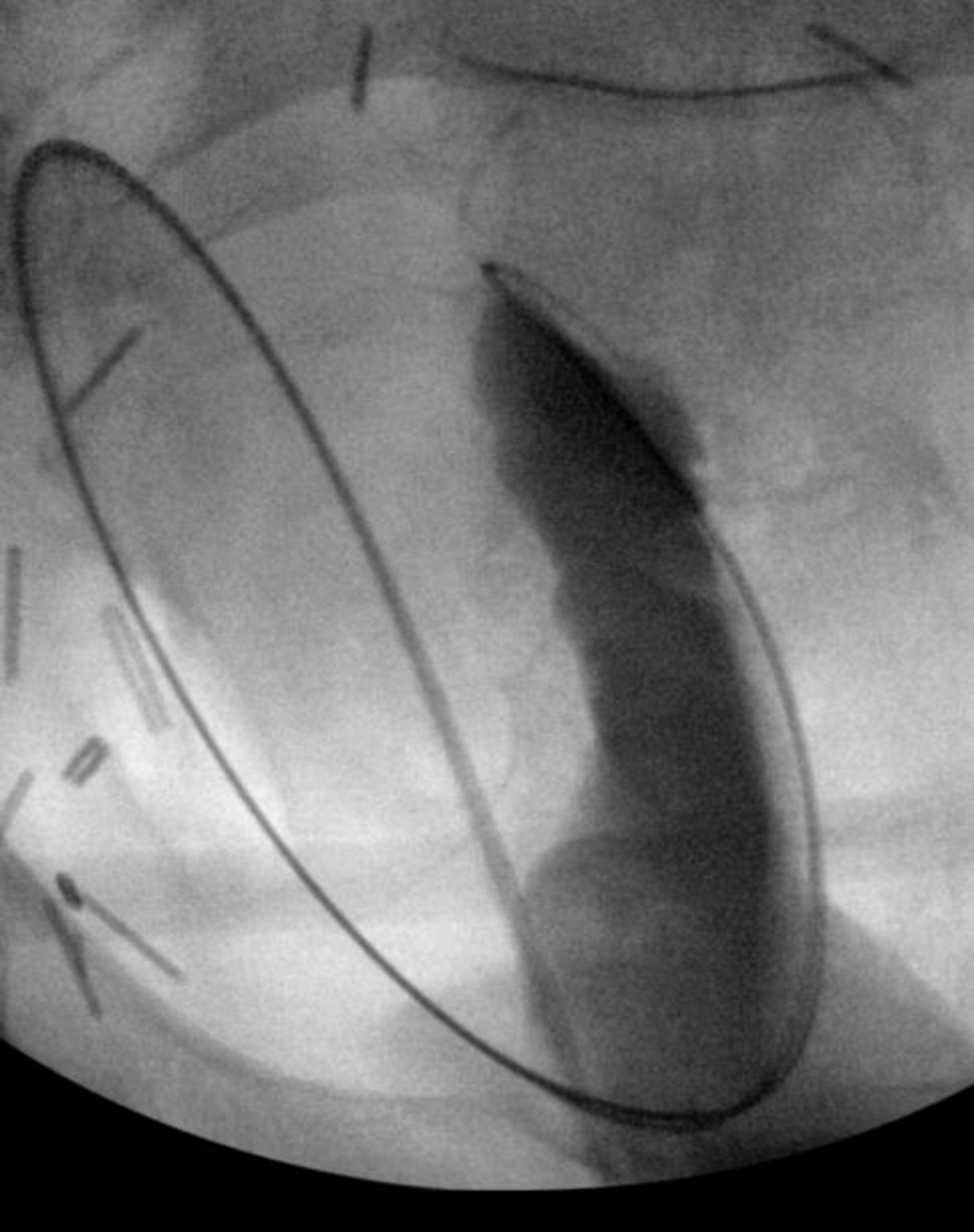
Patient with extremely long afferent limb of the neobladder. Retrograde ureteroscopy was unsuccessful in this case.
In the seven renal units (five patients) in which URS was unsuccessful, antegrade URS was performed in one patient who demonstrated recurrence of urothelial carcinoma. The other patient underwent antegrade brushing of a suspicious lesion. Of the three remaining patients who were unable to have retrograde URS, one underwent a CT-guided biopsy of a suspicious ureteral filling defect, one patient with hematuria chose observation, and one patient with urolithiasis chose observation. There were no complications in the successful retrograde URS group. The patient with the Indiana pouch diversion was treated for both bladder and ureteral stones and thus underwent a percutaneous cystolithotomy with bilateral URS and was admitted for observation. All other patients were dismissed as outpatients. Ureteral stents or nephrostomy tubes were left in place postprocedure in six (50%) patients.
Discussion
Over the past 10 years, we identified 12 patients who underwent 13 attempted retrograde URS procedures on 17 renal units. Of those, 10 were successful. All of the failures were, in part, because of the challenging neobladder anatomy—in particular, the afferent limb of the neobladder. Angulation, tortuosity, and extreme length of the afferent limb were listed in the operative report as reasons for unsuccessful access. Our success rate of 59% is lower than previous published reports. 2,6 This may be, in part, because of the length of time between neobladder formation and attempted URS. In the successful URS group, however, the average time after diversion was 8.4 years (2.3–14.5 years) (Table 1), and in our failure group, it was 5.1 years (1.3–12.5 years) (Table 2). The mean age of patients with URS failures was 60.8 years (49–77 years), and it was 63.5 years (27–75 years) in the successful group.
UPJ=ureteropelvic junction; UTC=upper tract urothelial carcinoma.
UO=ureteral orifice.
While our overall success rate is lower than in previous reports, 75% (six of eight patients) of our successes have occurred within the past 5 years. Nelson and associates 2 list the rate of success with retrograde access in ileal neobladder at 10/13 (77%) renal units. Patients in the series had URS attempted an average of 29 months after diversion. In the description of surgical technique, a directional angled glidewire was used to obtain access to the ureter without an access sheath or safety wire.
Hyams and colleagues 6 described their experience with URS in urinary diversions. The overall success was listed at 75% overall and 90% specifically for neobladder and 33% for Indiana pouch. Indications for URS were stricture disease and UTUC. While a safety wire was used in the described technique, use of an access sheath is not mentioned. There was no mention of how long patients had the diversion before attempted URS. The authors also noted that a lengthy and tortuous ileal conduit limb or anastomotic stricture made achieving ureteral access difficult.
In our described technique, an access sheath is used twice: First to locate and straighten the afferent limb, and second, to access the desired ureter. Ureteral access can be particularly difficult because the ureter typically is implanted at an oblique angle in the afferent limb. While angled wires and ureteral catheters can aid in engaging the ureteral anastomosis, a flexible ureteroscope allows for a much greater range of motion to approach the target. A superstiff wire along with a ureteral catheter is a great aid in straightening and shortening a tortuous ureter. Fluoroscopy is critical to ensure the desired side is being accessed becuse it is not always obvious based on the location of the ureteral anastomosis. Once an access sheath is placed in the ureter, flexible URS with pressurized irrigant can be performed in the usual fashion with excellent visualization.
While retrograde access was attempted for 12 patients in our cohort, some of the unsuccessful URS were in patients who underwent additional antegrade procedures. Currently, antegrade access is more commonly used after urinary diversion than retrograde URS for nonmalignant causes. 9 –11 By accessing the upper tract, all potential problems with the retrograde approach can be avoided; however, there is significant morbidity associated with percutaneous access in patients with urinary diversion with complication rates ranging from 12.5% to 38%. 3,9,12 Of note, 50% (5/10 renal units) of our successful URS cases had negative findings, thus saving those patients the morbidity of a more invasive procedure for a benign workup. In our patients who underwent successful retrograde URS, all were dismissed as outpatients except one, and none of them experienced a complication.
The vast majority of our patients underwent URS for diagnostic purposes. These patients presented with findings of suspicious imaging during follow-up of their primary malignancy, recurrence in the neobladder during surveillance cystoscopy, or positive urine cytology. Picozzi and coworkers 13 performed a meta-analysis evaluating more than 13,000 patients over 40 years with upper urinary tract recurrence after radical cystectomy. After cystectomy, the risk of UTUC ranges between 1% and 6%. Patients with positive ureteral margins had an odds ratio of greater than 7 in cancer recurrence (P<0.0001) and, once with a diagnosis, the prognosis in those patients is poor, with many having evidence of advanced or metastatic disease at presentation with few surviving past 3 years postdiagnosis. 13,14
We recognize certain limitations of this study—namely, that it is a retrospective review subject to selection bias. Our limited number of patients makes it difficult to assess statistical differences between our successful and unsuccessful retrograde group. Our aim, however, was to describe our technique and evaluate our success with URS in continent urinary diversions by a single institution. A multi-institutional prospective study would garner sufficient patient recruitment to allow for further analysis.
Conclusion
While technically challenging, retrograde URS can be performed successfully and safely in patients with a continent urinary diversion once the learning curve for the procedure is overcome. Length and tortuosity of the afferent limb of the neobladder are the most common reasons for retrograde access failure.
Footnotes
Disclosure Statement
Dr. Krambeck is a consultant for the data safety monitoring board of Histosonics; for Dr. Rivera, no competing financial interests exist.