
Abstract
Purpose:
To create a tissue-based simulator that allows practice of key steps of robot-assisted radical prostatectomy (RARP) in a sequential fashion.
Materials and Methods:
A model was created from female porcine genitourinary tract tissue to represent the male pelvic genitourinary anatomy. The following steps of RARP were simulated: dorsal venous complex ligation, division of bladder neck, seminal vesicle dissection, prostatic pedicle ligation with nerve sparing, urethral division, bladder neck reconstruction, and vesicourethral anastomosis. Ten novices and 10 experts performed RARP on the model. Face validity was calculated by ratings of realism. Content validity was calculated by experts' rating of usefulness of the model as a training tool. Construct validity was calculated by comparison of time to complete the simulator and rating of performance on the objective structured assessment of technical skill (OSATS) questionnaire, between novices and experts.
Results:
The model was determined to have good face and content validity with an average score of 3.7/5 and 4.8/5, respectively. The mean time for completion of the simulator was 121.5 minutes for the novice and 62 minutes for the expert group (P<0.001), and the mean overall OSATS performance ratings were 4.6/5 for experts and 2.6/5 for novices (P<0.001), yielding good construct validity.
Conclusions:
We created and validated a realistic, tissue-based simulator to allow for training of key surgical steps of RARP in a sequential fashion. Ultimately, this simulator could be incorporated into urology training, credentialing, and facilitate surgeon transitioning from open prostatectomy to RARP.
Introduction
S
Surgical simulators can be placed into two categories—virtual reality simulators that simulate an operation with animation on a computer monitor and mechanical simulators that actually manipulate real-life objects. Currently, virtual reality surgical simulators can effectively reproduce specific tasks, such as moving a ball into a basket or cauterizing and cutting blood vessels. Examples of such simulators that use a robotic console to allow practicing tasks or following steps of the procedure include the da Vinci Skills Simulator, dV-Trainer, Mimic, and RoSS. 9 –17 While this helps to improve a surgeon's core laparoscopic and robotic skills and familiarize the surgeon with the robotic console, it does not replicate the actual steps of RARP. Mechanical laparoscopic simulators have been developed to replicate the vesicourethral anastomosis during RARP, but not the entire procedure. 18 –24
Our goal was to create and validate a high-fidelity, ex-vivo tissue-based simulator that allows the key steps of RARP to be practiced in a sequential fashion.
Materials and Methods
Development of model
A plaster replica of the human pelvis is fitted with a rubber pad, simulating the urogenital diaphragm. A tissue model of the human male lower genitourinary tract is constructed from female porcine genitourinary tract tissue representing the urethra (which was catheterized), bladder, prostate, prostatic pedicles, seminal vesicles, rectum, dorsal venous complex, and neurovascular bundles (Fig. 1). To create this model, the vagina, bladder, and ureters are harvested from a female pig. The female vaginal orifice is left intact, and the vagina and urethra are transected at a point 5 cm proximal to the introitus and cut in half lengthwise. A 5-cm segment of fallopian tube is cut and secured posteriorly to the introitus at the junction of the vagina with the introitus.

Creation of model. The porcine genitourinary tract tissue used to create the model is depicted before manipulation. The corresponding portions of anatomy that it will come to represent in the simulator are demonstrated.
A posterior cystotomy is made in the native bladder, and the introitus tissue is secured inside the bladder neck, pushing the tissue mass as distally as possible into the bladder neck, creating a bulge that replicates the prostate. The two segments of the cut urethra and vagina are pulled through lateral incisions in the bladder to represent the prostatic pedicles, and the fallopian tubes are pulled through the posterior midline to replicate the seminal vesicles. The ureters are secured to the posterolateral portion of the model prostate with Super Glue® to replicate the neurovascular bundles. The remaining vagina remains attached to the native urethra to represent the rectum, and Super Glue is used to secure the “prostate” onto the vagina. The Super Glue creates realistic tissue adhesions that are seen between prostate and neurovascular bundle as well as between prostate and rectum during RARP. The cost of the raw tissue for each model is approximately $75, with each model needing 30 to 45 minutes to fashion.
This model is then placed into the pelvic mold that has been affixed with a latex urogenital diaphragm. The urethra, dorsal venous complex, and rectum (actually pig vagina) exit the urogenital diaphragm while the bladder and anterior rectum are secured superiorly. The entire model is then secured onto an operating bed with robotic arms directed into the pelvis. The model represents RARP after the ports have been placed and the bladder has been dissected from the anterior abdominal wall. The subjects were then instructed to perform the following steps of a RARP without pauses: (1) Placement of a dorsal venous complex suture; (2) division of the bladder neck; (3) dissection of the seminal vesicles; (4) ligation of the prostate pedicles with identification and preservation of the neurovascular bundles; (5) apical dissection of the prostate and division of the urethra; (6) bladder neck reconstruction; and (7) vesicourethral anastomosis (Fig. 2). A bedside assistant was provided for instrument changes, retraction, and insertion of sutures only as instructed by the surgeon.
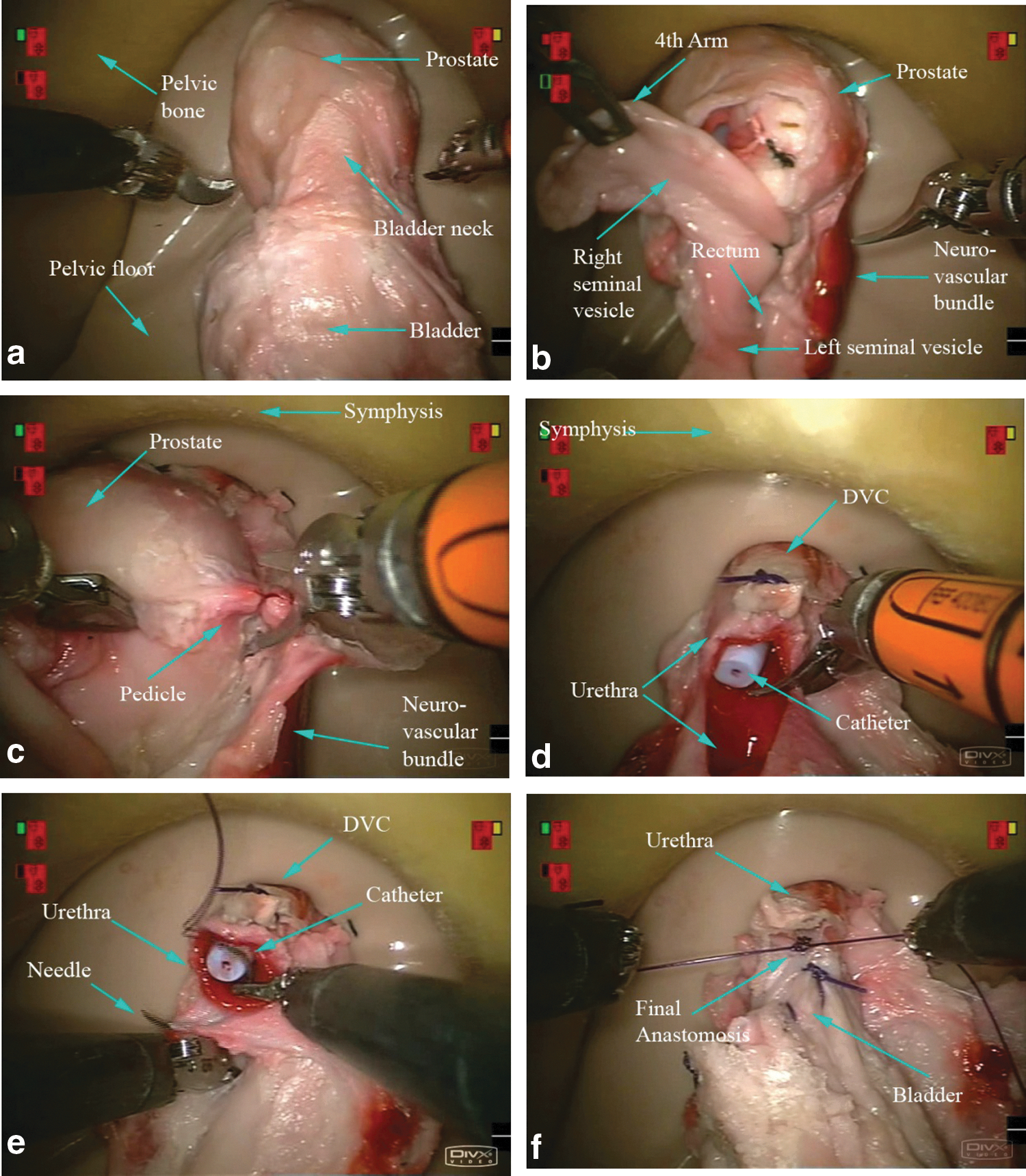
Simulator during robot-assisted radical prostatectomy. Steps illustrated as follows:
Subjects
A total of 20 subjects were evaluated: 10 were considered experts and 10 novices—based on the number of RARP performed as the primary surgeon (>50 RARPs classified as expert, <20 RARPs classified as novice). All novices had experience with the da Vinci console (either from a training module or in the operating room) and were familiar with the steps involved during RARP (either as an assistant, primary surgeon, or video education). Subjects received a standardized introduction to the simulator and the steps of the RARP to be performed in our model.
Validation
Face validity (the measure of the realism of a simulator) and content validity (judgment of the appropriateness of a simulator as a teaching modality) 25 for our RARP simulator were determined by a 10-question survey completed immediately after performance on the simulator. Ratings were scored on a 1–5 Likert scale. Face validity was determined by analysis of survey data from the novice and expert questionnaire regarding realism of the simulator. Content validity was determined by analysis of survey data from the expert group regarding useful of the simulator as a training tool for RARP.
Construct validity (the ability to discriminate between subjects at different levels of experience) was measured both objectively and subjectively. First, time to complete each step and the entire procedure was recorded (including instrument changes) and compared between novices and experts. Second, two expert robotic surgeons, neither of whom were study subjects, and blinded to subject identity and experience, observed video performance of each subject and graded the procedures. Each expert reviewer has performed at least 200 robot-assisted procedures as a primary surgeon. A validated global objective structured assessment of technical skills (OSATS) 26 format was used for grading the procedure while watching video playback of each surgeon. The OSATS scores from the two expert observers were compared to determine interrater reliability. In addition, the quality of final product in regard to the nerve sparing and anastomosis was also assessed on a 1–5 scale based on the residual nerve tissue left behind on completion of the RARP and water-tightness of anastomosis.
For sample size and power computations, we hypothesized that the mean global rating score for the expert will be 4.5 for all of the OSATS categories and the mean OSATS score for novice would be 2.5. Based on the maximum and minimum possible value, standard deviation was expected to be near 1.5. Based on these estimates, we enrolled a total of 20 participants (10 from each group) to differentiate expert from novice, with 80% power at 5% level of significance. To compare novices with experts, we used the Wilcoxon rank sum test. To evaluate agreement among expert video reviewers, we used the Kappa statistic. Bootstrapping was used to simulate 10,000 samples to compute 95% confidence intervals.
Results
Demographics (Table 1)
The novice group was younger than the expert group (mean age 31.8 years vs 39.3 years, respectively, P<0.001), had assisted a similar number of cases as the expert group (median 32.5 vs 50, respectively, P=0.675), but had performed fewer procedures as primary surgeons than the expert group (median 2 vs 255, respectively, P<0.001). Only one person in the novice group was currently in a fellowship, and one had completed a certified module for robotic surgery, while eight of the experts had completed or were currently in a fellowship, and all but one had completed a certified module.
Face and content validity (Table 2)
The overall rating of realism of the simulator by experts and novices was 3.7/5 and 3.8/5, respectively, establishing face validity. The most realistic step was the vesicourethral anastomosis, with ratings of 4.5/5 and 4.6/5 for experts and novices, respectively. The least realistic steps for both experts and novices were seminal vesicle dissection (3.2/5 and 3.2/5, respectively), bladder neck division (3.4/5 for both), and pedicle ligation and neurovascular bundle dissection (3.4/5 and 3.2/5, respectively). Content validity was demonstrated with a rating of 4.7/5 by experts in response to the question regarding usefulness of the simulator as a training tool for RARP.
Face validity.
Content validity.
Questionnaire based on 1–5 likert scale (Not at all, Somewhat, Very)
RARP=robot-assisted radical prostatectomy; DVC=dorsal venous complex.
Construct validity (Table 3)
The mean time for completion of the simulator was 121.4 minutes for the novice and 60.8 minutes for the expert group (P<0.001). Experts completed all of the steps faster than the novices except for seminal vesicle dissection (P=0.97) and division of the urethra (P=0.111) (Table 3).
The overall mean OSATS performance ratings were significantly higher for experts than novices (4.6/5 vs 2.6/5, respectively, P<0.001) (Table 4). Reviewer 1 rated experts better in all of the subcategories, while reviewer 2 did in all but “respect for tissue” (P=0.262), “time and motion” (P=0.052), and “flow of operation” (P=0.058). The raters showed good reliability and agreement with each other (Cronbach α=0.84) (Table 4).
Differences are not statistically significant.
Discussion
Surgical simulation aids in the training of residents and practicing physicians who are honing their surgical skills. While there are many simulators that offer laparoscopic and robotic training for routine skills, there are no realistic simulators for RARP currently available that use real tissue and allow surgeons to progress through the many critical steps of RARP in one setting. It is important for trainees to fully realize the amount and extent of prolonged concentration and skill that are necessary to perform a full RARP. Therefore, we sought to devise a model that was inexpensive, made of readily available tissue, reproducible, and that would allow a trainee to progress through each of the crucial steps of an RARP in a sequential fashion.
Face and content validity of this simulator demonstrated that it is realistic and appropriate in the teaching setting. Construct validity was confirmed for most of the steps of the procedure and for the procedure in its entirety. Placement of the dorsal venous complex suture, bladder neck reconstruction, and vesicourethral anastomosis demonstrated good validity all around. Seminal vesical dissection and division of urethra did not reach significance for construct validity, although they did show face and content validity. While demonstrating good construct validity, division of the bladder neck had fair face validity likely because of the large size of the bladder neck after vesicoprostatic division in our model. Ligation of the pedicles and neurovascular bundle yielded fair face validity, and this may be because of the bloodless dissection in our model and occasional difficulty in cutting through the tissue necessitating assistance from supervisors.
Many surgeons currently begin their RARP experience after observing several cases and attending a 1 to 2 day robotic training course, resulting in the potential for unacceptably long operative times and poor outcomes. 5 As a result, postresidency training for RARP is particularly challenging, and practicing urologists have few options for dedicated training in this procedure. Preceptoring programs have promise, although they are expensive, and necessitate significant time commitment of faculty for design and delivery of the program. 3 Therefore, there is a need for alternative teaching methods, and simulators are able to provide additional training and fill this gap.
Current ex-vivo tissue models for traditional laparoscopic prostatectomy have focused only on the vesicourethral anastomosis, failing to provide simulator training for other key steps in radical prostatectomy. 18,20 Moreover, current virtual reality simulators for robotic surgery, although promising, have evaluated surgical tasks and modules, not actual steps of a procedure such as RARP. 13 As RARP becomes a more commonplace procedure in the academic and community setting, the need for a robust, realistic, and validated simulator to provide training will become paramount. Until affordable lifelike virtual reality simulators are available, it is crucial that surgeons embarking on a complex procedure like RARP be properly trained before sitting at the console in a clinical scenario.
Our model is not without limitations. First, there is a learning curve to the creation of the models, and the quality of the model can be creator-dependent. We did, however, observe the models to be quite consistent over time, which is shown by the reviews from surgical subjects. Second, given that it is a bloodless field with generally consistent tissue planes, the model is probably best used for training novice surgeons and not useful for teaching the nuances of advanced nerve sparing or apical dissection that experienced surgeons will need. Experienced surgeons will continue to need other training tools to learn those techniques, such as expert video review. Third, our model does not allow for training on how to “drop” the bladder off the anterior abdominal wall and therefore also cannot be used to teach a “posterior” approach; only an “anterior” approach with dissection of the seminal vesicles after bladder neck given can be simulated. Fourth, a robotic system needs to be available for use when it is not being used clinically, limiting use to centers with such facilities.
Conclusions
We created and validated a realistic, tissue-based simulator to allow for training of key surgical steps of RARP in a sequential fashion. Ultimately, this simulator could be incorporated into urology residency/fellowship training or facilitate surgeons transitioning from open prostatectomy to RARP.
Footnotes
Acknowledgments
Intuitive Surgical provided an educational grant supporting this project. Endosim helped provide porcine tissue to create the model. They were also not involved in any data analysis.
Disclosure Statement
Endosim is owned by Dr. Kai Matthes. For the remaining authors, no competing financial interests exist.