
Abstract
Purpose:
To evaluate the occlusive properties of latex-covered Amplatzer Vascular Plugs (AVPs) for transrenal ureteral occlusion in vitro.
Materials and Methods:
Latex-covered AVPs type I and II (diameter 8, 10, 12, 14, and 16 mm) were used as occlusive devices. Radial force of an AVP was measured using simulated ureteral diameters of 4 to 12 mm. Occlusive properties were examined in a silicone tube (inner diameter 6 mm) with measurement of drainage time of a 40 cm water column. In complete occlusion, the maximum pressure that the plug was able to withstand was determined at different temperature levels. Statistical analysis of drainage time was performed in a general linear model (GLM) and using correlation analyses. Explanted porcine ureters were used to simulate physiologic conditions. Pressure measurements were performed until leakage, plug dislocation, or rupture of the ureter occurred.
Results:
Radial force depended on AVP type, size, ureteral diameter, and temperature. The 16-mm AVP II showed the highest radial force of more than 5 N (ureteral diameter 4 mm, body temperature). All AVP I showed water leakage and plug dislocation. Drainage time of the AVP II depended significantly on plug size and temperature and correlated with radial force (r=0.731, P<0.001). In complete occlusion, water leakage occurred at 500 to 1000 cm H2O and dislocation between 500 to more than 2000 cm H2O. In porcine ureters, leakage occurred at room temperature between 19 to 93 cm H2O. At body temperature, all AVP II occluded the ureter completely.
Conclusion:
Latex-covered AVP II (diameter 8–16 mm) can effectively occlude the ureter, especially considering remodeling of the nitinol at body temperature. Large plug diameters can exert enough radial force even in dilated ureters to allow for successful occlusion. Because deployment of a 16-mm latex-covered AVP II can be technically difficult, we advocate the use of 12- or 14-mm AVP II for transrenal ureteral occlusion. AVP Is are not suitable for ureteral occlusion.
Introduction
I
To date, several different methods to achieve ureteral obstruction interventionally have been proposed. Drawbacks of many of these techniques are material dislocation necessitating reinterventions, large access sites, or technically challenging methodology. 3
A new method proposed by Schild and associates 4 is the use of a latex-covered Amplatzer Vascular Plug (AVP) type II, which is placed into the ureter via a preexisting nephrostomy to achieve occlusion. Pieper and colleagues 2 recently reported encouraging results of long-term occlusion using this technique without any AVP dislocations. Little is known, however, about the occlusive properties of latex-covered AVPs of different sizes under varying pressure conditions. Because of hypothetical concerns of possible dislocation of a latex-covered plug, other authors alternatively proposed using a bare AVP in combination with cyanoacrylate 5 or even multiple AVPs. 6
The purpose of this study was, therefore, to evaluate the occlusive properties of latex-covered AVPs in a series of in vitro experiments to find the ideal AVP type, size, and delivery protocol to achieve complete ureteral occlusion.
Materials and Methods
Occlusion device
As described by Schild and coworkers, 4 a modified AVP (St. Jude Medical, Plymouth, MA) was used to achieve occlusion. The AVP was covered by a 4-cm long sterile latex finger stall. The cover was knotted tight at the proximal end of the plug using nonabsorbable surgical suture material. AVPs type I and II were used with a diameter of 8, 10, 12, 14, and 16 mm.
Experimental setup
1. Study of radial force of AVPs I and II
2. Study of drainage time after occluding a silicone tube
3. Study of occlusive properties and delivery protocol in explanted porcine ureters
1. Measurements of radial force
To compare the radial force that different AVPs exert on the ureteral wall at varying diameters and temperatures, a set of semicanals milled into aluminium blocks was used (Fig. 1). The blocks were placed together to form a canal (simulated ureteral diameter 4–12 mm) in which the extended AVP was subsequently placed. Weights were then used to approximate radial pressure (N) on the canal by AVPs I and II, both at room temperature, as well as at body temperature. Measurements were repeated five times. Data were evaluated using a general linear model (GLM) to assess interrelations between radial force, AVP type, size, canal diameter, and temperature.
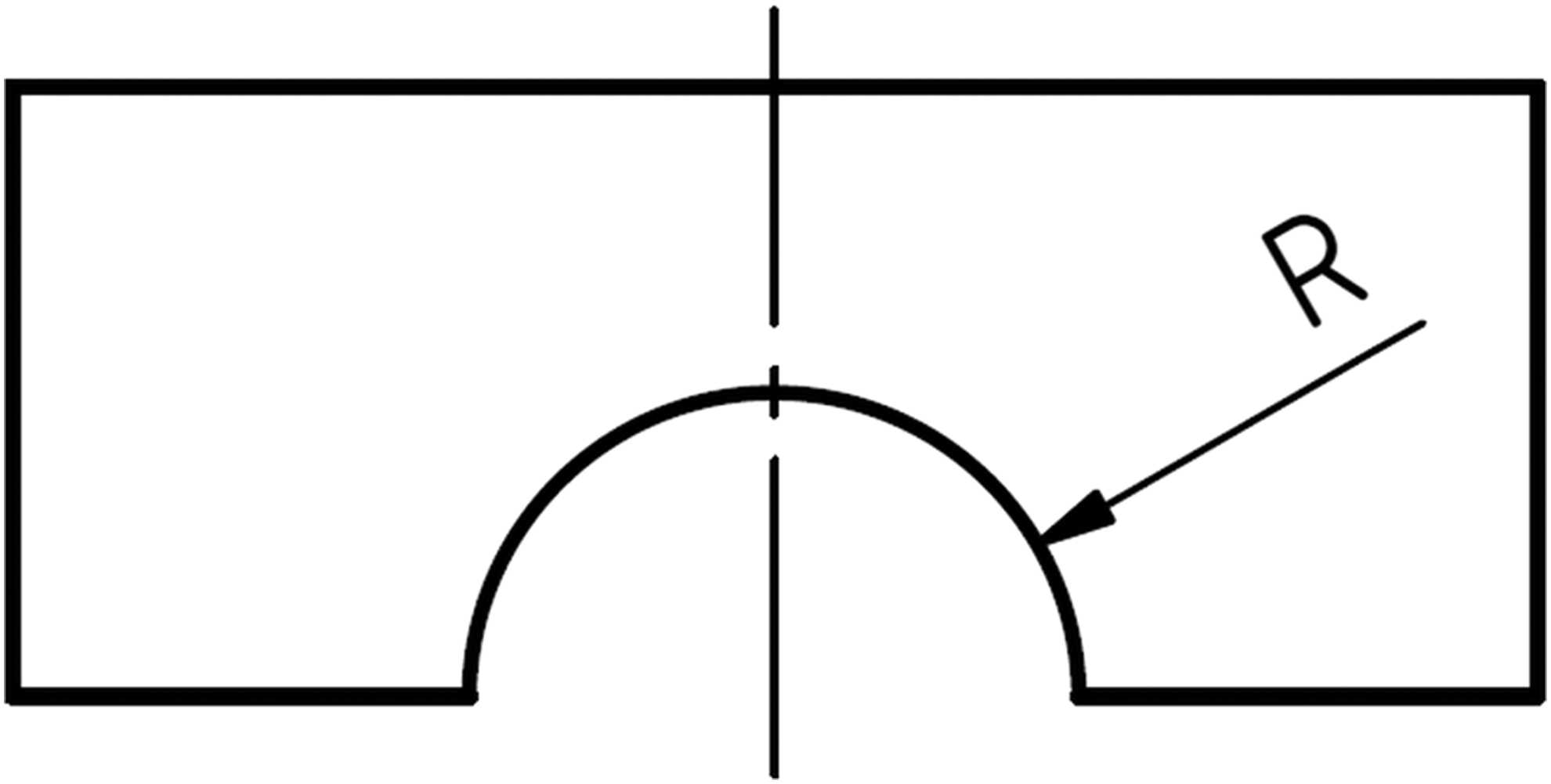
Technical drawing of a semicanal used to measure radial force of the Amplatzer Vascular Plugs. Radius (R) ranged from 2 to 6 mm. Two semicanals were placed together to simulate ureteral diameters of 4 to 12 mm.
2. Silicone tube
The latex-covered AVP was placed into a noncompliant, transparent, 50-cm long silicone tube with an inner diameter of 6 mm (comparable to a normal ureter) through a 12F vascular sheath. Once the plug exited the sheath, it expanded and pressed the latex stall against the tube wall. The plug was pushed into the tube either with or without axial compression leading to different configurations after deployment—i.e., fully longitudinally expanded vs compressed configuration. Axial compression was achieved by pushing the sheath slightly forward during plug deployment.
The upright tube was then filled with dyed water, and the lower part of the tube was observed for any water leakage. If there was detectable leakage, the time it took for a 40 cm column of water to drain out completely was measured (“drainage time”).
Measurements of drainage time were performed in three settings: (1) Immediately after AVP application, (2) after 1 hour at room temperature, and (3) after 1 hour in a bath of water at body temperature to test for remodeling effects of the nitinol mesh. All experiments were repeated five times for each AVP size and configuration.
Drainage time measurements (seconds) were logarithmized to ensure normal distribution of the data. Thereafter, statistical analysis was performed in a GLM to evaluate dependency of drainage time from AVP type, diameter, and remodeling effects (room vs body temperature). Finally, correlation analyses between drainage time and radial force in the corresponding 6-mm canal at room and body temperature were performed.
If no leakage past the plug was detectable initially, the tube was observed for 12 hours. After that, a manometer was connected to the tube, and the maximum pressure at which leakage or dislocation of the AVP occurred was measured.
3. Porcine ureter
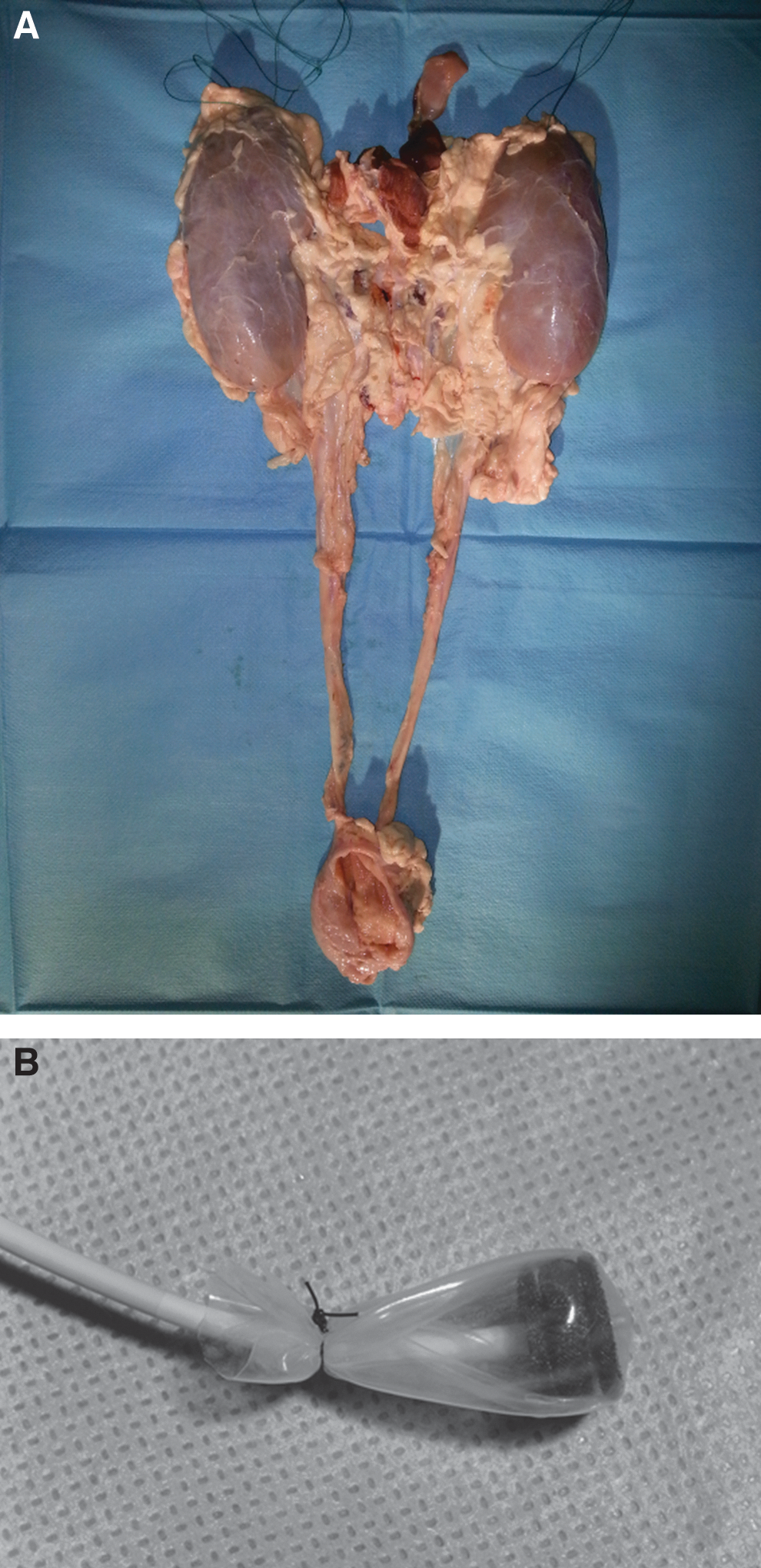
Ten explanted ureters complete with kidney and bladder were used from five adult domestic pigs (Fig. 2).
The sheath of an 18G Chiba needle was passed up the distal ureteral orifice from the bladder, and the lower urinary tract was filled with contrast agent to facilitate transrenal puncture of the renal pelvis. After successful puncture, a 0.035-inch J-wire was passed into the pelvis and down the ureter. The needle was exchanged for a dilator. After sequential dilation, a 14F vascular sheath was advanced down the ureter over a stiff wire.
An 8F sheath was then used to push the latex cover and AVP through the 14F sheath into position. Silicone spray was used as a lubricant to facilitate pushability of the latex cover. When the AVP exited the 8F sheath, it pressed the latex cover against the ureteral wall (Fig. 3). The 14F sheath was pulled back into the renal pelvis, the 8F sheath was removed, and contrast agent was administered manually.

Application methodology.
After that, an additional 4F pigtail catheter was advanced through the sheath into the renal pelvis. A syringe pump was connected to the sheath, and saline was infused at a constant rate of 1.5 mL/min. Pressure in the renal pelvis was constantly measured via the pigtail catheter. Kidney, renal pelvis, and ureter were observed under continuous fluoroscopy. Intrapelvic pressure was documented at 1 minute intervals. Infusion was terminated when leakage, dislocation of the plug, or rupture of the lower urinary tract with contrast extravasation was observed.
Pressure measurements were performed in two ureters of different pigs for each AVP II diameter. In the first ureter, measurements were obtained at room temperature; in the second, the ureteral segment containing the AVP II was placed in water at body temperature before measurements.
Results
Radial force
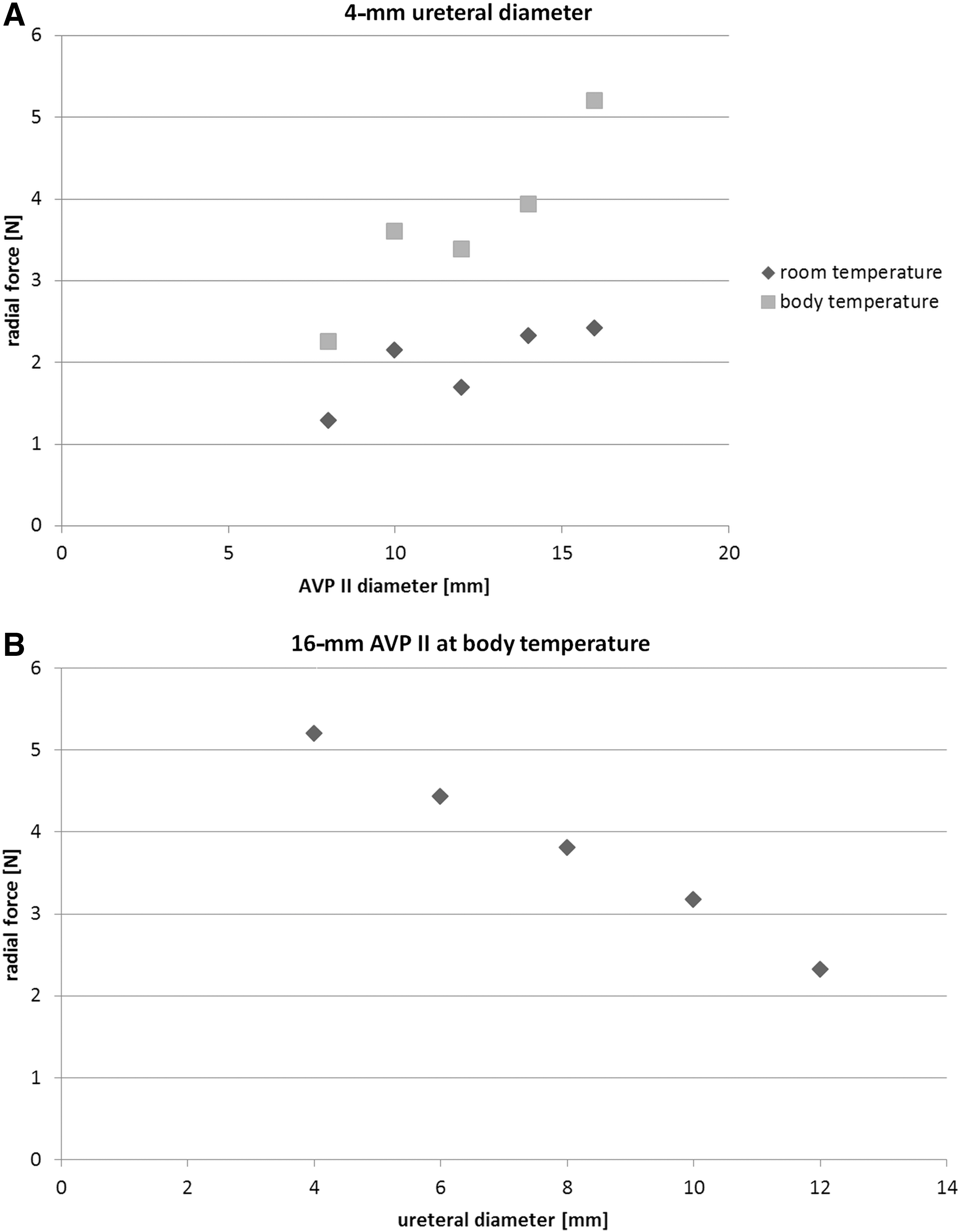
Mean radial force of the AVPs under different conditions was found to vary greatly, ranging from 0.43 N (8-mm AVP I in 6-mm canal at room temperature) to 5.26 N (16-mm AVP II in 4-mm canal at body temperature). The results of radial force measurements are summarized in Table 1.
AVP=Amplatzer Vascular Plug.
Radial force increased for each plug size with decreasing canal diameter and was generally significantly higher for larger plug diameters, with the exception of comparable radial force between the 14- and 16-mm AVP I at room and body temperature, and the 14- and 16-mm AVP II at room temperature. Radial force of the AVP II generally was significantly greater compared with the respective AVP I. Body temperature led to a statistically significant increase of radial force for each plug and canal diameter. The highest radial force of more than 5 N was measured for a 16-mm AVP II restrained to a diameter of 4 mm at body temperature.
Overall radial force was shown to be significantly related to AVP type (P<0.001), size (P<0.001), canal diameter (P<0.001), and temperature (P<0.001). See also Figure 4 for illustration.
Silicone tube
All experiments with an AVP type I showed considerable water leakage and frequent plug dislocation. AVP I diameter or configuration had no effect on occlusion. Because of insufficient sealing properties of the AVP I, subsequent experiments were performed with the AVP II only.
All AVP II placed into the silicone tube with axial compression supported a 40-cm water column for 12 hours regardless of plug diameter. Maximal pressure levels the plugs were able to withstand are given in Table 2.
SD=standard deviation.
All AVP II deployed without axial compression showed leakage to different degrees. Analysis showed the drainage time to be dependent on plug diameter (P<0.001) and remodeling effects at body temperature (P<0.001). Except for the 8-mm plug, leakage time 1 hour after application at room temperature was longer than that immediately after application (P<0.001, Bonferroni corrected), with the increase being most prominent for the 12-mm plug (6–165 sec mean drainage time).
Body temperature led to an additional significant increase in leakage time (P<0.001, Bonferroni corrected), most prominent for the 16-mm plug (25–4510 sec [i.e., more than 70 min] mean drainage time). There was a significant correlation between drainage time and radial force of the different AVPs measured in the 6-mm canal, corresponding to the inner diameter of the silicone tube (Pearson correlation coefficient r=0.731, P<0.001). The results of drainage time measurements are summarized in Table 2.
Porcine ureter
Continuous infusion of water led to an increase in pressure levels within the renal pelvis in all experiments. At room temperature, leakage past the AVP II was observed at different pressure levels for each plug diameter reaching from 19 to 93 cm H2O.
At body temperature, all AVP II occluded the ureter completely so that rupture of the renal pelvis occurred at 42 to 83 cm H2O (Fig. 5c). In one case of 16-mm AVP deployment, the cover was damaged because of friction within the sheath, leading to leakage at 69-mm Hg at body temperature. The experiment was therefore repeated using ultrasound gel in addition to silicone spray as a lubricant with subsequent complete occlusion. See Table 3 for details.

With rising intrapelvic pressure, increasing tubular reflux of contrast media can be observed.
In two cases in which the experiments could be performed only hours after explantation of the kidneys, radiographic monitoring showed increasing tubular reflux at 59 cm H2O (8-mm AVP) and 15 cm H2O (10-mm AVP) (Figs. 5 a, b, d).
Discussion
Transrenal ureteral occlusion today is a rather rare procedure. 7 In cases of clinically insufficient urine drainage by percutaneous nephrostomy alone, however, it can be advantageous to block free urine flow through the ureter. 1 Clinical indications for ureteral occlusion are, for example, lower urinary tract fistulas and leakages after gynecologic surgery, especially after radiation therapy in advanced pelvic malignancy, otherwise untreatable incontinence, and dysuria or postoperative pouch insufficiency. 1,2
Because open surgery is not feasible in many cases, several different interventional approaches have been developed over the last three decades to allow for minimally invasive treatment. 1
The most widely studied interventional techniques use a transrenal approach with a large variety of occlusive materials—e.g., isobutyl-2-cyanoacrylate, 8 nondetachable and detachable balloons, 9 –15 coil embolization and additional gelatin sponge, 12,13,16 –20 modified covered stents, 3,21 nylon or silicone plugs. 22,23 Other approaches used electrocautery or fulguration. 24 –27
Most of these techniques have not reached general acceptance because of several drawbacks. Cyanoacrylate is known to soften in contact with urine, leading to dislocation and the need for repeated reinterventions. 8,10 Detachable balloons can deflate and migrate 3 and have usually been filled with a silicone material 13 no longer commercially available, so that this technique is no longer an option. Coil embolization with the additional use of gelatin sponge can lead to effective occlusion, but coil separation and migration from peristaltic waves of the ureter can be a problem. 17,18 Finally, the application of nylon plugs necessitates a larger access size of 24F to 26F with the additional problem of frequent plug dislodgment. 22
Transrenal ureteral occlusion using a latex-covered AVP II has recently been suggested as a new alternative method by Schild and associates, 4 describing a case of a 62-year-old female patient with a large vesicovaginal fistula from advanced cervical cancer. A 12-mm latex-covered AVP II was used to completely occlude the ureter with a follow-up of 2 months.
Shabrang and colleagues, 5 on the other hand, proposed the use of an AVP II in combination with tissue adhesive. They raised the hypothetical issue of possible migration of a latex-covered plug. Likewise, Saad and coworkers 6 advocated using tissue adhesive between two AVP II in a “sandwich technique” to ensure permanent occlusion. In the only larger series of 10 ureters occluded with a latex-covered AVP II, no plug dislodgments were encountered. 2
We conducted this experimental study to learn more about the occlusive properties of an AVP covered by a latex finger stall and to find the ideal AVP type and size for transrenal ureteral occlusion.
Our in vitro experiments showed that in the scenario of a noncompliant silicone tube, sufficient immediate occlusion depended on plug configuration at the time of deployment. Only if a certain amount of axial compression was administered, an AVP II led to immediate, complete occlusion, supporting a water column of 40 cm regardless of AVP II diameter. Axial compression, therefore, is likely to lead to a higher radial force, pressing the latex cover firmly against the silicone tube. In cases of total occlusion, AVPs II with a diameter of 8, 10, 14, and 16 mm withstood a maximum pressure between 500 cm H2O and 1000 cm H2O before water was pressed past the plug. The 12-mm plug even withstood a pressure of more than 2000 cm H2O without any leakage.
In an in vivo study of porcine intrapelvic pressure, normal pressure was shown to be less than 14 cm H2O. In cases of complete subpelvic obstruction, values can rise to 27–54 cm H2O, leading to decreased diuretic activity. 28 –32 Pressure values more than 82–109 cm H2O led to tubular reflux in the kidney and between 82–245 cm H2O “blowout”—i.e., rupture, with contrast material extravasation occurring. 28 –31
The pressure levels measured in our in vitro study (500 to more than 2000 cm H2O) are therefore far beyond any physiologically achievable pressure.
Drainage time in AVP II embolization correlated significantly with radial force of the respective plug at 6-mm ureteral diameter. The force the plug exerts on the ureteral wall, therefore, seems to play an important role in successful occlusion. Because larger plugs exert higher radial pressure on the wall, it is arguable that these are better suited for successful occlusion. Deployment of a large (i.e., 16 mm) latex-covered AVP II, however, can be technically difficult because of high friction forces within the sheath, as reflected in damage to the latex cover in one case. One also has to bear in mind that the pressure the ureteral wall can withstand in vivo until necrosis occurs is unknown. Available data on this issue in general are scarce, and no exact measurements concerning this issue have so far been undertaken. Günther and colleagues 10 observed flattening of the urothelium and a minor ulceration in a canine ureter 3 weeks after occlusion using a detachable, silicone-filled balloon. In two studies on ureteral stent application, the authors observed mucosal thickening with squamous cell metaplasia and formation of granulation tissue, but no transmural necrosis, although the stents exerted a chronic outward pressure on the ureteral wall. 3,33
Although we never used an AVP type I clinically for ureteral occlusion, we tested the occlusive properties in the in vitro experiment. Because no AVP type I diameter or configuration led to complete occlusion, it is to be assumed that successful embolization depends also on the distance over which the cover is pressed against the tube wall. The AVP II is generally longer than type I because of additional disks at each end and therefore seems to be more suited for ureteral occlusion.
The AVP itself consists of a nitinol mesh with a temperature dependent inherent memory effect leading to plug remodeling over time. 34 This effect could be seen in the radial force measurements. Radial force of a deployed AVP II ranged from 1 to 2.5 N at room temperature and 2 to more than 5 N at body temperature at the smallest examined ureteral diameter (4 mm) depending on the AVP diameter. Radial force increased linearly with decreasing ureteral diameter (Fig. 4). Because the temperature dependent reconfiguration of the nitinol mesh of the AVP is likely to produce even tighter sealing of the ureter over time, we repeated measurements in all cases of initial leakage in the silicone tube after 1 hour at room temperature and after 1 hour at body temperature for the AVP II. One hour at room temperature led to only slightly better occlusion with the exception of the 12-mm plug, whereas 1 hour at body temperature produced a significantly better occlusion, with even near total obstruction with the 16-mm plug.
As described above, normal intrapelvic pressure in living pigs is less than 14 cm H2O with a possible increase up to 54 cm H2O in subpelvic obstruction. 28 –32
Intrapelvic pressure measurements in our study of explanted porcine ureters showed first slight leakage past the AVP II to occur between 63 and 92 cm H2O for AVP II diameters 10 to 16 mm at room temperature. Only the 8-mm AVP II showed leakage at 19 cm H2O, possibly because of insufficient radial force of this rather small AVP at room temperature.
Experiments at body temperature, on the other hand, showed blowout of the lower urinary tract at 42 to 83 cm H2O. Most of these pressure values exceed the pressure of 54 cm H2O that can be achieved in complete subpelvic obstruction, so that it is to be assumed that the occlusive material would withstand intrapelvic pressures under physiological conditions. Blowout pressure in the human lower urinary tract has, to our knowledge, not been studied, but it is to be assumed that pressure levels are comparable to those measured in the pig model by Donkervoort and coworkers. 28 –31 One also has to bear in mind that in a clinical setting, ureteral occlusion is always combined with urinary diversion. Urinary drainage via a nephrostomy tube would cancel out any pressure gradient in human application. Pressure levels higher than the hydrostatic pressure would, therefore, only be encountered in cases of nephrostomy dysfunction.
The fact that we observed blowout at lower pressure levels than in the in vivo setting of Donkervoort and coworkers 28 –31 is most likely to be attributed to the absence of protective surrounding tissue in the explanted kidneys and isolated ureters. Interindividual resilience of the lower urinary tract, as well as possible minor damage to the ureters during explantation of the porcine urinary system, or AVP implantation procedure may also play a role in the individual blowout pressure level. This question cannot be addressed in more detail because of the number of available kidneys in our experiments.
Results of the experiments, however, suggest that hydronephrosis would occur in vivo before leakage past the latex-covered AVP II, especially taking remodeling effects at body temperature because of the inherent memory effect of the nitinol into account. These effects lead to an even tighter occlusion under physiologic conditions. Our results further showed that in contrast to the theoretical problem of dislocation of a latex-covered plug raised by Shabrang and associates 5 and Saad and colleagues, 6 AVP dislodgment in the silicone tube did only occur at pressure levels (more than 500 to more than 2000 cm H2O) that cannot be achieved under physiologic conditions. In explanted porcine kidneys, we observed no plug dislocations before blowout. In vivo inflammatory reactions to the foreign body in the ureter are likely to further secure complete occlusion. Such chronic inflammatory reactions with ureteral wall thickening, fold formation, and granulation tissue have been observed in several animal studies using coils or stents as occlusive material. 3,17,18,33
One might argue that hyperperistaltic waves might lead to plug dislocation in vivo. Hyperperistalsis, however, is known to produce pressure levels of 27 to 95 cm H2O only in cases of insufficient drainage via a nephrostomy. 17 Accordingly, Pieper and coworkers 2 observed no plug dislocations in a series of 10 AVP II ureteral occlusions.
Our data are limited by the experimental character of this study with limited transferability to an in vivo, human application. Furthermore, only a single set of AVPs was available. It is arguable that radial force may vary between different AVPs of the same diameter. The measuring technique of radial force is certainly not completely accurate and primarily intended to allow for comparison between different AVP types and sizes.
Conclusion
The results of our experimental study indicate that a latex-covered AVP II of any diameter between 8 and 16 mm can lead to effective ureteral occlusion. Successful occlusion seems to depend primarily on the radial force exerted on the ureteral wall and the occlusion distance—i.e., length of the implanted latex-covered AVP. An AVP type I generally seems not to be suitable for ureteral occlusion.
In contrast to the concerns of other authors, we only observed plug dislocation at pressure levels that cannot be achieved in vivo. Because larger AVP diameters are able to maintain a sufficient radial force on the ureteral wall even in a dilated ureter, they should be preferred to achieve long-term occlusion. Because plug application of a 16-mm plug can be technically challenging from friction within the sheath, we advocate the use of a 12- or 14-mm AVP type II in combination with lubricant within the sheath for embolization. Further in vivo studies, however, are warranted to study the effects of a latex-covered foreign body and associated pressure on the ureteral wall.
Footnotes
Acknowledgments
The authors would like to thank Philipp Hänisch (leading engineer of fine mechanics, Department of Physics, University of Bonn) and Jennifer Nadal (Institute for Medical Biometry, Informatics and Epidemiology, University of Bonn) for their support.
We further would like to thank St. Jude Medical for providing us with the studied Amplatzer Vascular Plugs (type I and II) of different diameters.
Disclosure Statement
No competing financial interests exist.