
Abstract
The aim of this study is to examine the role of robotic partial nephrectomy (RPN) in the management of caliceal diverticula by assessing our single-center outcomes. Between July 2007 and July 2013, 7 of 670 patients underwent RPN procedures as a reason of caliceal diverticula. The indications for RPN in all cases were recurrent urinary tract infection and pain attributed to the diverticulum in addition to failed management by endourologic or extracorporeal shockwave lithotripsy (SWL) treatments. One patient with a calcified diverticulum and another with an unsuccessful SWL treatment underwent RPN without further endourologic intervention. The other five patients had a history of unsuccessful percutaneous nephrolithotomy (one case), ureteroscopy (URS) (two cases), and a combination of SWL+URS (two cases). No intraoperative or postoperative complications were observed. No patient was readmitted postoperatively. Unique features of the robotic platform facilitate the excision of diverticulum and subsequent kidney reconstruction for this benign, but complex pathology.
Introduction
R
Caliceal diverticula are uncommon urothelial lined cyst-like structures that may communicate with the renal collecting system. They often are associated with stones, pain, and chronic infection. Endoscopic techniques (ureteroscopy [URS] or percutaneous nephrolithotomy [PCNL]) are often attempted as first-line treatments, but extirpative therapy may be required if endoscopic treatment is unsuccessful or the anatomy mandates.
The aim of this study is to examine the role of RPN in the management of caliceal diverticula by assessing our single-center outcomes.
Materials and Methods
Our Institutional Review Board approved prospectively maintained database was queried to identify patients who underwent RPN for caliceal diverticula. Of 670 RPN procedures completed during the study period (July 2007–July 2013), 7 met the study inclusion criteria and were included in the analysis (Table 1).
PCNL=percutaneous nephrolithotomy; SWL=extracorporeal shockwave lithotripsy; URS=ureteroscopy.
The indications for RPN in all cases were recurrent urinary tract infection and pain attributed to the diverticulum in addition to failed management by endourologic or extracorporeal shockwave lithotripsy (SWL) treatments. One patient with a calcified diverticulum and another with an unsuccessful SWL treatment underwent RPN without further endourologic intervention. The other five patients had a history of unsuccessful PCNL (one case), URS (two cases), and a combination of SWL+URS (two cases).
Surgical technique
Our RPN technique for renal masses has been standardized and previously reported. 5 For cases of a peripheral caliceal diverticulum, a cystoscopy and retrograde pyelogram were performed to confirm the communication between the collecting system and the diverticulum. A 5F ureteral catheter was kept indwelling in the ureter and attached to a syringe of dilute indigo carmine/methylene blue. The diverticulum is identified using intraoperative ultrasound and visual cues, is unroofed, and all stones are removed. Visualization of the diverticular neck is aided by retrograde injection of dilute indigo carmine/methylene blue and is closed using a 2-0 Vicryl suture in a figure of 8 configuration. No ureteral catheter or stent is left in place, whereas a Foley catheter and a closed suction drain are left indwelling.
In cases of a central, intraparenchymal diverticulum, a more standard RPN is performed for complete resection of the cavity. We preferably employ a three-arm transperitoneal approach, although a four-arm technique can be used (Fig. 1). Key steps of the procedure include colon mobilization, hilar dissection, and mobilization of the kidney with Gerota's fascia. An intraoperative drop-in, flexible, ultrasound probe (ProART Robotic Drop-In Transducer 8826; BK Medical, Peabody, MA) is used by the console surgeon to identify and mark the margins of the diverticulum as no portion of the structure is exophytic. Often stones within the diverticulum cause shadowing, which can help confirm the location. Ischemia is then initiated using bulldog clamps and the diverticulum is completely excised. The base of the defect is then over sewing using a 2-0 Vicryl running suture and the capsule is reapproximated in a continuous horizontal mattress configuration using an 0-Vicryl suture and sliding hem-o-lok clips, as previously described. 5 The hilum is unclamped and a closed suction drain and Foley catheter are left indwelling. The Foley catheter and the drain are removed sequentially on the first postoperative day.
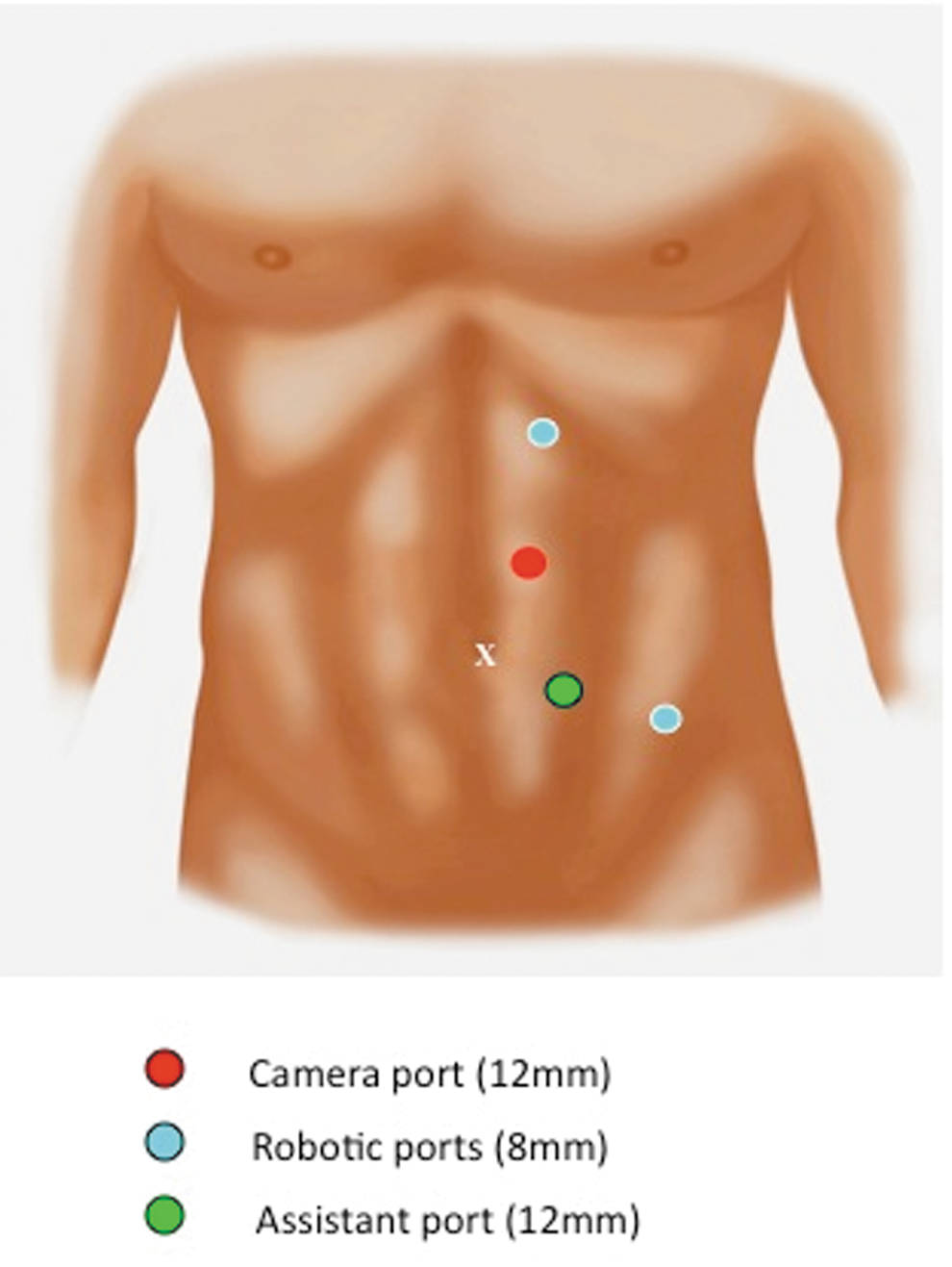
Port position for left side robotic partial nephrectomy for caliceal diverticulum.
Results
Three surgeons performed all the procedures. The median age of the patients was 37 years (range 18–47 years). Female patients were more prevalent (n=6, 85.7%). Hilar clamping was performed selectively with sequential arterial and venous bulldog clamping in three patients, only arterial bulldog clamping in one patient, and zero ischemia in three patients. The median warm ischemia time was 20 minutes (range 18–21 minutes), and the median operative time was 150 minutes (range 99–222 minutes). There was no significant difference between preoperative and postoperative estimated glomerular filtration rate (p=0.364) (Table 2). No intraoperative or postoperative complications were observed. No patient was readmitted postoperatively. All patients reported resolution of symptoms postoperatively. Within the short median follow-up of 1 month, no patient reported recurrence of symptoms.
BMI=body mass index; ASA=American Society of Anesthesiologists; eGFR=estimated glomerular filtration rate; IQR=interquartile range.
Discussion
To the best of our knowledge, this report is the first series of RPN for the treatment of caliceal diverticulum. Despite the small sample size, our experience suggests that robotic surgery represents a viable option for minimally invasive management of selected patients, especially after failed endoscopic attempts.
Urine enters the diverticulum from the pyelocaliceal system through a narrow infundibulum in a retrograde manner. 6 Stone formation as a complication of a caliceal diverticulum occurs in 10% to 50% of cases. 7 Although often asymptomatic and requiring no treatment, caliceal diverticula may be associated with flank pain, hematuria, or urinary tract infection so that intervention may be necessary. Caliceal diverticula commonly represent a therapeutic challenge. Minimally invasive treatments are available for the management of symptomatic caliceal diverticula, including SWL, 8 retrograde intrarenal surgery, 9 percutaneous surgery, 10 or laparoscopy. 11,12
Despite poor stone-free rates, patients achieve symptomatic relief after SWL. Streem and Yost reported 86% symptomatic relief despite a stone-free rate of 58% in a selected group of patients with caliceal diverticula associated with short diverticular neck and stones less than 15 mm. 8 Ureteroscopic management, including laser infundibulotomy and simultaneous stone removal, provides unique treatment options for caliceal diverticula for stones less than 15 mm in size. 9 Percutaneous management of a caliceal diverticulum can be effective especially in cases with a large stone burden. Limitations of this approach include difficulties with treatment of anterior diverticula, intraoperative loss of the percutaneous tract due to a thin surrounding parenchymal wall, and persistence of the diverticular cavity after the procedure. 10 Laparoscopy has been a more useful approach for anterior, large diverticula or in cases with a history of failed endourologic management of diverticula. 11,12
In the fields of robotics, Driscoll and Kim reported their experience with a single case of robotic diverticulectomy in 2007. 3 They described a case of a 14-year-old girl with a large cystic structure originating from the right upper and anterior portion of the kidney. They initially performed a retrograde pyelogram and placed a 4F ureteral catheter for easier identification of the diverticular neck. Then, they performed a robotic excision of the diverticulum wall and closure of the diverticular neck using a 5-0 Vicryl suture. Indigo carmine was injected and verified a watertight seal closure. The back wall of the diverticulum was left in place and fulgurated.
In the present case series, none of our patients could be successfully managed with SWL or an endourologic approach although one patient did not undergo an attempt at either of these procedures as his diverticulum was completely calcified. Six patients presented with stones associated with the diverticulum, and all RPN procedures were completed without intraoperative complications. No postoperative urine leak occurred and no patient required hospital readmission.
For standard laparoscopy or robotics, 13 lesions must first be located once the kidney is properly exposed. Intraoperative laparoscopic real-time ultrasonography is a requirement in nearly all cases, as caliceal diverticula are not exophytic and can rarely be identified unless the cavity is larger and peripheral. For peripheral cavities, unroofing and over sewing of the infundibulum are often successful. Retrograde injection of indigo carmine/methylene blue allows visualization of the diverticular opening. For smaller central diverticula, a standard RPN with complete excision is advised. As laparoscopic suturing can be difficult and time-consuming, the use of the robotic platform can facilitate this task, given its unique features.
Conclusion
Symptomatic caliceal diverticula can be effectively managed by using a minimally invasive robotic approach. Urologists who may already be comfortable with standard RPN can consider this specific subset of cases. Unique features of the robotic platform facilitate the excision of the diverticulum and subsequent kidney reconstruction for this benign, but complex pathology.
Footnotes
Disclosure Statement
J.H.K., consultant to companies “Intuitive, Endocare and Ethicon”; G.P.H., consultant to companies “Intuitive, Baxter, Merck”; R.A., consultant to company “Willy”; the remaining authors have no disclosures.