
Abstract
Purpose:
To produce and validate a predictive model based on CT parameters for calculating the probability of a stone to be visible on fluoroscopy of shockwave lithotripsy (SWL) and to compare its accuracy to that of kidneys-ureters-bladder (KUB) radiography.
Methods:
We retrospectively analyzed 306 patients (sample group) who underwent an SWL between March 2011 and August 2012. A multivariate analysis of several parameters extracted from the preoperative CT scan was conducted to identify independent predictors for radiopacity on SWL fluoroscopy. The results were used for the creation of a predictive model. Internal validation was made on a group of 75 patients (validation group) treated from September 2012 until December 2012. Predictive accuracy of the model was evaluated by receiver operating characteristic (ROC) curve and calibration plot. The ROC curve was also used for comparing the predictive accuracy of the model to that of KUB radiography.
Results:
From 306 evaluated stones, 238 (77.8%) were visible on fluoroscopy. Results of the multivariate analysis revealed that stone size (P<0.001), stone attenuation (P<0.001), location in the midureter (P<0.001), the distance between the stone and the anterior abdominal wall (P<0.001), and fat thickness of the anterior abdominal wall (P=0.001) were all independent predictors for stone radiopacity on fluoroscopy. A predictive model was produced based on the above parameters. The model demonstrated high calibration and areas under the curve of 0.923 and 0.965 in the sample and validation group, respectively, while its predictive performance was significantly higher (P<0.001) of that of KUB radiography (area under the curve=0.727).
Conclusions:
This novel model can estimate with high accuracy stone radiopacity on SWL fluoroscopy using parameters of CT scan and thus it can be used as an alternative to KUB radiography for treatment planning.
Introduction
E
At present, a noncontrast abdominal CT (NCCT) scan represents the preferred imaging modality for the detection of renal stones because of its high sensitivity and specificity. Its advantage over conventional radiographic studies is mainly the identification of radiolucent stones and the determination of other important parameters, such as stone density and stone to skin distance, which may influence treatment outcomes. 5,6 The NCCT scan cannot give information regarding stone radiopacity on fluoroscopy, however. Kidneys-ureters-bladder (KUB) radiography is used additional to NCCT for the preoperative planning of SWL. Not all radiopaque stones on KUB radiography are radiolucent in fluoroscopy as well, however. Identifying these stones that will be radiopaque on fluoroscopy is of paramount importance because it may influence treatment planning.
Because the primary radiologic examination applied to patients with urolithiasis is NCCT, the creation of a predictive model based on NCCT parameters, standing as an alternative to KUB radiography, would be optimal. Such a predictive model would diminish the need for an additional KUB film, and consequently it would decrease radiation exposure, it would assist patient consultation for potential treatment options, and it would decrease the therapeutic management cost, because patients with radiolucent stones on fluoroscopy can have alternative treatment options.
The aim of the present study was to evaluate several clinical and radiologic parameters extracted from preoperative NCCT in patients with urolithiasis for identifying independent predictors for stone visibility on fluoroscopy during SWL and to produce a preoperative predictive model for the calculation of this probability. The second objective was to compare the predictive accuracy of the model with the predictive ability of preoperative KUB radiography.
Methods
After we obtained an Ethics Committee approval, we reviewed prospectively collected data of SWL procedures in our department, and we conducted an analysis of 417 consecutive patients who underwent SWL for renal stones between March 2011 and August 2012 with a Dornier Gemini electro-magnetic lithotripter (Dornier MedTech, GmbH, Germany). All procedures were performed by the same operator under supervision of the same urologist.
All patients included in the study had both preoperative KUB radiography and NCCT. Patients missing KUB radiography (32 patients) or NCCT (79 patients) were excluded; finally, 306 patients entered the analysis (sample group). The preoperative NCCT scan was used for the calculation of Hounsfield units (HU). Transverse views were used for the measurement of stone to anterior abdominal wall distance, anterior to posterior abdominal wall distance, and fat thickness of the anterior abdominal wall (Fig. 1). Stone size was defined as the maximal diameter of the calculus in either the sagittal, transverse, or coronal plane. Stones that were located in the area of the sacroiliac joint were defined as midureteral stones. Evaluation of preoperative NCCT and KUB films were made by a single physician.
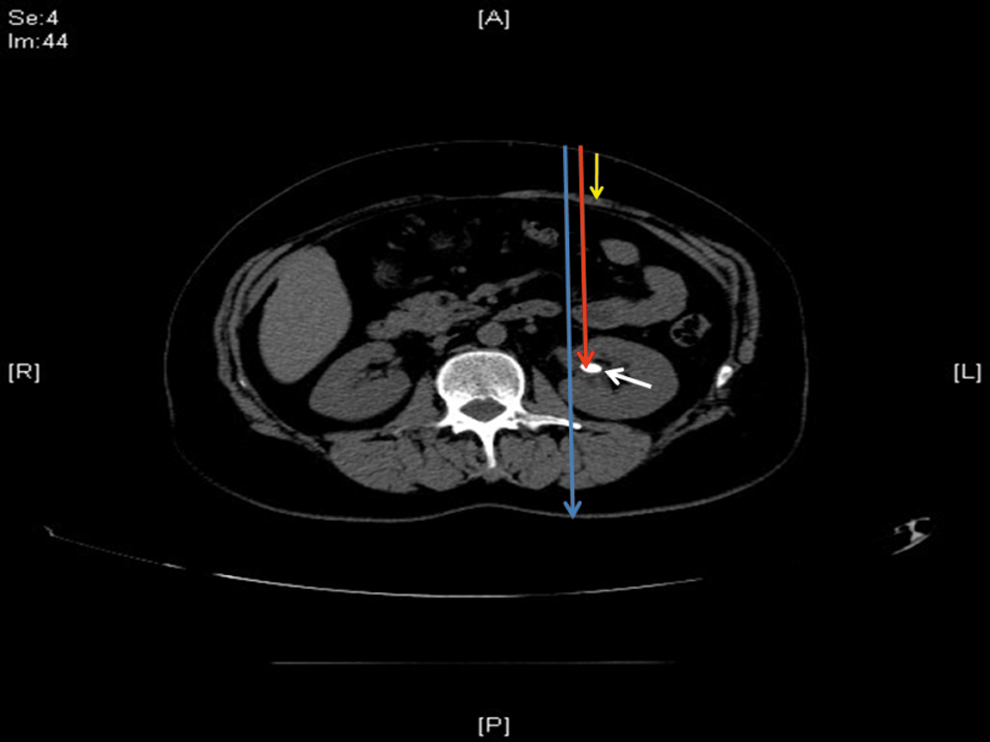
A non-contrast CT scan of a patient with a 13-mm stone in the left renal pelvis (white arrow). Information regarding anterior-posterior diameter (blue arrow), stone to anterior abdominal wall distance (red arrow), and fat thickness of the anterior abdominal wall (yellow arrow) was obtained.
All procedures were made with the patient in the supine position under sedation. Fluoroscopy was applied through the lithotripter device. The fluoroscopy setup was constant in all cases. The pulsed mode was used, and image settings were autoadjusted for optimal imaging, fixed by the manufacturer at 40–125 kV and 0.2–12.5 mA. Evaluation of stone visibility was attempted either in the sagittal plane or at 30 degrees to the cephalic or caudal axis by a single operator. Stones of uncertain visibility were considered as radiolucent.
Patients were divided into two groups according to stone radiopacity on fluoroscopy. Group A consisted of patients with radiopaque stones on fluoroscopy and group B with radiolucent ones. Intraoperative retrograde urography was used in patients in group B for stone identification and facilitation of stone targeting.
Statistical analysis was performed by SPSS software version 17 (SPSS Inc, Chicago, IL) and MedCalc software version 12.5 (MedCalc software bvba, Ostend, Belgium). Numeric variables are presented as mean±standard deviation (SD) and interquartile range (IQR). Categoric variables are described by their absolute number and percent frequency. The Mann-Whitney U test was used to compare means of numerical variables. The chi-square test was used to compare categoric variables. A multiple logistic regression analysis with a backward variable selection procedure was used to identify independent predictors. Variable selection was performed using the “step-down” method suggested by Harrell and associates, 7 and the model was reduced until achieving the best discrimination.
To produce a predictive model, we firstly calculated the logit by adding beta weights. Logit was used to compute the odds and the latter converted to probability through the equation: Probability=odds/1+odds. The final model coefficients were used to create a user-friendly web-based calculator, giving the name FLUO.R.O. (Fluoroscopy RadiOpaque) that estimates the probability of a stone to be visible on fluoroscopy and can be downloaded at the following link:
The predictive performance of the model was quantified and compared with that of KUB radiography by the area under the curve (AUC) and DeLong test. A calibration plot was generated to assess the discrimination capacity of the model.
The predictive model was internally validated using the medical data of 75 consecutive patients who underwent SWL from September 2012 until December 2012 (validation group). Validity was assessed by comparing the C-indexes of the sample group and validation group.
All P values were two-tailed, with statistical significance set at 0.05. All confidence intervals were calculated at the 95% level.
Results
A total of 306 patients were recruited for the construction of the predictive model. Study population consisted by 238 (77.8%) males and 68 (22.2%) females with a median age of 48 years (48.6±14.1, 20). Median stone size was 9.14 mm (9.59±3.68, 4.79). One hundred and forty stones (45.8%) were found in the right side and 166 (54.2%) stones in the left side. Topographic distribution was as following: 7 (2.29%) stones were located in an upper calix, 24 (7.84%) in a middle calix, 77 (25.2%) in a lower calix, 55 (18.0%) in the renal pelvis, 72 (23.5%) in the proximal ureter, 22 (7.19%) in the midureter, and 49 (16.0%) stones in the distal ureter. Radiopaque stones on both KUB radiography and fluoroscopy were found in 240 (78.4%) and 238 (77.8%) of the patients, respectively.
Study cohort characteristics are seen in Table 1. As expected, there was a statistically significant correlation (P<0.001) between KUB radiography and fluoroscopy radiopacity. Stone size (P<0.001) and stone attenuation in HU (P<0.001) were significantly higher in patients of group B. The anterior-posterior abdominal diameter (P=0.011), stone to anterior abdominal wall distance (P=0.002), and fat thickness of the anterior abdominal wall (P<0.001) were significantly higher, as well. Midureteral stone location was negatively associated with radiopacity on fluoroscopy (P<0.001). Significant parameters in the univariate analysis entered a multivariate regression analysis for the extraction of independent predictors (Table 2). Finally, stone size (P<0.001), HU (P<0.001), location in the midureter (P<0.001), stone to anterior abdominal wall distance (P<0.001), and fat thickness of the anterior abdominal wall (P=0.001) were found to be significant independent predictors for stone radiopacity on fluoroscopy.
Chi-square test.
Mann-Whitney U test.
Statistically significant.
SD=standard deviation, IQR=interquartile range; KUB=kidneys, ureters, and bladder; HU=Hounsfield units; AP=anterior-posterior.
Statistically significant.
CI=confidence interval; HU=Hounsfield units.
Using the results of the regression analysis, we created the following equation for the calculation of the accumulative probability of a stone to be visible in fluoroscopy: elogit/1+elogit, where e=2.71828 and logit=0.203+[0.304*stone size (in mm)]+(0.005*HU) - [3.087*midureteral stone (if yes=1, if no=0)] - [0.029*stone to skin distance (in mm)] - [0.078*fat thickness of the anterior abdominal wall (in mm)]. The html version of FLUO.R.O. calculator can be downloaded through the following link:
The FLUO.R.O. model was internally validated in 75 patients. Characteristics of patients in the validation group are seen in Table 3. The predictive performance was evaluated with receiver operating characteristic curve analysis (Fig. 2) and with calibration plot (Fig. 3). The AUC of FLUO.R.O. in the study group was 0.923 (P<0.001, confidence interval [CI]: 0.886–0.961, standard error=0.019), and the AUC of the model in the validation group was 0.965 (P<0.001, CI: 0.894–0.994, standard error=0.024).

FLUO.R.O. (Fluoroscopy RadiOpaque) predicting performance in the sample group and validation group. AUC=area under the curve; SE=standard error.
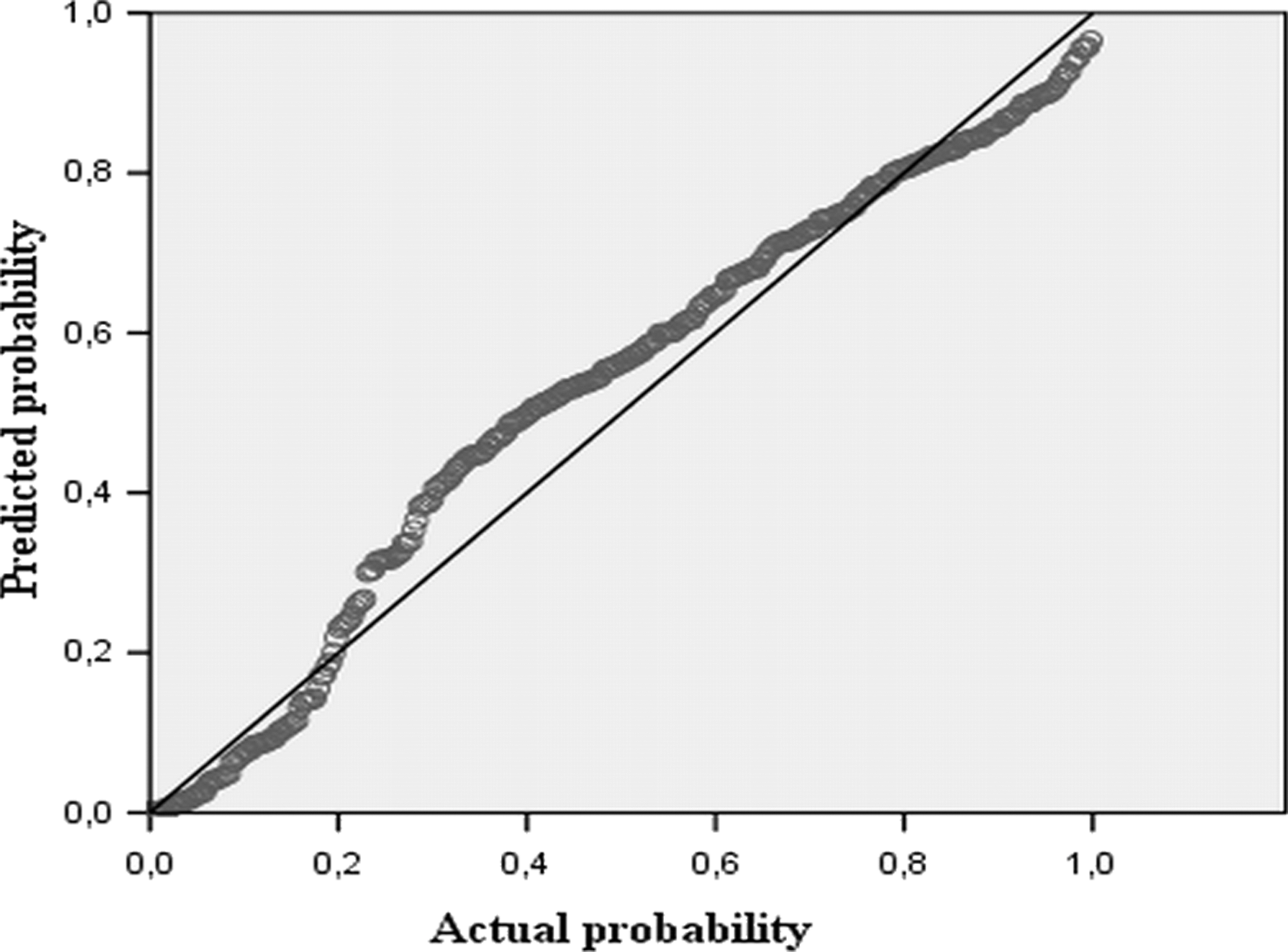
Calibration plot of the model.
SD=standard deviation; IQR=interquartile range; KUB=kidneys, ureters, and bladder; HU=Hounsfield units.
KUB radiography could significantly predict radiopacity on fluoroscopy (P<0.001). FLUO.R.O performed better than KUB radiography (P<0.001), however, in the validation group (Fig. 4). FLUO.R.O. and KUB AUC was 0.965 (CI: 0.894–0.994, standard error=0.024), and 0.727 (CI: 0.611–0.823, standard error=0.063), respectively.

Predictive performance of FLUO.R.O. (Fluoroscopy RadiOpaque) vs kidneys-ureters, and bladder (KUB) radiography.
Discussion
In the era of contemporary radiologic examinations with high sensitivity and specificity for the detection of renal stones, the diagnosis of urolithiasis is based on an NCCT scan. Patients with renal stone disease are referred for consultation to centers of expertise with a NCCT as the primary and sole examination. In these patients who fulfill the criteria for SWL treatment, the question of stone radiopacity is rising. Consequently, an additional KUB radiography is usually asked to answer the question and to assist treatment planning.
Identification of stones with high potential to be visible on fluoroscopy during SWL, without the need for supplementary KUB radiography, would be an optimal scenario. Furthermore, if the estimation of radiopacity is based on NCCT parameters, this would be ideal. Based on this concept, we produced a novel and simple to use predictive model, using parameters extracted by the NCCT, which can predict with high accuracy the probability of a stone to be identifiable in fluoroscopy during SWL.
The benefits of using a predictive model for estimating stone radiopacity are multiple. Using statistics and technology to produce predictive models represents a latest diagnostic and therapeutic shift in modern medicine providing a quick and accurate computation of the probability of a certain medical dilemma to occur, avoiding the application of supplementary, time-consuming, and sometimes invasive modalities. Practically, a predictive model is a device using a mathematical formula to predict the probability of an outcome, optimized for predictive accuracy. Predictive models allow continuous variables to remain continuous, maximizing their predictive power. Furthermore, they allow for the convergent use of all important parameters, in order for the most accurate prediction model to be built. Our predictive model is based on imaging parameters, such as stone size, location, and attenuation providing high predictive accuracy.
Stone size and stone attenuation, measured in HU, are well-known parameters influencing radiopacity. 8 –10 This finding was proved in our study as well, and both parameters reached high statistical significance and entered the predictive model. On the other hand, it has been reported that stone location does not influence stone radiopacity, unless a stone is located in the midureter. 8,10 This can be explained by the fact that the sacroiliac joint is a highly attenuating anatomic structure and consequently an overlying ureteral stone cannot be easily identified during fluoroscopy. The findings of our study are totally consistent with this. Midureteral stones were found to have a significantly lower likehood of being visible compared with stones located elsewhere in the ureter or in the collecting system.
There is limited knowledge regarding the impact of body dimensional parameters in stone radiopacity. A recent study reported that anterior-posterior diameter, measured at the level of the stone in the axial plane, was significantly associated with radiopacity. 9 In our study, we evaluated anterior-posterior diameter and some dimensional surrogates, specifically stone to anterior abdominal wall distance and fat thickness of the anterior abdominal wall. Both surrogates found to be significant and entered the FLUO.R.O. predictive model in contrast to anterior-posterior diameter that failed to reach significance.
Avoiding pre-SWL KUB radiography appears a fascinating option. Apart from minimizing the radiation exposure, our model can save time and money. Given the worldwide financial constraints in national medical systems, replacing examinations with simplified predictive models or nomograms is an appealing option. Referring patients for additional examinations presupposes the expense of time for the patient (missing working hours) and for the national health system (appointments for radiologic investigations, reconsultation by an urologist) that could be invested for other medical purposes. Pointing to patients' quality of life, a fast and reliable consultation would accelerate treatment and decrease the need for additional examinations and consultations. The FLUO.R.O calculator can stand as an efficient and accurate tool providing reliable assistance for treatment planning.
The advent of CT has revolutionized the imaging of urinary stone disease, and NCCT has emerged as a highly accurate modality for the identification of renal stones with sensitivity and specificity to reach 100%. 11,12 The implementation of low-dose CT protocols has decreased radiation exposure compared with conventional-dose ones without compromising the diagnostic ability. 13
Recent data suggest that NCCT preserves high sensitivity and specificity even under very low-dose protocols with similar radiation exposure to that of plain KUB radiography. 14 On the other hand, sensitivity and specificity of KUB radiography is 44% to 77% and 80% to 87%, respectively, and it is not suggested as a routine diagnostic examination for patients with urolithiasis if NCCT is considered. 15,16 The presence of phleboliths, vessel calcifications, obesity, and bowel gases decrease its diagnostic accuracy for renal calculi. KUB radiography is mainly reserved for the follow-up of patients with nephrolithiasis and as an additional examination to NCCT for SWL candidates to determine stone radiopacity. There are no published studies evaluating the sensitivity of KUB radiography in identifying radiopaque stones on fluoroscopy.
Based on the results of the present study, we showed that KUB radiography has a high predictive accuracy in identifying radiopaque stones on fluoroscopy with 90% of the KUB radiopaque stones visible on fluoroscopy. The FLUO.R.O. model, however, revealed higher predictive accuracy when compared with that of KUB radiography, and consequently it can be assumed as a reliable and efficient alternative.
To our knowledge, this is the first published predictive model to calculate the probability of a renal stone to be visible on fluoroscopy for patients undergoing SWL. In addition, this is the first study to compare KUB radiography with an alternative option for estimating stone radiopacity. The potential weakness of the present study may be the retrospective fashion. Data collection was made prospectively, however, and evaluation of all medical information was performed by a single urologist increasing reliability and consistency of the data. Internal validation was performed for the evaluation of the model's predictive performance. To further evaluate the predictive performance of our model, an ongoing prospective validation has been initiated in our institution.
It will also be necessary to perform external validation to investigate the differences between institutions and lithotripters. All procedures were performed with a single lithotripter system that is not available in all institutes, meaning that fluoroscopy images may vary depending on the system setup and settings, and thus the present results may not be extended to other systems. We believe that multi-institutional validation will assess the clinical importance and reliability of our model and it will further demonstrate its clinical usefulness. Finally, the cost of any differentiation of the common clinical practice should be evaluated. In the present study, we did not compare the cost benefit of our nomogram, and this remains to be examined in future studies.
Conclusions
Radiopacity of stones in candidates for SWL can be predicted by a novel predictive model. The FLUO.R.O. calculator may replace KUB radiography in the treatment planning of patients with urolithiasis with high efficiency and accuracy.
Footnotes
Disclosure Statement
No competing financial interests exist.