
Abstract
Background and Purpose:
Laparoscopic pyeloplasty has emerged as the gold standard for repair of ureteropelvic junction obstruction. Microlaparoscopic (MLP, <3 mm) instrumentation has improved markedly and can now be used for suturing and complex dissection needed during laparoscopic pyeloplasty. We present our experience with microlaparoscopy compared with conventional laparoscopy for transperitoneal pyeloplasty.
Methods:
We performed a retrospective analysis of hybrid MLP, using a 5-mm camera in a hidden umbilical incision, and 1.9 or 3 mm working instruments and compared with patients undergoing conventional laparoscopic pyeloplasty (CLP). The data for MLP and CLP were compared using the Student t test, Pearson chi-square test, and Fisher exact test, where appropriate.
Results:
Between January 2009 and May 2013, there were 19 MLP and 27 CLP procedures performed. The MLP group mean age was younger than the CLP group (34 vs 50 years; P=0.0003). Body mass index, previous treatment rates, operative time, length of stay, ureteral stent duration, and complication rates were not statistically different between the MLP and CLP groups. Strict success rates (indicated by follow-up renal scan T½<20 min) were similar between MLP and CLP groups (89.5% vs 88.9%; P=0.95). No MLP procedures were converted to CLP or open approaches.
Conclusions:
From technical, perioperative, and outcome perspectives, transperitoneal pyeloplasty with microlaparoscopy is both safe and feasible in our hands compared with conventional laparoscopy, and results in subjectively superior cosmesis. This is the largest MLP series to date and contains, to our knowledge, the only cases described using prototype 1.9 mm instruments.
Introduction
L
Over the past decade, use of the da Vinci robotic platform (Intuitive Surgical Inc., Sunnyvale, CA) has increased exponentially and has resulted in widespread translation of laparoscopic pyeloplasty. Recently, new minimally invasive approaches, such as laparoendoscopic single-site (LESS) surgery, have been proposed and touted to potentially decrease invasiveness and improve cosmesis, but reported results vary. 3 –5 Considering the technical difficulty of pure laparoscopic LESS surgery for even the most skilled laparoscopic surgeons, the use of robotics in combination with the LESS approach has been proposed. 6 –8 While this approach may ease technical difficulty, using the robot increases cost, decreases case margin, and may necessitate a larger incision and increased use of accessory equipment such as the GelPort system (Applied Medical, Rancho Santa Margarita, CA).
In 2009, we sought an alternative approach and undertook the development of a microlaparoscopic approach using≤3 mm working instruments for the performance of adult dismembered laparoscopic pyeloplasty. The main concerns regarding microlaparoscopy and its instruments were decreased intraoperative durability of the microlaparoscopic instruments, increased skill needed to operate, and overall decreased ability to perform complex tasks, such as intracorporeal suturing. 9,10 Before 2009, microlaparoscopy had been used for pyeloplasty only in a small series of primary UPJO procedures in a pediatric population 11 and as adjunctive trocars in procedures in adults necessitating minimal-to-no specimen removal or suturing. 12 To address the feasibility and outcomes of our hybrid microlaparoscopic pyeloplasty (MLP) in adults, a single surgeon's and institutional experience with both MLP and conventional laparoscopic pyeloplasty (CLP) was retrospectively analyzed and compared.
Methods
A retrospective review of adult patients who underwent laparoscopic transperitoneal dismembered pyeloplasty performed by a single surgeon (SDH) led team from January 2009 through May 2013 was performed. All patients underwent standard preoperative evaluation with a history, physical examination, and functional/anatomical renal imaging. CLP was performed either via standard pure laparoscopic instruments or with robot assistance using camera and instrument ports ranging in size from 5 mm to 12 mm, while MLP used 1.9 mm to 3 mm (Karl Storz Inc., Tuttlingen, Germany) working instruments with a 5-mm umbilical camera port (hybrid approach) (Figs. 1, 2). All procedures included in this series and period were approached transperitoneally, and we universally performed an Andersen-Hynes dismembered pyeloplasty technique with crossing vessel transposition and pelvic reduction at the discretion of the attending surgeon.

Microlaparoscopy uses ports and instruments with diameters smaller than the most compact counterparts in conventional laparoscopy, as demonstrated by the larger 5-mm reusable laparoscopic trocar and instrument
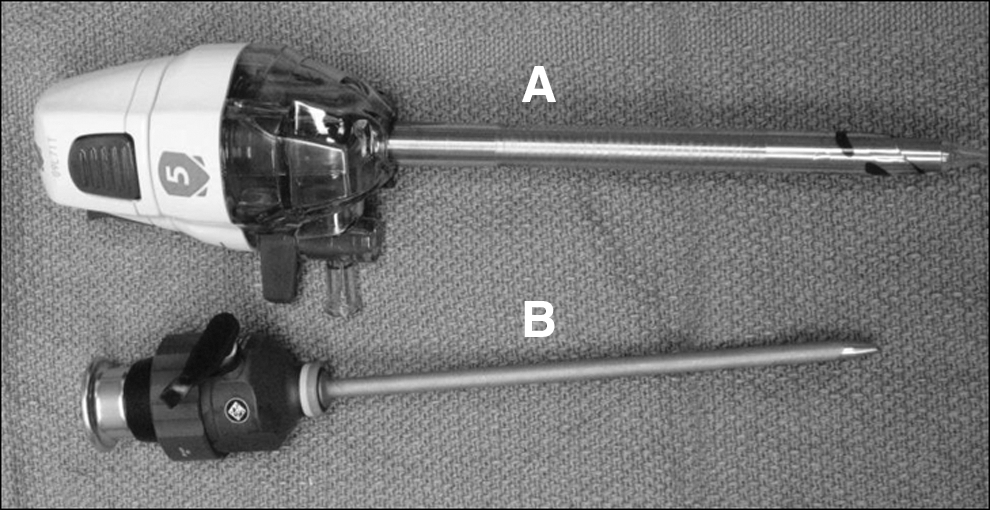
The hybrid approach to microlaparoscopic pyeloplasty uses an optical 5-mm trocar (Ethicon Endosurgery)
Our technique for patient positioning and laparoscopic pyeloplasty has been previously published and was followed in all cases other than the exclusion of initial retrograde pyelography in some patients. 13 Our technique for MLP performing initial entry and insufflation consists of visual access via an optical 5-mm trocar (Ethicon Endosurgery, Cornelia, GA) access in combination with a 0-degree, 5-mm camera through an incision within the typical concavity of the umbilicus often hidden in an umbilical skin fold. The trocar tip is tunneled slightly caudally and laterally to result in a more optimal angle of visualization. In addition, the dilating tip design, 5-mm size, and insertion angle minimize the risk of hernia, so fascial closure is not necessary.
Once insufflated, the microlaparoscopic ports (3.5 mm) are placed under direct vision. Previous versions of the trocars were short and needed securing sutures to prevent accidental extraction, while, more recently, longer trocars are available. The upper ureter and ureteropelvic junction area are dissected. The ureter is divided below the UPJO and spatulated. In some cases, 5-mm scissors were inserted through the 5-mm umbilical trocar and a 3-mm lens used through a microlaparoscopic trocar to speed division and resection of the redundant pelvis. Two 4-0 polyglactin (8 in) sutures are brought in tail first through the 5-mm trocar or the site of one of the microlaparoscopic trocars. Intracorporeal suturing and knot tying is performed using the microlaparoscopic needle holders. The stent is inserted after anastomosis and before closure of the renal pelvis after which standard drain (3 mm) placement and skin closures are performed. Stent placement confirmation and postoperative care are consistent with previously published technique and postoperative care pathway. 13
Data from these clinical interactions were collected and analyzed, which included patient age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, laterality, pre- and postoperative creatinine levels, previous UPJO treatment, pre- and postoperative diuretic renography results, operative time, estimated blood loss (EBL), presence of crossing vessel, need for transfusion, length of stay (LOS), ureteral stent duration, complications, length of follow-up, and need for re-treatment. Success was defined by postoperative diuretic renography T½ less than 20 minutes and/or resolution of preoperative symptoms. These data for MLP and CLP patients were compared using the Student t test, Pearson chi-square test, and Fisher exact test, where appropriate.
Results
From January 2009 through May 2013, 46 laparoscopic transperitoneal dismembered pyeloplasties were performed by a single surgeon (SDH). There were 27 CLP (7 performed with robot assistance) and 19 MLP patients (Table 1). The mean age was lower in MLP patients (34 vs 50 years; P=0.0003), but the sex distribution was similar (P=0.13). The mean BMI was not significantly different in the MLP group compared with the CLP group (24 vs 27; P=0.05). The distribution between groups in ASA categories I–II and III–IV were not significantly different (P=0.06). Among the CLP patients, 6 (22.2%) had previous UPJO treatment compared with 1 (5.3%) MLP patients (P=0.38). Mean preoperative creatinine level was similar between groups (1.0 vs 1.0 mg/dL; P=0.48).
Statistical significance indicated by P value <0.05.
MLP=microlaparoscopic pyeloplasty; CLP=conventional laparoscopic pyeloplasty; BMI=body mass index; ASA=American Society of Anesthesiologists.
There were more identified crossing renal vessels in the MLP group (12 vs 9; P=0.046). There was no difference between groups in operative time (197 vs 208 min; P=0.48), mean EBL (57 vs 77 mL; P=0.23), or mean LOS (1.1 vs 1.3 days; P=0.07). There were no transfusions needed in the series (Table 2).
Statistical significance indicated by P value <0.05.
There were no major complications.
Success determined by post-operative diuretic renogram demonstrating T-½ <20 minutes.
MLP=microlaparoscopic pyeloplasty; CLP=conventional laparoscopic pyeloplasty; EBL=estimated blood loss.
There was no significant difference in the overall postoperative creatinine level (0.02 vs 0.0 mg/dL; P=0.70) or change in creatinine level from preoperative values in either group (P=1.0 vs 1.0 mg/dL; 0.74). There was no difference between MLP and CLP groups for duration of indwelling ureteral stent (46 vs 46 days; P=0.91), length of follow-up (244 vs 380 days; P=0.18), or complications (P=0.28). There were six complications in the MLP group. One patient was readmitted for pain and nausea 7 weeks after surgery, but demonstrated no evidence of obstruction on imaging; in one patient, gross hematuria developed and clot urinary retention necessitating percutaneous nephrostomy drainage, but following this, postoperative renal scan T½ was 6.7 minutes. The other patients' postoperative courses were complicated by urinary tract infection (UTI) or pain managed expectantly. Two MLP patients with treatment failure underwent redo robot-assisted laparoscopic (RAL) pyeloplasty because of persistent pain and/or evidence of continued obstruction. Intermittent obstruction that could not be defined by renal scan (postoperative T½ 11 minutes) developed in one of these patients, but was consistent on imaging with an intermittent obstructive kink during renal ptosis. This patient's pain resolved after repeated pyeloplasty and renal pexing.
The CLP group had four complications, consisting of Candida urosepsis, UTI, ureteral stent-related pain, or persistent pain. No CLP patients needed repeated pyeloplasty. The difference between MLP and CLP groups in re-treatment was not significant (2 vs 0 patients; P=0.17). There were no intraoperative complications or conversions to an open approach in either group. No MLP procedures were converted to CLP or had equipment failure. Strict physiologic success rates (indicated by renal scan T½ <20 min) were similar between MLP and CLP groups (89.5% vs 88.9%; P=0.95).
Discussion
Microlaparoscopy was initially introduced in gynecology and pediatrics to further reduce the invasiveness of surgery beyond that of conventional laparoscopy. Initially, microlaparoscopy was ideally suited for use in procedures not needing incisional enlargement for specimen removal and was used in diagnostic procedures or nonextirpative surgeries, such as tubal ligation. Microlaparoscopy was initially applied in adults in urology only as an adjuvant or assistant trocar or tool rather than a primary therapeutic instrument, such as renal cyst decortication, adrenalectomy, and bladder cuff management. 14,15 Microlaparoscopic instruments for pyeloplasty were first used in the pediatric population because of the frequency of the procedure and the goal of improved postoperative cosmetic results in children. 11
To our knowledge, treatment of UPJO in adults using microlaparoscopy for pyeloplasty has been described by only one other group thus far, starting around the same period as our initial experience. Porpiglia and associates 16 described their series of 10 adult patients undergoing minilaparoscopic pyeloplasty. 16 The authors described a high rate of success with diuretic renography (although no T½ criteria were specified) and high patient satisfaction regarding postoperative scars. One patient in this series needed conversion to conventional laparoscopy secondary to bleeding. Their second study 17 was an extension of the series, including two additional patients and comparing this group with 24 patients who previously underwent CLP. 17 The perioperative outcomes were similar between these groups with no difference in operative time, EBL, postoperative pain scores, and success (with T½ specified as less than 20 min on diuretic renography). The authors describe higher patient satisfaction regarding postoperative scars in the minilaparoscopic pyeloplasty group. Overall, their studies demonstrate the benefit of miniaturized laparoscopic instruments with regard to patient satisfaction and outcomes comparable to those of conventional laparoscopy.
To date, our description of 19 adult MLP compared with 27 CLP describes the first adult cases and is the largest series of adult pyeloplasties reported. This is also the first series of its kind to include patients with secondary UPJOs. Limitations of the study include the retrospective nature and the small patient numbers, which could fail to detect a small but significant success rate difference. Also, MLP, unlike robotics, needs significant laparoscopic suturing skills and may not be universally applicable. The nondisposable tools and trocars, however, reduce disposable equipment costs and increase hospital margin compared with robotics (unpublished data). Widespread translation will likely require either increased training in laparoscopic suturing, which is unlikely in the era of robot-assisted laparoscopy, or easing the difficulty with development of a microlaparoscopic surgical robotic platform. 18
While 3-mm instruments were used in most cases, we also successfully adapted new, even smaller, prototype 1.9-mm instruments that were used in several cases. The strict physiologic success rates measured by diuretic mercaptoacetyltriglycine-3 renal scan with T½ less than 20 minutes on postoperative diuretic renography were comparable in patients who underwent MLP vs CLP. There were no intraoperative complications, and no microlaparoscopic cases necessitated conversion. We prefer the high definition quality visualization of a hybrid microlaparoscopic approach with a 5-mm laparoscopic camera and port hidden in an umbilical fold. The completion of these MLP procedures without instrument failure and corresponding good outcomes demonstrate the feasibility of microlaparoscopic instruments for complex laparoscopic tasks, such as intracorporeal suturing and knot tying. Although limited by its retrospective collection, the results of this study demonstrate the feasibility of MLP for treatment of adults with UPJO and its comparability to a conventional laparoscopic or RAL approach.
Conclusion
Both conventional laparoscopic and robot-assisted pyeloplasty have been shown to be highly successful, and new approaches, such as LESS, have sought to further reduce invasiveness. Microlaparoscopy is an alternative approach and is ideally suited for this procedure in selected patients to further reduce cosmetic impact (Fig. 3). Microlaparoscopic instruments are capable of use in adults to complete complex laparoscopic tasks, such as laparoscopic dismembered pyeloplasty. The results of this study demonstrate the safety and feasibility of MLP as well as outcomes comparable to a conventional laparoscopic approach.
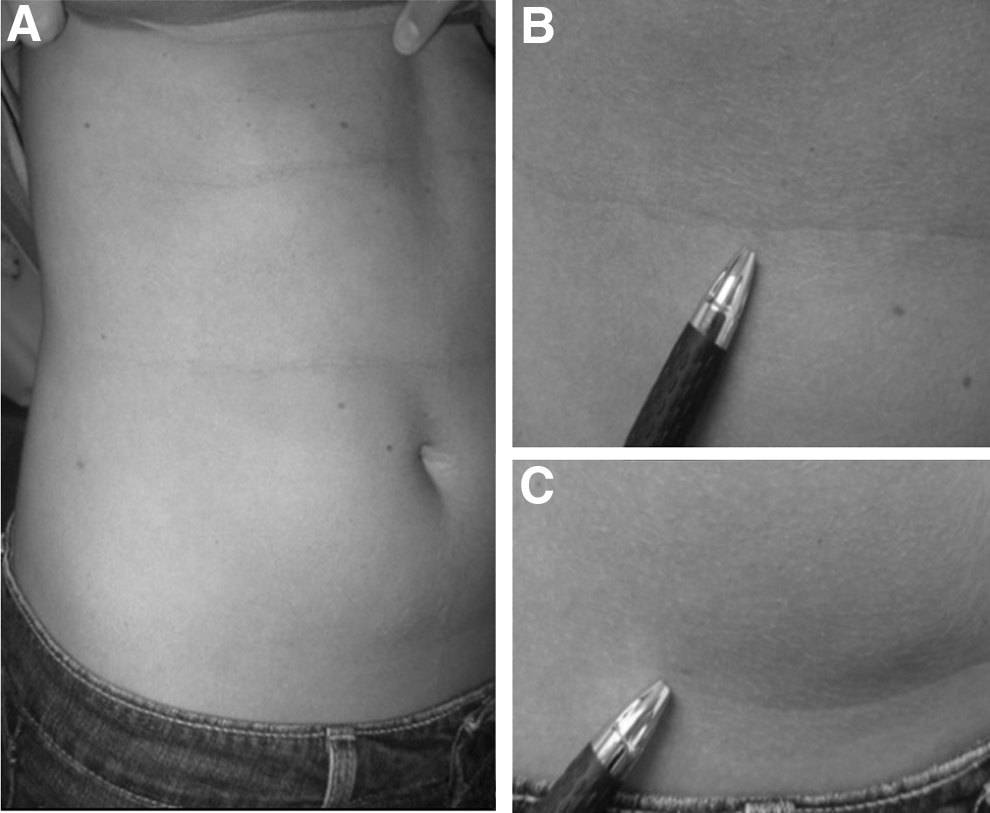
Three months after a hybrid approach microlaparoscopic pyeloplasty the skin over the operative side is almost scarless, as demonstrated by the barely visible scars corresponding to the 5-mm camera port in the umbilical fold
Disclosure Statement
No competing financial interests exist.