
Abstract
Purpose:
We sought to evaluate the relationship between hospital volume and postoperative complications following robot-assisted partial nephrectomy (RAPN) using the Nationwide Inpatient Sample.
Materials and Methods:
We identified patients undergoing RAPN between 2009 and 2011. Hospitals were divided into volume-based tertiles for each year (high, medium, low). Descriptive analyses were performed using Pearson's chi-squared and Student's t-test. Multivariable logistic regression assessed the association between hospital volume and postoperative complications, adjusting for age, gender, hospital region, type of hospital, primary payer, comorbidities, and kidney cancer.
Results:
We identified 17,583 cases from 323 hospitals, of which 112 were low volume, 112 medium volume, and 99 high volume. 13,645 (78%) cases were performed at high-volume institutions. Eleven percent of patients developed an in-hospital postoperative complication, with 15% at low-volume, 12% at medium-volume, and 10% at high-volume hospitals (p=0.071). In addition, blood transfusion was less common at high-volume hospitals (p=0.015). On multivariable logistic regression, high-volume hospitals had 42% decreased odds of postoperative in-hospital complications (95% confidence interval 0.37–0.90; p=0.016). Complications were associated with a $4500 increase in hospital costs.
Conclusions:
High-volume hospitals are associated with decreased blood transfusions and complications. With the recognition that high-volume RAPN hospitals are independently associated with improved clinical outcomes, further studies should be performed to determine the role of the hospital and surgeon volume thresholds in the performance of RAPN.
Introduction
P
Materials and Methods
Database and patients
The Nationwide Inpatient Sample (NIS) is made available through the Healthcare Cost and Utilization Project of the Agency for Healthcare Research and Quality. The NIS is a nationally representative database that provides data on 20% of in-patient hospitalizations at nonfederal hospitals each year. Forty-five states reported data to the NIS in 2011. Procedures and diagnoses are available in the form of international classification of disease (ICD)-9 codes. Discharges weights are provided by NIS to enable population estimates. 10
In a retrospective cohort analysis using the 2009 to 2011 NIS data, we identified all patients undergoing RAPN, regardless of the reason for PN. Our reason for including noncancer RAPN was that we felt that this still significantly contributes to hospital volume and thus should not be excluded. We did, however, perform a sensitivity analysis examining our outcomes among only kidney cancer cases and found no differences, which reinforced our decision to include all RAPN. Years for analysis were chosen because an ICD-9 clinical modification (CM) code was introduced in the fourth quarter of 2008 to identify RA (ICD-9 CM 17.4x). In addition, this enabled us to account, at least in part, for the initial robotic learning curve. PN was defined by ICD-9 55.4.
Outcomes and variables
The primary outcomes of interest were in-hospital complications and length of stay (LOS). In-hospital complications included urinary, vascular, cardiac, respiratory, neurologic, and digestive system complications along with seroma, hematoma, shock, hypotension, pain, venous thromboembolism, and pneumothorax. As a separate outcome, blood transfusion at any point during the hospital stay was identified. Complications were identified by ICD-9 codes (Supplementary Table S1; Supplementary Data are available online at
Statistical analysis
Descriptive analysis comparing across low-, medium-, and high-volume RAPN hospitals was performed using Pearson's chi-squared test for categorical variables and analysis of variance for continuous variables. A subanalysis was performed after separating out the highest 10% RAPN hospitals to determine whether patient outcomes were different at these hospitals compared with the low (≤33 percentile), medium (34–66 percentile), and high (67–89 percentile). Multivariable logistic regression was used to determine patient and hospital characteristics associated with developing postoperative complications. Variables included were age, gender, region, type of hospital, primary payer, CCI, kidney cancer, and hospital volume. Variables were chosen as potential confounders that are available in the NIS. Multiple linear regression evaluated the relationship between cost, complication, hospital volume, and extended LOS (>3 days represents the 75th percentile of LOS). Clustering was accounted for using generalized estimating equations. A priori significance for two-tailed t-tests was set at p<0.05. All statistical analyses were performed using Stata 12.1 (Stata Corp. LP, College Station, TX). Institutional review board exempt status was granted for conduct of this study.
Results
Three hundred twenty-three individual hospitals were identified as having performed at least one RAPN during the study period. One hundred twelve hospitals were considered low volume, 112 medium volume, and 99 high volume. A total of 17,583 patients underwent RAPN—964 at low-volume hospitals, 2975 at medium-volume hospitals, and 13,645 at high-volume hospitals (Table 1). There were no demographic or comorbidity differences between patients in each of the three hospital volume categories. High-volume hospitals were more commonly teaching hospitals and located in urban settings. Over half of the patients undergoing RAPN had private insurance. Among patients under the age of 65, 79% had private insurance billed as the primary payer.
Race unknown for 16% total.
NR=not reportable due to the limited incidence of other race; however, the number was used in calculation of the Pearson's chi-squared; SD=standard deviation.
Eleven percent of patients (n=1881) developed an in-hospital complication (Table 2). The incidence of complications was higher among patients operated upon at low-volume (15%) and medium-volume (12%) hospitals compared with high-volume (10%) hospitals (p=0.071). Blood transfusion occurred less commonly at high-volume institutions (Table 2). Median LOS was 3 days for patients at low-, medium-, and high-volume hospitals. As shown in Table 3, after adjusting for patient and hospital characteristics and accounting for clustering, high-volume hospitals were at a 42% decreased odds of developing a postoperative complication compared with low-volume hospitals (p=0.016). In addition, each point on the CCI was associated with a 31% increased odds of postoperative complication (Table 3).
IQR=interquartile range.
CI=confidence interval.
Differences in median hospital costs approached statistical significance (p=0.090) (Table 2). Median hospital costs for patients with a complication were significantly higher than for patients without a complication, regardless of hospital volume (low: $19,334 vs $13,628; medium: $19,951 vs $13,787; high: $17,701 vs $13,695; all p<0.001). On multiple linear regression when adjusting for hospital volume and extended LOS, postoperative complication was associated with a $4511 increase in hospital cost (p<0.001).
On subanalysis, there were 32 hospitals that were considered highest volume (top 10% by volume). Forty-seven percent of patients undergoing RAPN were operated upon at the highest volume hospitals (n=8348). These hospitals were concentrated in the Midwest and South, which had combined 66% of the highest volume centers (p<0.001) (Fig. 1). The incidence of blood transfusion at high-volume and highest volume hospitals was comparable (5.2% vs 4.8%). Fifteen percent of patients at low-volume, 12% at medium-volume, 11% at high-volume, and 9% at the highest volume hospitals developed a postoperative complication (p=0.109). The median (IQR) LOS for those operated upon at the highest volume centers was 2 (2–3) compared with 3 (2–4) for low-, medium-, and high-volume hospitals (p<0.001). There was no difference in median hospital costs.
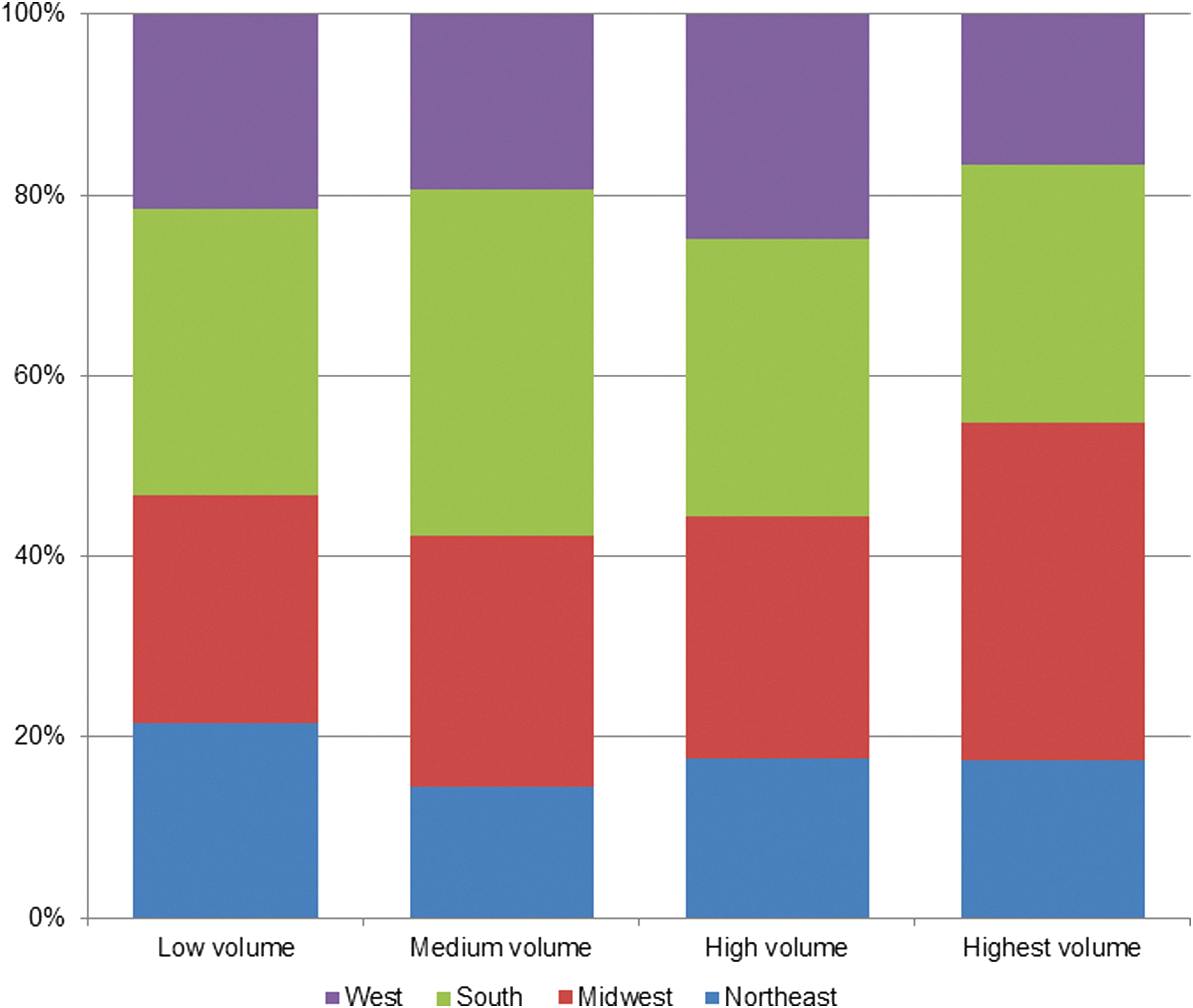
Distribution of hospitals by region within each robot-assisted partial nephrectomy case volume strata.
Discussion
Since RAPN was first reported in 2004, there has been a significant increase in the utilization of RA in the conduct of PN. 3,13 Understanding the role of hospital volume on RAPN outcomes is important in light of the significant increase in PN over the past decade and recommendations in favor of PN for the management of small renal masses. 3,14 We hypothesized that the hospital volume of RAPN would play a significant role in developing postoperative complications due to the complexity of PN. Perhaps, not surprisingly, nearly half of RAPNs in the United States are performed at the top 10% of hospitals by volume and being a high-volume RAPN hospital is independently associated with decreased risk of postoperative complications. Our findings suggest that there is significant regionalization of care to higher volume hospitals for RAPN.
The impact of hospital volume on surgical patient outcomes has been explored numerous times. 15 –21 Repeatedly, studies have found that hospitals that are high volume in specific procedures have incremental, but significant, decreases in the incidence of postoperative complications and reduced hospitalization time. Hospital and surgeon volumes are used as proxies for quality of care based on the notion that repetition leads to decreased errors. 18,20 While hospital volume has been advocated as a potential quality indicator, its utility and potential shortcomings have been debated. 22 One potential shortcoming is that recent graduates will likely have lower case volumes than well-established urologists, which could unintentionally create a bias against these new practitioners receiving referrals. 22 Lane et al. reported a significant increase in the proportion of small renal masses that were treated with PN at a community hospital over a 12-year period. 2 Interestingly, they found that urologists who graduated more recently were more likely to perform PN than those who graduated before 2001. Although we are unable to evaluate the years that a urologist has been in practice using the NIS, we imagine that recent graduates in community settings may be more likely to perform RAPN than their colleagues. If this is the case, then potentially higher rates of RAPN in smaller and medium-volume institutions may be seen in the coming years with associated lowered incidence of complications.
With the recognition that high-volume hospitals are associated with improved clinical outcomes, ensuring that patients have access to these hospitals becomes significant. Although we did not identify demographic or payer-based differences in patients undergoing RAPN at low-, medium-, and high-volume institutions, previous studies of open procedures have reported on disparities. 23,24 Trinh et al. examined disparities in patients undergoing uro-oncologic procedures at low-, medium-, and high-volume hospitals and reported that older patients, those with higher comorbidities, those in lower income brackets, and Medicare patients were less likely to undergo uro-oncologic surgery at high-volume hospitals. 24 Ensuring equal access to quality care must remain a priority of our healthcare system. Interestingly, we found that 79% of patients under the age of 65 were private insurance patients. This is significantly higher than the 2011 estimate that 64% of Americans between the ages of 18 and 64 had private insurance. 25 New technology is known to come at a cost premium that can influence which patients receive it based on payer type. It has been suggested that RAPN may replace open PN as the standard of care for small renal masses 26 or at the very least alter the patient population that is offered a minimally invasive option for PN may expand. 3,14 Should this occur, it is important to ensure that all patients have equal access to the standard of care treatment modality, regardless of the primary paying modality.
Postoperative complications following RAPN were recently reported as 13% in a multi-institutional cohort of RAPN patients. 5 Five percent of patients required perioperative blood transfusion. The findings of Tanagho et al. are based on 886 patients managed at five hospitals, all of which would likely fall within our high-volume institution category. 5 Their findings echo our own, in which we report an 11% postoperative complication rate, varying between 10% at high-volume institutions to 15% at low-volume institutions, with a 5.7% overall blood transfusion rate, similarly varying between 5% and 9% by hospital volume.
For the past decade, the Leapfrog Group, which is a coalition of public and private purchasers, and the Centers of Excellence program have advocated for management of select procedures at higher volume or quality benchmarked institutions, respectively. 18,27,28 Although regionalization of care for other surgical and urologic procedures, such as prostatectomy, would not be easily conceivable due to the high number performed, 21,29,30 perhaps, in the setting of a complex reconstructive procedure such as RAPN, it should be considered. We report that less than a quarter of RAPNs were performed at low- and medium-volume hospitals and that nearly half occurred at the highest 10% volume hospitals. Furthermore, high-volume hospitals were independently associated with decreased postoperative complications. Studies examining both hospital and surgeon volume have found that each is associated with reduced complications. 18,20 This is reflective of the critical complementary roles that both surgeon and ancillary staff play in the care of surgical patients. Regardless of a surgeon being well trained in the performance of a complex reconstructive surgery, if the ancillary staff is unable to provide necessary, specialized postoperative care, then complications will occur more commonly. Based on the findings of our study, regionalization of care exists for RAPN.
Moving forward in the current healthcare climate, it is unclear whether continued regionalization of care will, or should, continue. Especially with more urologists being trained in performing RAPN, potential surgeon competence will enable an expansion and increase in the number of RAPNs being performed at previously low-volume centers. Although high-volume centers were associated with significantly fewer complications, the absolute difference between high- and low-volume centers was relatively small (5%), which leads us to believe that RAPN could be performed safely at lower volume centers. This is particularly important for the delivery of care to the underserved and disadvantaged populations, who have previously been shown to receive disparate surgical care, 23,24 so long as the quality of care is shown to be appropriate.
Although we report a lower incidence of complications at high- vs low- volume institutions (10% vs 15%) with a significant reduction of odds of a complication after adjusting for hospital and patient factors, these results should be interpreted and used to influence policy with caution. By virtue of using an administrative database, we are unable to assess characteristics specific to the urologist such as years in practice or extent of robotics training. Also, we are unable to determine the severity (Clavien grade) of complications and the resultant morbidity to the patient; however, the fact that complications were associated with a $4500 increase in hospital costs leads us to believe that the majority of these complications were significant. The cut-points for low-, medium-, and high-volume institutions were based on the cases within the database, which may or may not reflect the best definition of these distinctions. If thresholds of case volume are used to direct the dispensation of care in the future, research into what constitutes the optimal case volume and acceptable rates of complications is necessary.
Several limitations warrant discussion. Using an administrative database offers the benefit of large numbers of cases to study in a nationally representative sample. However, it is subject to potential limitations, including miscoding and a lack of pathologic and intraoperative data, which could result in uncontrolled for biases. Furthermore, NIS relies on using ICD-9 codes to identify both diagnoses and procedures. RA is identified using a secondary ICD-9 code, so some cases might have been missed. It is, additionally, important to note that pathologic details such as tumor size, tumor histology, and tumor characteristics are not collected by NIS. Using in-hospital complications is a potentially biased outcome, as we are unable to identify patients who develop fistulas or hematomas and require readmission. Finally, assessing volume–provider relationships is subject to biases that have been extensively described, 30 although we attempted to minimize these biases with a large sample size. Despite these limitations, this study is among the first to examine the volume–provider relationship in a robot-assisted reconstructive procedure and offers insights into the centralization of care associated with RAPN.
Conclusions
The majority of robot-assisted partial nephrectomies occur in high-volume hospitals, which are independently associated with decreased postoperative complications and had lower incidence of blood transfusion. Studies examining the specific role of surgeon volume on postoperative complications should be performed to aid in the determination of the role of hospital and surgeon volume thresholds in the performance of RAPN.
Footnotes
Disclosure Statement
No competing financial interests exist for any of the authors.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.