
Abstract
Purpose:
To determine the feasibility and develop a robotic technique for intracorporeal implantation of a biodegradable tubular scaffold seeded with adipose-sourced smooth muscle cells (Neo-Urinary-Conduit) that, when implanted as a conduit for urinary diversion, facilitates regeneration of native-like neourinary tissue.
Materials and Methods:
Robotic NUC implantation was performed in two fresh male cadavers. The greater omentum was widely detached from the greater curvature of the stomach, in preparation for final wrapping of the conduit. Bilateral ureters were mobilized for implantation. The NUC, with two precreated ureteral openings, was inserted into the abdomen. Bilateral, stented uretero-NUC anastomoses were created. The NUC was circumferentially wrapped with the predissected omentum, exteriorized through the abdominal wall, and maturated.
Results:
Both procedures were successfully completed intracorporeally. Operative time for NUC implantation was 90 and 100 minutes, respectively. Examination of gross anatomy showed no injury to other organs. There was no omental kinking, rotation, eversion, or stripping from the NUC. Bilateral stents were confirmed to be in situ with the proximal coil in the kidney. Uretero-NUC anastomoses and omentum were tension free. The entire NUC, including its distal edge and posterior aspect, was circumferentially wrapped 360 degrees.
Conclusion:
We demonstrated the feasibility and developed a robotic technique for intracorporeal implantation of a biodegradable regenerative urinary conduit. This study serves as the foundation for the robotic surgical technique before the clinical application.
Introduction
I
Tissue engineering has provided a potential alternative to bowel for reconstructive urinary tract procedures such as augmentation cystoplasty.
4
Preclinical and initial clinical studies have demonstrated regeneration of native-like neourinary tissue within biodegradable tubular scaffolds seeded with adipose-sourced smooth muscle cells (SMCs),
5
and phase 1 clinical trials are under way to evaluate open surgical implantation of a regenerative urinary conduit in humans with encouraging preliminary outcomes (
Before using the minimally invasive approach to implant this regenerative urinary conduit on patients, the feasibility of the technique must be investigated. Here, we determine the feasibility and demonstrate a completely intracorporeal robotic technique for implantation of a biodegradable regenerative urinary conduit.
Materials and Methods
Regenerative urinary conduit
The Neo-Urinary Conduit™ (NUC, Tengion®, Winston-Salem, NC) is a hollow tubular conduit, 3 cm in diameter and 25 cm in length. This biodegradable tubular scaffold is composed of polyglycolic acid (PGA) coated with poly-dl-lactide-co-glycolide (PLGA) and seeded with the patient's own adipose-sourced SMCs. These SMCs, obtained from an incisional biopsy from the same patient's own anterior abdominal subcutaneous fat approximately 1 month before, are expanded in vitro in the laboratory, as described previously. 5 The entire seeding process takes 4 weeks, after which the NUC is deemed ready for implantation into the patient.
Surgical technique
Our robotic technique was developed in two fresh, adult human cadavers. The cadaver is placed in the supine decubitus position with abducted thighs, pneumo-peritoneum is obtained, six transperitoneal ports are placed in a manner identical to clinical robotic radical cystectomy, the robot is positioned between the patient's legs, and the 30-degree robotic lens is used throughout the entire procedure (Fig. 1).
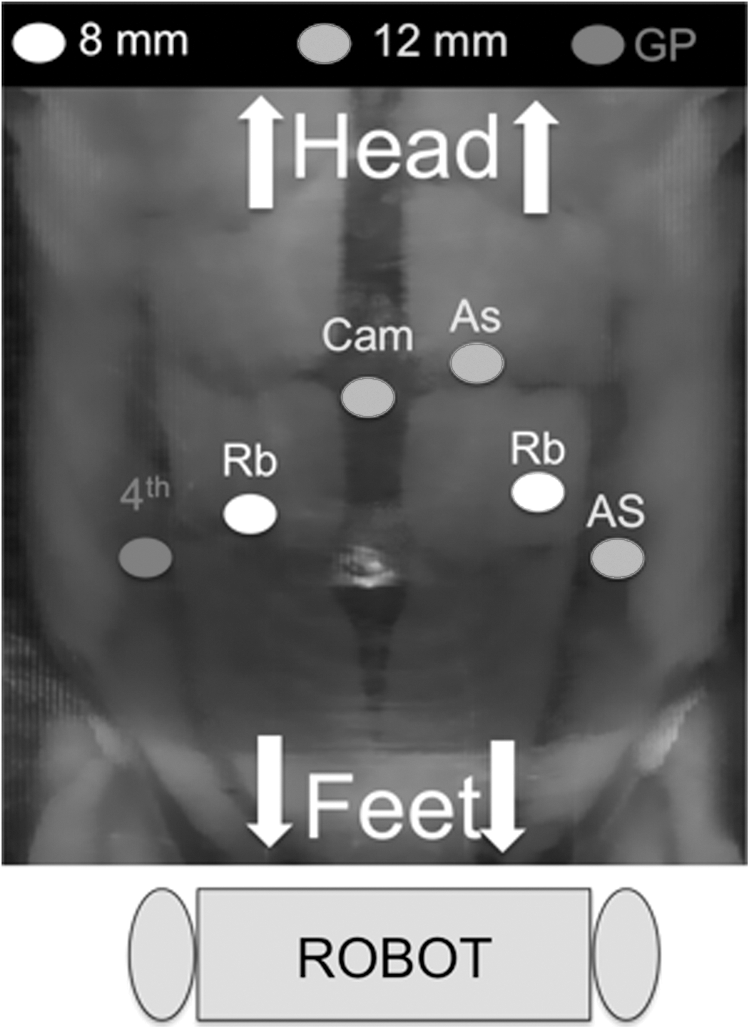
Port placement. Six ports are transperitoneally placed in a similar fashion as for clinical radical cystectomy. AS=assistant port; GP=GelPort®; Rb=robotic arm; Cam=camera; 4th=fourth robotic arm.
At the start of the procedure, robotic work is directed towardsthe head-end of the cadaver. The greater omentum is identified and placed on caudal stretch to assess its length and range. To increase its length, the greater omentum is widely detached from its most cephalic attachments along the greater curvature of the stomach, carefully preserving its feeding vasculature (Fig. 2). Omental detachment is achieved between nonabsorbable clips to ensure no bleeding or intraomental hematoma occurs. Adequate omental length is deemed to have been prepared when the broad tip of omentum readily reaches the pubic symphysis in the pelvis in a tension-free manner. This mobilized omental length is adequate to permit complete 360-degree wrapping of the NUC.

Robotic work is now redirected toward the pelvis, and RC and extended lymphadenectomy are completed. Both ureters are athermally mobilized with generous mesoureter; the left ureter is brought to the right side of the abdomen posterior to the descending mesocolon. The ureteral edges are spatulated and prepared for bilateral Bricker-type ureteral-NUC anastomosis.
Before inserting the NUC into the abdomen, it is pr-prepared for implantation on the back-table. Using scissors, two oval-shaped openings are created close to the proximal end of the NUC, one for each ureteral-NUC anastomosis. Each opening is 1.5 cm in diameter, and the two openings are spaced 4 cm apart. The proximal (internal) end of the NUC is sutured closed by oversewing with 2-0 polyglactin on a CT-1 needle (Fig. 3).

Back-table preparation of the Neo-Urinary Conduit (NUC). (
The NUC is inserted into the abdomen, with its proximal end first, through the preselected location of the ultimate NUC stoma site. Similar to the standard open technique for creating an ileal conduit stoma, a button of skin and subcutaneous tissue is excised, the underlying fascia is incised, and a generous full-thickness opening that easily admits two fingers is created; the skin opening for the NUC is created slightly larger than that for a traditional ileal conduit. A GelPort® (Applied Medical, Rancho Santa Margarita, CA) is now secured at this location and pneumoperitoneum is reestablished.
Bilateral, individual, stented uretero-NUC anastomoses are performed in standard fashion; the right ureter is anastomosed first. Interrupted stitches (4-0 polyglactin suture, RB-1 cutting needle) are used so as to not compromise ureteral vascularity. Before completing the anterior wall of the anastomosis, a 7F 26-cm Double-J® stent is inserted into the ureter over a glide wire through an appropriately placed 2-mm MiniPort® (MiniPort™ Auto-Suture™; Norwalk, CT); the proximal coil of the stent is positioned within the renal pelvis, and the distal coil is inserted into the NUC. The ureteral anastomosis is then completed (Fig. 4).
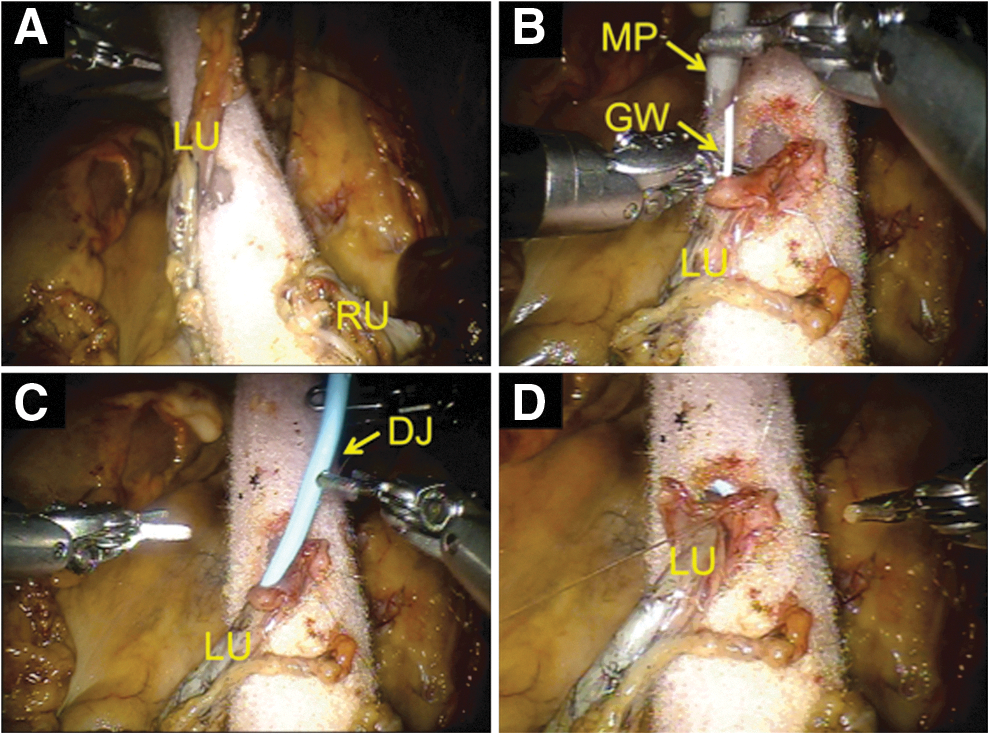
Bilateral ureteral-Neo-Urinary Conduit (NUC) anastomoses.
The NUC is now completely and circumferentially wrapped in its entirety with omentum; wrapping is performed from proximal-to-distal end. At approximately 10 to 12 sites, the omentum is circumferentially suture-tacked to the NUC with 4-0 polyglactin stitches. The goal herein is to not leave absolutely any part of the NUC surface uncovered by omentum. This is critically important to promote maximal neovascularization of the NUC. At the distal (external) end of the NUC, omentum coverage is secured with only one to two stitches, with their suture-tails left long (Fig. 5).

Omental wrapping the Neo-Urinary Conduit (NUC). To maximize its neovascularization, the NUC must be completely wrapped circumferentially over its entire outer surface with omentum (OM). (
Robotic visualization confirms that the NUC easily reaches the abdominal wall, without any omental kinking, rotation, or tension; also, care is taken to reconfirm that the NUC is indeed completely wrapped by omentum, without any omental eversion. Both uretero-NUC anastomoses are confirmed to be well oriented and tension free. The NUC is now exteriorized through the abdominal wall after removing the GelPort from the stoma location; again, extreme care is taken to ensure that no omental stripping from the NUC occurs during passage of the NUC through the abdominal wall tunnel. A Jackson-Pratt drain is inserted into the abdomen through a port site, and the robot is undocked.
The NUC stoma is now matured. The distal-most omental stitches (with the long tails) are removed, the omentum is peeled back, and the distal end of the NUC is appropriately exteriorized, shortened, and tailored. The freshened distal end of the NUC is circumferentially covered by omental invagination into the NUC lumen. The NUC is secured to the skin with interrupted 3-0 polyglactin stitches. A 24F silicone tube is indwelled into the NUC (Fig. 6). Port sites are closed, and the procedure is completed.
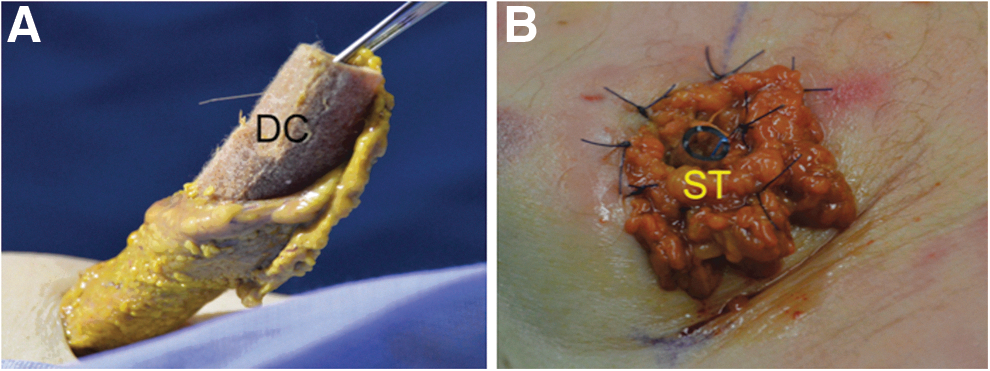
Neo-Urinary Conduit (NUC) maturation. (
Results
Both NUC implantation procedures were successfully completed robotically with operative times of 90 and 100 minutes, respectively. Cadaveric body mass indices were 26 and 28 kg/m2, respectively. Gross examination showed no injury to other organs. There was no omental kinking or rotation, and the omentum was not everted or stripped from the conduit within the abdominal tunnel. The stents were in place, with the upper coil in the renal pelvis and the distal coil in the NUC. Bilateral uretero-NUC anastomoses and omentum were tension free. The entire surface of the NUC, including its distal (external) edge and posterior aspect, was completely wrapped with omentum (Fig. 7).
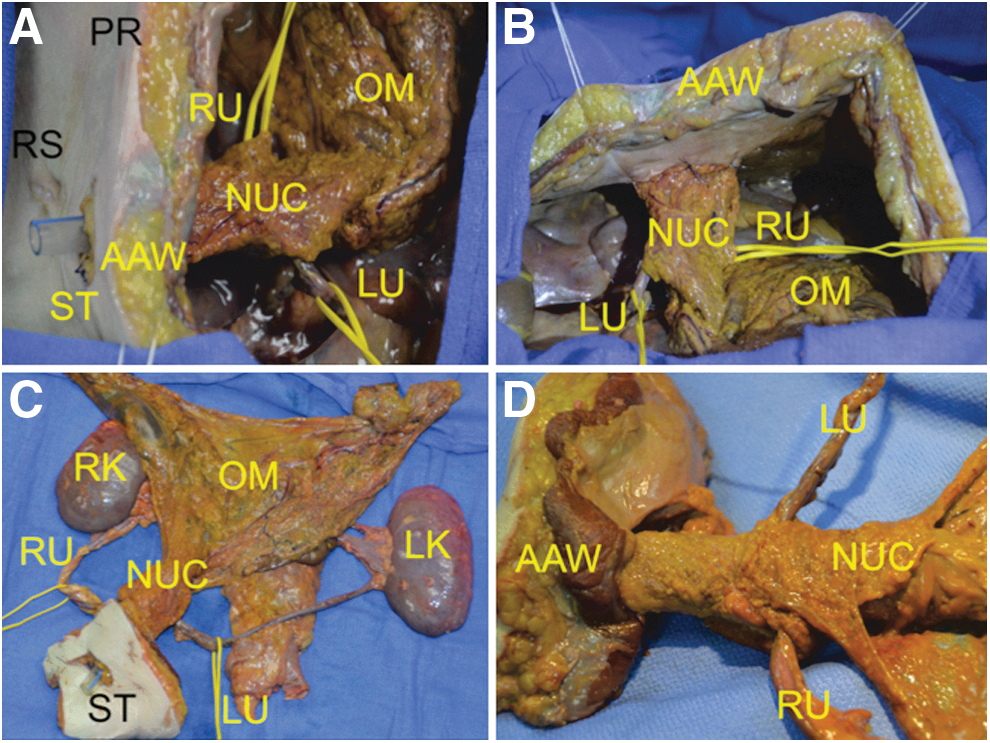
Gross anatomy. (
Discussion
Radical cystectomy with urinary diversion is a major surgical procedure that is associated with high postoperative complication rates ranging from 41% to 81%, most of which are diversion-related. 2,3,6 –8 These complications are typically infectious (12%–32%), gastrointestinal (10%–27%), or metabolic (0%-12%), and they likely stem from enteric interposition within the urinary tract leading to urine absorption, metabolic/electrolyte imbalance, contamination/infection and excessive mucus production (Table 1). 2,3,6 –9 Robotic RC and intracorporeal ileal conduit are associated with early and late complication rates of 63% and 81%, respectively. 6 Because it eliminates use of bowel, NUC has the potential to diminish bowel-related complications of RC. Further, since the regenerated neourothelial tissue within the NUC is similar to native urothelium, it provides a sterile, nonabsorptive environment, without any mucus secretion. 4,5
Neobladder n=29 (28%), Indiana pouch n=23 (22%).
Neobladder n=26 (31%) (28%), Indiana pouch n=10 (12%).
Continent cutaneous UD n=48 (25%), Orthotopic neobladder n=86 (44%).
Obstruction, leaking or enteric fistula.
11 (1%) patients were re-operated due to small bowel obstruction (n=8) or bowel injury (n=3).
RARC=Robot-assisted radical cystectomy; ECUD=extracorporeal urinary diversion; ICUD=intracorporeal urinary diversion; UD=urinary diversion; NA=not available.
The NUC used in this study is a synthetic biodegradable tubular scaffold, with shape and dimensions similar to an ileal conduit and seeded with the patient's own adipose-sourced SMCs. Importantly for bladder cancer patients, these SMCs are not derived from the patient's native urinary tract, thus allaying concerns about the risk of isolating, expanding, or seeding cancerous cells onto the construct. As such, the development of an engineered tissue that uses SMCs derived from a nonurothelial source was sine qua non for ensuring oncologic safety of the construct. 5 Important also is that bladder cancer patients requiring RC undergo surgery in a timely manner so as to not jeopardize oncologic outcomes. 10 As such, the 4 weeks between harvesting the patient's abdominal adipose tissue to completion of SMC integration into the final construct scaffold is an acceptable period while the patient is being prepared for RC. 10
Jayo and associates 11 compared functional and histologic outcomes of unseeded biodegradable scaffolds (scaffolds) versus scaffolds seeded with autologous urothelial cells and SMCs (constructs) implanted in a canine model of augmentation cystoplasty. The constructs were urodynamically compliant similar to baseline within 4 months and histologically demonstrated complete regeneration of bladder wall, including mucosa and muscular components, within 9 months. Conversely, the unseeded scaffolds were unable to regenerate functional outcomes and provided only reparative healing (repair) with incomplete tissue development at 9 months. 11
In a recent preclinical study, Basu and colleagues 5 could isolate SMCs from adipose tissue and peripheral blood that were functionally and phenotypically indistinguishable from bladder-derived SMCs. 5 They compared tubular scaffolds seeded with either nonbladder derived (adipose or blood tissue) or bladder-derived SMCs after implantation (wrapped with peritoneum) in a survival porcine cystectomy model. After a recovery period of 84 days, the animals were euthanized. On histologic examination, constructs seeded with adipose and peripheral blood tissue were able to regenerate de novo urinary-like neotissue identical to native bladder. These findings have implications for translation of preclinical studies into clinical practice. 5
Initial results of a Phase 1 clinical study evaluating open surgical implantation of bioengineered regenerative NUC (same NUC as used in our cadaver study) are encouraging (Timothy A. Bertam—personal communication). Seven patients underwent open RC followed by open surgical NUC implantation. Histologic analysis of four explanted NUCs showed early evidence of urinary tissue 7weeks postimplantation, and mature urinary tissue with urothelium and tunica muscularis layer fully developed 10 months postimplantation.
Atala and coworkers 4 performed open bladder augmentation in seven patients with myelomeningocele using bladder-shaped scaffold seeded with urothelial and muscle cells. Over a mean follow-up of 46 months (range 22–61), the engineered bladder showed satisfactory functional outcomes with adequate structural architecture and phenotype on histologic examination. 4 Furthermore, the patients experienced early return of postoperative bowel function, without any metabolic consequences, stone formation, or mucus production. 4
Given the above-mentioned improvement in patient outcomes, we hypothesized that, if the essential technical aspects of this procedure could be rigorously replicated minimally invasively, robotic surgery may result in further reduction of morbidity. As such, before conducting a clinical trial on patients, we developed an intracorporeal robotic technique of NUC implantation in the fresh human cadaver model. We were readily able to widely mobilize the omentum while preserving its vascularization. Equally, we were able to completely cover the NUC with omentum over its entire surface. All this could be achieved with standard port placements and robot positioning as is typical during clinical RC.
Omental wrapping is deemed essential to optimize vascular supply to the cultured cells in the scaffold that may impact the remodeling/regeneration process of the NUC. Animal and clinical studies have shown that complete omental coverage of the scaffold provides superior neovascularization and long-term histological outcomes. 4,12 Using robotic techniques, adequate dissection of the omental flap was achieved readily, enough to achieve full coverage of the NUC without tension or kinking, as observed intraoperatively and confirmed on necropsy. Excess omentum was tailored, invaginated, and sutured to the NUC to ensure coverage of the outer (external) edge of the NUC. If done via an open surgical technique, proximal enlargement of midline abdominal incision would be necessary to achieve omental mobilization to this degree 4 ; this was completely avoided robotically.
Bilateral uretero-NUC stented anastomoses were readily feasible robotically. In so doing, we intended to provide two separate sources of native urothelial cell ingrowth and urine entry into the NUC, which may facilitate neotissue regeneration. Also, this minimizes any chance of simultaneous bilateral ureteral-NUC anastomotic stenosis.
The main shortcoming of our study is that we did not use a live model; therefore, postoperative complications and tissue regeneration could not be evaluated. Our cadaver study is the necessary, prudent first step, however, to assess feasibility before eventual clinical application. Taken as a whole, the available preclinical data, the emerging Phase 1 open surgical clinical data, our cadaveric technique herein demonstrated, and our current routine performance of robotic RC and intracorporeal diversion surgery, the robotic intracorporeal NUC implantation could become a clinical reality in the not too distant future.
Conclusion
We developed a robotic technique for intracorporeal implantation of the neourinary conduit in the fresh human cadaver model. Eliminating use of bowel during urinary diversion coupled with intracorporeal robotic techniques may decrease morbidity for patients undergoing radical cystectomy for bladder cancer. This study serves as the foundation for the robotic surgical technique before clinical application.
Footnotes
Acknowledgment
Tengion® provided the Neo-Urinary-Conduit™ (NUC) free of cost for the purposes of this study.
Disclosure Statement
Inderbir S. Gill is a paid consultant for Hansen Medical and EDAP. Osamu Ukimura is an advisory board member to SonaCare Medical LLC. For the remaining authors, no competing financial interests exist. Mihir M. Desai is a paid consultant for Hansen Medical and Baxter. Monish Aron received honoraria from Intuitive Surgical in 2013.