
Abstract
Objectives:
To present time-efficiency data during our initial experience with intracorporeal urinary diversion and technical tips that may shorten operative time early in the learning curve.
Patients and Methods:
Data were analyzed in the initial 37 consecutive patients undergoing robotic radical cystectomy and intracorporeal urinary diversion in whom detailed stepwise operative time data were available. Median age was 65 years and median body mass index was 27. Neoadjuvant chemotherapy was administered in 6 patients and 11 patients had clinical evidence of T3 or lymph node-positive disease. Each component of the operation was subdivided into specific steps and operative time for each step was prospectively recorded. Peri-operative and follow-up data up to 90 days and final pathological data were recorded.
Results:
All procedures were completed intracorporeally and robotically without need for conversion to open surgery or extracorporeal diversion. Median total operative time was 387 vs 386 minutes (p=0.2) and median total console time was 361 vs 295 minutes (p<0.007) for orthotopic neobladder and ileal conduit, respectively. Median time for radical cystectomy was 77 minutes, extended pelvic lymph node dissection was 63 minutes, and diversion was 111 minutes (ileal conduit 92 minutes and orthotopic neobladder 124 minutes). Median estimated blood loss was 250 mL, and median hospital stay was 9 days. High grade (Clavien grade 3–5) complications at 30 and 90 days follow-up were recorded in 6 (16%) and 9 (24%) patients, respectively. Over a median follow-up of 16 months, 12 (32%) patients experienced disease recurrence and 9 (24%) died from bladder cancer. These correspond to 1-year recurrence-free and overall survival of 64% and 70%, respectively.
Conclusions:
Intracorporeal urinary diversion following robotic radical cystectomy can be safely performed and reproducible in a time-efficient manner even during the early learning curve.
Introduction
R
We recently reported our intracorporeal technique that exactly duplicates the open ileal conduit and orthotopic ileal neobladder as performed at our institution. 3 We standardized each step of this complex procedure with the aim of making the entire intracoporeal technique time efficient in a reproducible fashion. In this study, we report the detailed technical nuances aimed at achieving time efficiency in the initial 37 patients undergoing robotic intracorporeal urinary diversion while exactly duplicating established open surgical principles of urinary diversion.
Patients and Methods
Robotic radical cystectomy with intracorporeal urinary diversion was performed in 103 patients with bladder cancer between July 2011 and October 2013 and entered prospectively into our Institutional Review Board approved database. All procedures were performed by the same surgical team using the same technique. From this cohort, data were further analyzed in the first 37 consecutive patients undergoing intracorporeal urinary diversion between March 2011 and July 2012 in whom detailed procedure time data were prospectively recorded for the individual steps of the operation. Since we instituted our intracorporeal program, all patients undergoing robotic cystectomy undergo an intracorporeal diversion. Detailed breakdown of individual steps were either prospectively recorded or retrospectively ascertained from reviewing full-length video recording of the procedure. Patients were seen at weekly intervals for the first 30 days to manage drains and catheters and assess biochemistry and nutritional status. Oncologic follow-up was based on pathologic stage.
Our technique of robotic radical cystectomy, extended pelvic lymph node dissection (PLND) and intracorporeal urinary diversion duplicates the open technique has been described in detail earlier. 3 The proximal extent of PLND was up to the aortic bifurcation (extended) or inferior mesenteric artery (super-extended) based on individual clinical parameters such as age, co-existing vascular disease, and clinical stage. Several technical tricks were employed to our basic technique with the aim of improving time efficiency and are summarized in Table 1. Demographic, peri-operative, and 90-day postoperative data were analyzed. Complications were graded according to Clavien classification. 5
Bowel measurement was performed using a Penrose drain with markings made in ink or a premeasured 11 cm suture. The suture is easier to grasp along the bowel compared to the drain and is now our preferred method.
Color-coded stay-sutures help keep the transected bowel ends and various segments of the ileal loop properly oriented. Dyed sutures are placed on the mesenteric side of each of the two bowel end that is to be re-anastomosed. The stay sutures not only keep proper orientation but also help manipulate the bowel loops over the stapler jaws during anastomosis. Undyed stay sutures are placed at 11, 22, 33, and 44 cm of the isolated bowel. The 11 cm stitch marks the site of the urethroileal anastomosis, the 0 and 22 cm join to form the crossfolding and 44 cm marks the start of the afferent limb.
A 2 mm MiniSite port (Covidien) is placed through the right iliac fossa to help direct the hydrophilic wire and 6×28 cm Double-J stent in an atraumatic fashion. The 2 mm port is inserted completely such that its tip lies just at the spatulated ureter thereby minimizing looping of the wire and stent intra-abdominally. Passing the port in the RIF orients the shaft in the correct direction.
IC=ileal conduit; PLND=pelvic lymph node dissection.
Statistical software package SAS, Version 9.3 (SAS Institute, Inc., Cary, NC) was applied to all the analyses in this study. Pearson's chi-square or Fisher's exact test were used to examine the association between categorical demographic and clinical variables. Kruskal–Wallis test was used to test the differences in not normally distributed continuous variables between groups or subgroups. Two clinical outcomes, that is, overall survival and recurrence-free survival were analyzed in this study. Time to overall survival was calculated from the date of surgery to the date of death (death from all causes), or to the date of last follow-up if patient was still alive at the last follow-up. Recurrence-free survival was calculated from the date of surgery to the date of first documented clinical recurrence or to the date of death or to the date of last follow-up if patient did not experience a recurrence. Kaplan–Meier plots were used to estimate the probabilities of overall survival and recurrence-free survival for every year since surgery. The log-rank tests were used to compare the differences of survival and recurrence in subgroups. All p-values reported are two-sided and p<0.05 is considered statistically significant.
Results
All 37 patients in the present study underwent robotic radical cystectomy followed by either intracorporeal ileal conduit (n=19) or orthotopic ileal neobladder (n=18). Median age was 65 years, there were 29 (78%) men, and mean body mass index was 27 kg/m2 (Table 2). Clinical staging revealed T3 or greater or N1–3 disease in 11 (30%) patients of whom 6 (16%) had neoadjuvant chemotherapy. Twelve (32%) patients had previous abdominal surgery. All procedures were completed intracorporeally without need for conversion to open surgery. Peri-operative data are detailed in Table 3. Median estimated blood loss was 250 mL for the entire cohort. Median total operative time was 386 minutes (286–597 minutes) for ileal conduit and 387 minutes (313–778 minutes) for the orthotopic neobladder cohort (Table 4). Median total console time was 295 minutes (195–423 minutes) and 361 minutes (283–560 minutes) for the ileal conduit and neobladder groups, respectively. Median time for radical cystectomy was 77 minutes (48–182 minutes), extended PLND was 63 minutes (31–150 minutes), intracorporeal ileal conduit was 92 minutes (55–160 minutes), and intracorporeal neobladder was 124 minutes (97–327 minutes) (Table 4).
ASA=American Society of Anesthesiologists; BMI=body mass index; TCC=transitional cell carcinoma; TURBT=transurethral resection of bladder tumor.
EBL=estimated blood loss; IMA=inferior mesenterica artery; PO=per oral.
Tables 5 and 6 illustrates the impact of learning curve on operative time. When comparing the first 9 to the last 10 cases in the ileal conduit cohort there was a significant reduction in total console time (330 vs 269 minutes, p=0.04), and time to perform ureteral anastomosis (95 vs 50 minutes, p=0.02). In the neobladder group the overall console time was similar (360 vs 362 minutes, p=0.9) but the time for cystectomy was shorter (77 vs 60 minutes, p=0.05) when comparing the first nine and last nine patients, respectively. In the neobladder cohort, 10 patients had a console time of under 6 hours, 5 patients between 6 and 8 hours, and 3 patients between 8 and 10 hours.
Final pathology showed positive surgical margins in two patients and the median lymph node yield was 35 (9–79) (Table 7). Overall, 30- and 90-day low-grade complications were recorded in 20 (54%) and 21 (57%) patients; and high-grade complications were recorded in 6 (16%) and 9 (24%) patients, respectively, and they are detailed in Tables 8 and 9. Over a median follow-up of 16 months (3–36 months), 1 patient (3%) had local recurrence and 11 patients (30%) had metastatic disease (Table 10). The 1-year disease-free survival was 64% and 1-year overall survival was 70%.
Difference between extended and super-extended nodes yield was significant, p=0.0005.
CIS=carcinoma in situ; NB=neobladder.
There is no statistically significant difference between the ileal conduit or neobladder groups within 30 or 90 days complications distribution or rate.
p=0.388.
p=0.843, respectively.
Discussion
A major stumbling block to the wider adoption of intracorporeal diversion primarily relates to concerns about prolonged operative times, especially in the early learning curve. This concern is even greater in patients undergoing orthotopic diversions. Longer anesthesia times may adversely impact peri-operative morbidity and increase operative room cost; the latter may be an important issue in the current health care environment where cost containment and optimization of resources is becoming increasingly important. Thus, for urinary diversion, especially orthotopic neobladder to be performed intracorporeally, the technique must be consistently time efficient and reproducible even in the early learning curve.
We employed a gradual stepwise transition to routinely performing intracorporeal urinary diversion at our institution. The robotic intracorporeal program was initiated only when we were confident that the extirpative component was being performed efficiently on a consistent basis. We initially focused on performing intracorporeal ileal conduit to gain experience with and standardize the technical aspects of robotic bowel isolation and anastomosis and uretereral reimplantation. Once we felt comfortable with ileal conduit diversion, we extended the robotic approach to orthotopic neobladders. After developing the initial technique of intracorporeal ileal conduit and orthotopic neobladder at our institution, we partnered with institutions in China where we performed 12 cases in a single week to further consolidate and standardize the technique. Even in our very initial experience, the overall mean console time was 295 and 361 minutes for intracorporeal ileal conduit and neobladder, respectively. We found a reduction in overall console time in the ileal conduit group and time to cystectomy in the orthotopic neobladder group with experience. Ongoing refinements in technique and the addition of new surgeons including trainees make accurate assessment of improvement in time efficiency difficult. However, when looking at the subset of patients performed in China where all steps were performed by two surgeons (Mihir M. Desai and Inderbir Singh Gill, Fig. 1) there was a significant reduction in operative time. Collins et al. reported the impact of learning curve on time efficiency for an individual surgeon and showed a significant reduction in operative time. 6
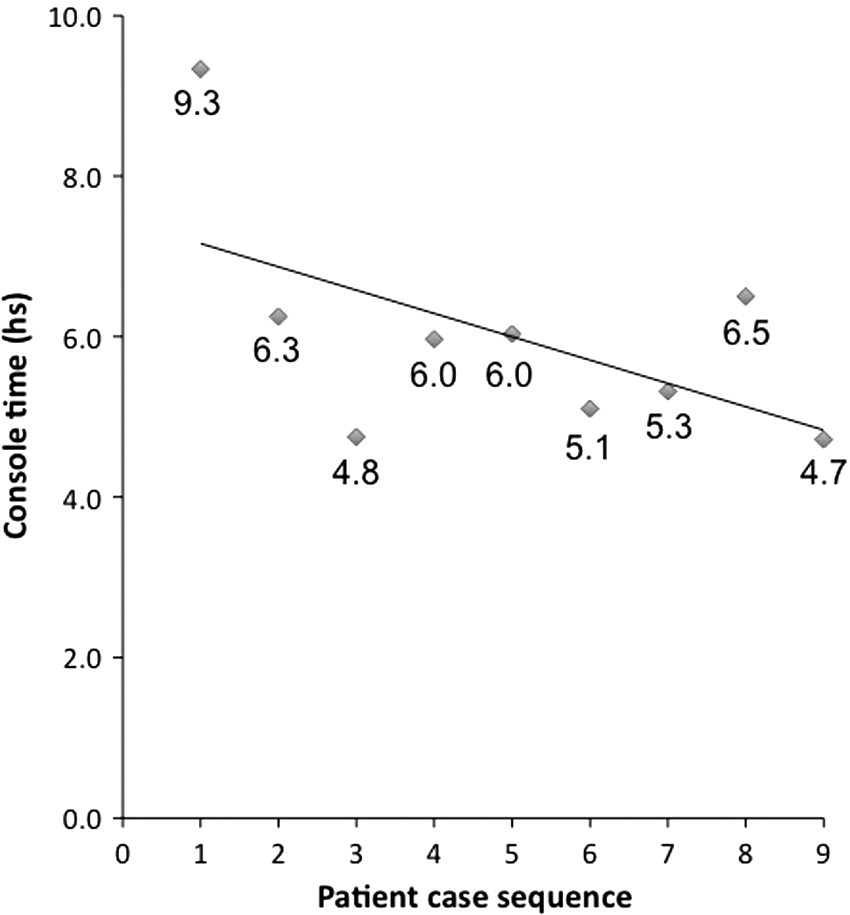
Shows a graph of trend of console time in nine orthotopic neobladders performed in China. All steps were completed by either of two attending surgeons (Mihir M. Desai and Inderbir Singh Gill).
Our approach to achieving time efficiency of intracorporeal orthotopic neobladders was to standardize each step of the procedure without altering the bowel dimensions and spherical pouch configuration of the Studer neobladder as is performed open surgically at our institution. 3 We broke down the procedure into individual steps and carefully examined time taken to complete each step thereby identifying technical modifications that could potentially improve efficiency. Technical nuances during this early experience that helped improve time efficiency of intracorporeal orthotopic diversion are detailed in Table 1. Accurate measurement of the stretched bowel is very important. If the bowel is not adequately stretched during measurement, it may lead to a significantly longer segment being isolated and a resultant longer suturing time in addition to increasing pouch capacity. Disorientation of the transected ends of the bowel during isolation and reanastomisis can significantly delay the procedure as it can take a long time to reorient the correct configuration of bowel segments. The use of color-coded stay sutures is very helpful in constantly maintaining orientation of the various transected segments of bowel that enables efficient bowel isolation and anastomosis. Stay sutures also help maintain orientation of the segments of isolated loop that will be used to construct a neobladder thus ensuring a smooth flow of the diversion.
Urethro-ileal anastomosis was the step that was most likely to have variability in operative time and accounted for three of the cases with the longest operative time in the present study. Patients with a short mesentery may have significant problems with the posterior plate reaching the urethra as is also evidenced during open surgery. We have employed several measures to try and minimize difficulty in bringing the ileum to the urethra and thereby facilitate a tension-free anastomosis. First and most important, we identify the most mobile loop of terminal ileum that is likely to reach the urethra and mark it as the site for future urethral anastomosis; this point then acts as reference to mark out the 59 cm ileal loop to be isolated for constructing the neobladder. Second, we detubularize toward the mesenteric border at the site of urethral anastomosis to give an extra length on the bowel reaching the urethra. Third, we take a suture between the seromuscular layer of bowel and the recto-urethralis to bring the posterior ileal plate closer to the urethral stump and release tension from the anastomosis. Fourth, we deepen the distal mesenteric division by firing two loads (60 mm) perpendicular to the mesentery and also mobilize the terminal ileum and ileocecal junction of the retroperitoneum to improve mobility of the ileum. Lastly, we routinely take the patient out of Trendelenburg position prior to commencing the diversion. In addition to facilitating the urethroileal anastomosis it reduces the adverse physiologic impact associated with prolonged Trendelenburg position.
Although greatly facilitated by robotic assistance, suturing still accounts for a significant portion of the operative time for creating an intracorporeal neobladder. We found that keeping suture length relatively short reduces the time required for pulling it through tissue and significantly shortens overall suturing time. We use a 6-inch length suture for suturing the anterior and posterior walls of the neobladder and a 3-inch suture for performing ureteroileal anastomosis.
Time-efficiency data for intracorporeal diversion are scant. Tyritzis recently updated the Karolinska experience with intracorporeal orthotopic diversion in 70 patients. 7 Median operative time was 7 hours (4.4–12.6 hours). This technique involves performing the urethroileal anastomosis right at the outset followed by bowel isolation and anastomosis, neobladder creation, and ureteral anastomosis using a Wallace technique. We adopted their approach of selecting the most mobile portion of the ileum but perform the actual urethro-ileal anastomosis after creating the posterior plate. Similarly, Azzouni et al. reported the influence of learning curve in 100 consecutive intracorporeal ileal conduits and showed a reduction in median diversion time (140–123 minutes, p=0.002) between first 25 and last 25 cases, although total operative time was similar (366 vs 352 minutes, p=0.802). 4
There are several limitations to this study. We have used console time as opposed to total surgical time for assessing time efficiency because for several patients time data were assessed from review of full-length video that could not yield time taken for docking and specimen extraction and closure. From a clinical perspective we realize that total surgical time is more relevant than console time. Second, the impact of various technical modifications on time efficiency represents our subjective impression and could not be objectively evaluated within the scope of the present study.
Conclusions
Robotic intracorporeal orthotopic neobladder and ileal conduit can be performed efficiently preserving established open surgical principles. Stepwise progression and standardization of individual steps help make the entire procedure time efficient. Comparative clinical studies with open surgery evaluating peri-operative morbidity and functional outcomes are necessary to evaluate its role in management of bladder cancer and are being planned at our institution.
Footnotes
Disclosure Statement
Monish Aron is a Intuitive Surgical–Honorarium recipient. Mihir M. Desai is a Consultant/Advisor for Hassen Medical and a Consultant/Advisor for Baxter. Inderbir S. Gill is a Consultant/Advisor for Hassen Medical Consultant/Advisor for EDAP.