
Abstract
Purpose:
To minimize stent-related symptoms, the proximal part of the Polaris™ stent is composed of a firm material and its distal part is composed of a soft material. The aim of this study was to compare stent-related symptoms of Polaris and Percuflex® stents and to assess the impacts of these stents on quality of life.
Patients and Methods:
A total of 144 patients were randomized to a “test” group (Polaris; n=64) or a “conventional” group (Percuflex; n=80) at the time of ureteral stent insertion after ureteroscopic stone removal surgery. Stents were allocated using a randomization program. At 1 week postoperatively, patient symptoms were evaluated using the Ureteral Stent Symptom Questionnaire (USSQ), and patients were asked complete a 10 cm visual analogue scale (VAS). Mean scores for USSQ domains and mean VAS scores were compared.
Results:
Mean patient age was 50.3 years, and the male-to-female ratio was 1:0.85. No significant intergroup differences were found in the domain scores of urinary symptoms (P=0.58), pain (P=0.87), general health (P=0.20), work (P=0.24), sexual activity (P=0.64), or additional problems (P=0.24). In addition, VAS scores were nonsignificantly different (P=0.11). Analysis of USSQ item scores, however, revealed the test group had better results for “presence of pain,” “frequency of pain killer use,” “difficulties with respect to hard physical activity,” “fatigue,” “frequency of rest,” “stent-related impact on work,” “antibiotics use” than the conventional group except for “outpatient department visits”.
Conclusion:
Compared with the conventional Percuflex ureteral stent, the new Polaris ureteral stent with a soft tail was not found to offer significant advantages in terms of voiding symptoms, pain, general health, sexual matters, or additional problems as determined by the USSQ or in VAS determined pain. Sub-analysis, however, showed that the Polaris has some advantages with respect to pain, physical activities, impact on work, and additional problems. Accordingly, the soft-tipped Polaris stent was found to have some clinical advantages over the conventional Percuflex stent.
Introduction
U
To minimize stent-related symptoms, various methods, such as correct choice of stent length, use of alpha blockers, drug-eluting stents, and changes in stent material have been studied. 2,6 –18 In particular, the distal portion of the recently introduced Polaris™ stent is composed of soft material and its proximal portion is composed of a firmer material. This distal soft portion is believed to minimize bladder irritation compared with the firmer distal portion of conventional ureteral stents.
Several questionnaires have been developed to identify ureteral stent-related symptoms. The Ureteral Stent Symptom Questionnaire (USSQ) has been translated in various languages and is widely used. 19 –22 Recently, a Korean version of the USSQ was validated. 21
The aim of this study was to compare the stent-related symptoms of the Polaris stent and a conventional ureteral stent (Percuflex®) using the USSQ and a visual analogue scale (VAS), and to assess the impacts of these ureteral stents on health-related QoL.
Patients and Methods
A total of 164 consecutive patients undergoing ureteral stent insertion after ureterorenoscopy (URS) between August 2012 and December 2013 were prospectively enrolled. Our Institutional Ethics Committee approved the study, and informed consent was obtained from all patients.
The enrolled patients were aged 16 to 80 years, and had a urinary stone necessitating temporary ureteral stent insertion after URS, as determined by surgeon discretion. The exclusion criteria applied included noncalculous disease (e.g., malignant obstruction, retroperitoneal fibrosis), recurrent ureteral stricture, loss to follow-up, pregnancy, or bilateral or long-term stent placement.
Patients were randomized to either the Polaris stent group (the test group) or the conventional Percuflex stent group (the conventional group) in a single-blinded manner (patients were unaware of allocations). Group allocations were performed using a random number generating program in the operating room before stent insertion.
All stents were inserted via a retrograde approach under fluoroscopic guidance. All stents were 6F, and stent lengths were determined based on patient height, as follows: Height <150 cm, 20 cm stent; height 150 to 165 cm, 22 cm stent; height 165 to 180 cm, 24 cm stent; and height >180 cm, 26 cm stent. All stents were inserted under fluoroscopic guidance, and in no patient did the inserted stent cross midline.
At 1 week after stent insertion, patients visited the outpatient department for stent removal and were asked to complete the USSQ. Stent-related symptoms were evaluated at 1 week after stent insertion by using the Korean version of the USSQ, which is composed of several domains—that is, urinary symptoms, pain, general health, work performance, sexual activity, and additional questions. In addition, patients were asked to indicate degree of pain on a 10-cm VAS scale.
The sample size was calculated based on the results of previous studies on stents. A total of 128 patients (64 patients per arm) appeared sufficient to detect a difference of 15% between mean index scores for urinary symptoms, pain, and general health, respectively, with 80% power.
All patients were administered antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs) (talniflunate) for 3 days after discharge. In addition, when patients were prescribed additional NSAIDs, dosages were recorded. Alpha blockers and anticholinergics were not administered. The primary outcome measure was the results of the questionnaire. Secondary outcome measures included adverse events—e.g., early stent removal because of stent-related symptoms or stent migration.
Statistical analysis was performed using PASW ver. 17.0. Mean domain scores of the test and conventional groups were compared using the Student t test. Categorical data were analyzed using the chi-square test. Statistical significance was accepted for P values <0.05.
Results
Of the 164 patients who underwent successful stent insertion, 144 patients completed the questionnaire and were included in this study. There were 64 patients and 80 patients in the test and conventional groups, respectively (Fig. 1).
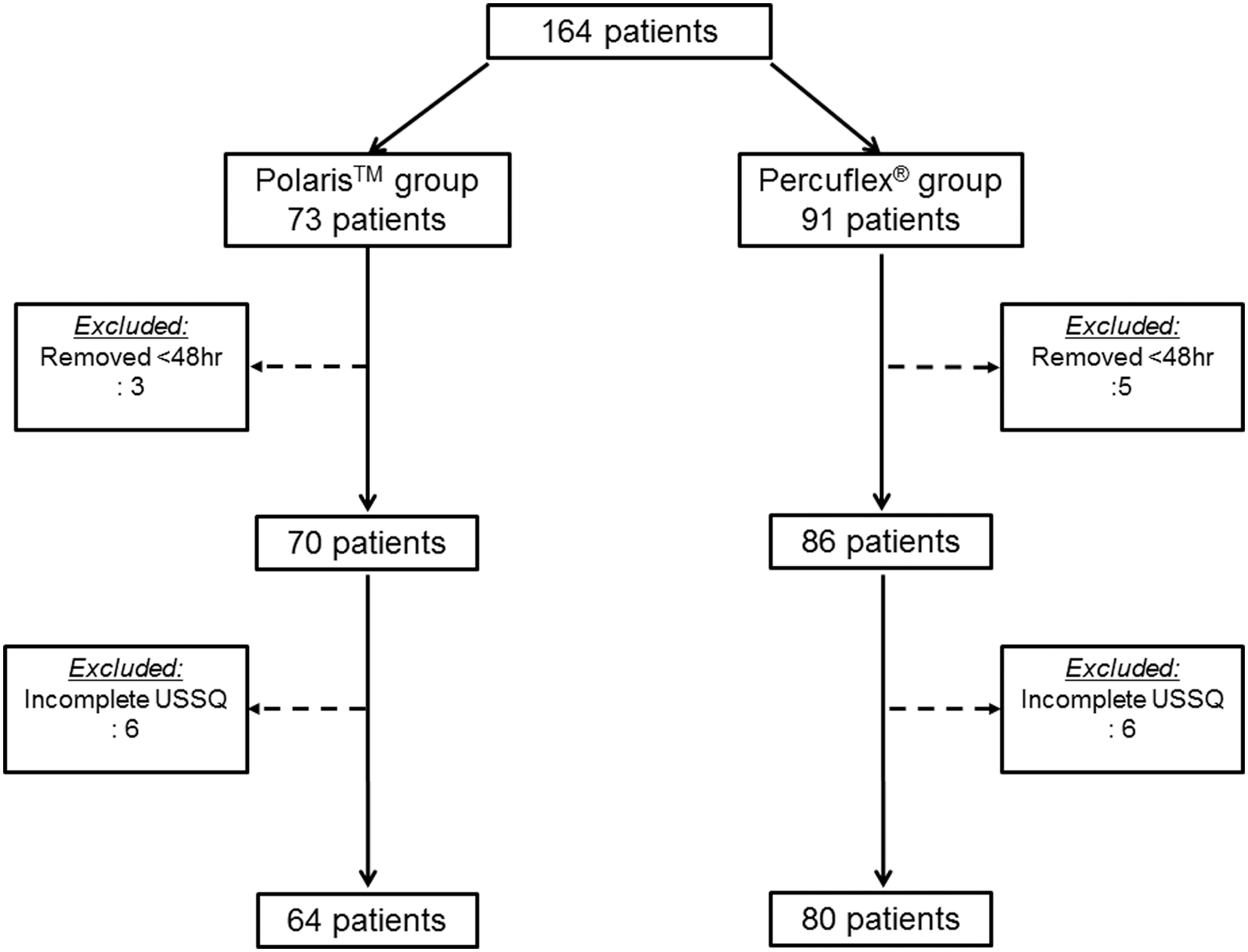
Patient selection flow chart. USSQ=Ureteral Stent Symptom Questionnaire.
Mean age of the 164 study subjects was 51.1 years, and the male-to-female ratio was 1:0.85. The demographic data of patients in the two study groups were comparable in terms of age, sex, and body mass index (BMI). (Table 1) VAS scores were not significantly different in the test and conventional groups (5.19±2.60 vs 5.46±2.93, P=0.111).
BMI=body mass index; VAS=visual analogue scale.
On comparing the mean scores for each main domain in the USSQ, no significant differences were found in any domain, including urinary symptoms, pain, general health, work, sexual activity, and additional problems (Table 2). Although no significant differences was found between domain total scores, patients in the test group reported less “pain,” less “difficulty during physical activity,” less “difficulty at work,” and less “use of antibiotics,” than patients in the conventional group (Table 3).
SD=standard deviation; VAS=visual analogue scale.
The patients in the test group reported less pain in response to question 1 in the pain domain category (the presence or absence of pain or discomfort from the ureteral stent) (1.33±0.47 vs 1.19±0.40, P=0.001), and less pain killers were needed by patients in the test group (1.93±1.07 vs 2.32±1.48, P=0.005). In the “general health” domain, patients in the test group experienced less difficulty during normal and hard physical activities (2.19±1.14 vs 2.56±1.38, P=0.01, 2.45±1.22 vs 2.88±1.45, P=0.02, respectively). In the “work” domain, patients in the test group took rests less frequently and reported fewer work-associated issues because of the presence of the stent (2.19±1.0 vs 2.85±1.42 P=0.004, 2.18±1.09 vs 2.79±1.42, P=0.015, respectively). In the “additional problems” domain, patients in the test group reported less antibiotic use than patients in the conventional group (1.40 times vs 1.66 times, P=0.033).
Patients in the test group, however, visited the outpatient department more often for stent-related discomfort (1.50 times vs 1.32 times, P=0.036). Patients in the conventional group did not give a more favorable response to any question in any domain, except for visiting the outpatient department for stent-related symptoms.
Correlation analysis showed a positive relationship existed between VAS scores and USSQ pain domain scores (R=0.640).
Early stent removal because of urinary symptoms or pain was performed in three (5.2%) patients in the test group and in five (7.9%) patients in the conventional group (P=0.243). There was no case of ureteral stent migration.
Discussion
Ureteral stents are inserted to reduce pain, relieve ureteral obstruction, improve urine passage, and prevent other complications. 1 Despite these therapeutic purposes, ureteral stent insertion often causes various stent-related symptoms, which include pain and urinary symptoms, and these symptoms impair QoL and sometimes result in emergency department or early outpatient visits. 3,7,23,24
Therefore, many studies have been conducted on the factors associated with ureteral stent-related symptoms and on methods or stent designs aimed at improving ureteral stent-related discomfort. Some studies 11,16 have concluded that correct stent length is the most important factor in terms of improving patient discomfort. Another study suggested that ureteral stent diameter is the most important factor. 2 Recently, it was suggested that medications, such as, alpha blockers and anticholinergics, might reduce stent-related pain, 9,13,14,15,18 while others advocated the importance of stent position over alpha blockers and anticholinergics. 6,8
Stent-related symptoms are partly from bladder mucosal irritation caused by the hard tip of the stent. Based on this finding, a stent with a soft distal tip (the Polaris stent) was developed and marketed recently and is expected to reduce bladder irritation symptoms and pain. Davenport and associates 25 compared the Polaris stent with the InLAY stent and found no significant reduction in pain or bladder irritation. This study, however, had the limitation of a small number of enrolled patients; we performed a prospective study in a larger number of target patients. Overall, our study showed no differences between the test group and conventional group with respect to USSQ domains, which is in line with the results of a previous study. 25
According to our analysis, the test group had favorable results for some aspects of pain, physical activity, and general performance. More specifically, the mean scores for pain and painkiller use were significantly lower in the test group, and although no significant difference was observed between the scores of other pain-related questions, all pain domain scores and VAS scores were lower in the test group.
Scores for some questions about general health and work were also higher in the test group. Patients in this group indicated less difficulty during normal or hard physical activities, took less frequent rests, and experienced fewer work-related changes. Furthermore, questions about general health and work also revealed that symptoms were less bothersome in the test group. These results suggest that the Polaris stent might have some advantages over the Percuflex stent in terms of pain relief, general health, and work performance.
The present study was conducted in a randomized, prospective manner and investigated the effects of the Polaris ureteral stent using a validated questionnaire. Although the USSQ is a validated questionnaire that is used all over the world, it has so many questions in each domain that there is a possibility of an opposing effect of questions in one domain even if there are some advantages for one group.
Our study has several imitations. In particular, we did not collect data after stent removal and, therefore, we could not evaluate changes in symptoms associated with removal. Another limitation is that it is important to approve that the baseline index, which was degree of pain in everyday and lower urinary tract symptoms (LUTS) before actual occurrence of the urolithiasis, was equal in the two groups. These patients, however, already had pain caused by urolithiasis when the stent was inserted; it was difficult to identify the perception about everyday pain or LUTS.
We tried to minimize this problem by randomization, and because more than 60 people were allocated to each group, baseline index of each group was thought to have been sufficient identification. In addition, we did not measure stent lengths, which were chosen based on patient height. Because perception of pain and stent length are known to be related to stent-related symptoms, this lack of measurement may have introduced selection bias. The randomization process, however, should have minimized selection bias.
The number of study subjects enrolled in the present study was larger than that in the previous study, 25 but we experienced hard to reach target numbers as determined power analysis because patients found it difficult to complete the questionnaire. The USSQ questionnaire contains many questions in each domain, and this is the main cause of noncompliance. A short form of the USSQ would aid further studies.
Conclusion
The Polaris ureteral stent with a soft tail shows no significant differences in terms of voiding symptoms, pain, general health, sexual matters, and additional problems when it was compared with the conventional Percuflex ureteral stent. Furthermore, the two stent groups had similar VAS scores. Analysis of the items of the USSQ questionnaire, however, revealed that the Polaris stent had some advantages with respect to pain, physical activities, work, and the use of antibiotics. Accordingly, we conclude that the Polaris ureteral stent has some clinical advantages over the conventional Percuflex ureteral stent.
Footnotes
Acknowledgment
This work was supported by Konkuk University.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.