
Abstract
Purpose:
To compare the perioperative outcomes of robot-assisted partial nephrectomy (RAPN) with open partial nephrectomy (OPN) in solitary kidneys.
Methods:
Records of 1542 consecutive RAPN performed in five high-volume centers (2007–2013) were reviewed for patients with solitary kidneys. Results were compared with solitary OPN cases performed during the same period. Cases were divided into simple (R.E.N.A.L. nephrometry score 4–8) and complex (R.E.N.A.L. 9–12) groups. Demographics, surgical, pathologic, and follow-up data were compared between OPN and RAPN in each group.
Results:
40 RAPN and 85 OPN cases were identified. For both tumor complexity groups, patients in each treatment modality were comparable. There were higher proportions of OPN cases in the complex group (61.2% vs 25%; P=0.001). For both complexity tumor groups, there was no statistical difference between the treatment modalities in overall intraoperative/postoperative complications, transfusion rate, and positive surgical margin (PSM) rates. Patients in the RAPN group had a shorter length of hospital stay. For the entire cohort, there was no difference in estimated glomerular filtration rate preservation beyond 1 month (OPN 80.51%, RAPN 81.29%). Limitations include retrospective, nonrandomized nature of the series and small number of cases in the RAPN groups.
Conclusions:
In the solitary kidney, RAPN offers comparable perioperative and short-term functional outcomes for localized tumors with low R.E.N.A.L. score. For more complex tumors, our early experience suggests comparability, but these results were obtained in selected cases and future studies will need to validate these results.
Introduction
N
Although utility of robot-assisted partial nephrectomy (RAPN) in this setting has been reported, 3 there is a paucity of data in the literature regarding comparison of this method with the open technique. The previous publications have not been comparative 4 or only compared the outcomes of RAPN with other minimally invasive techniques. 5,6 Also, given the selection biases associated with surgeon experience and choice of modality of surgical approach, direct comparison of results of different series without consideration of such factors as well as tumor complexity and patient characteristics is not possible.
In this study, we aim to compare the perioperative outcomes of RAPN with those of open partial nephrectomy (OPN) in patients with solitary kidneys.
Method
After obtaining Institutional Review Board approval, we retrospectively reviewed records of 1542 consecutive cases of RAPN performed in five high-volume centers across the United States from 2007 to mid-2013. We compared these results with the results of OPN for clinically T1/T2 renal neoplasms in solitary kidneys performed during the same period. Our inclusion criteria encompassed NSS in the setting of the solitary kidney. Cases where the contralateral kidney contributed more than 10% toward total glomerular filtration rate (GFR) were excluded from the study.
To make the groups comparable and to control for variations in tumor complexity across the two treatment arms, we stratified cases according to the radius, exophytic/endophitic, nearness to collecting system or sinus, anterior/posterior, and location relative to polar lines (R.E.N.A.L.) nephrometry score 7 into simple (R.E.N.A.L. score 4–8) and complex (R.E.N.A.L. score 9–12) groups.
The choice of surgical modality, OPN or RAPN, was at the discretion of the primary surgeon and was decided on a case by case basis. All procedures were performed by experienced surgeons who were beyond their learning curves for the given treatment modality. Demographics, surgical, pathologic, and follow-up data were compared between OPN and RAPN in each R.E.N.A.L. score complexity group. These included age, sex, body mass index (BMI), Charlson Comorbidity Index (CCI), proportion with CCI≥5, 8 American Society of Anesthesiologists score, preoperative/pathologic tumor size, ischemia time (cold and warm) and type, estimated blood loss, operative time, intraoperative complications, length of stay, pathologic data, postoperative complications, and percentage (%) of GFR preservation on day 3 and beyond 3 months.
For the RAPN group, we also assessed the number of solitary cases during each 500 RAPN cases performed by all of the five surgeons (every 100 case per surgeon). GFR was calculated by using the Modification of Diet in Renal Disease formula. Percentage of GFR preservation was defined as a ratio of postoperative GFR at 4 to 10 months compared with the preoperative GFR. Chronic kidney disease (CKD) was defined as GFR <60 mL/min/1.73 m2. Margin status was assessed by final pathologic evaluation. Postoperative complications were graded according to the Clavien classification. 9
Continuous data with normal distribution variables are presented as mean±standard deviation. Mean values are compared using the Student t test. For variables with nonnormal distribution, data are presented as median (interquartile range [IQR]), and the groups are compared using the Mann-Whitney U test. Categorical variables are compared using the chi-square test. Significance was set at P<0.05. All analyses were performed using SPSS v21 software (IBM SPSS Statistics, Armonk, NY: IBM Corp).
Surgical technique
The surgical technique for RAPN was relatively similar across the five participating institutions and has been described previously. 10,11 The transperitoneal route was used in all the cases, and zero ischemia was used selectively. Intracorporeal renal parenchymal cooling was not used in any of the RAPN cases.
OPN technique was relatively similar across the cohort and has been described previously. The extraperitoneal flank approach was used in the majority of cases, and parenchymal cooling was used selectively. Intravenous mannitol was used routinely for all OPN and RAPN cases.
Results
A total of 125 patients (40 RAPN and 85 OPN) were identified for the comparison (Table 1). The mean age of the cohort was 61.42±11.1 years. Twenty (16%) patients had a functionally solitary kidney (<10% of function on renal scan). From the patients with an anatomically solitary kidney, 82 (65.6%) patients had a history of radical nephrectomy. Forty-one (32.8%) patients had a CCI of 5 or higher. Seventy-two (57.6%) patients had a preoperative estimated GFR of less that 60 mL/min/1.73 m2 (CKD). The median preoperative tumor size was 3.5 cm (IQR 2.53). The median follow-up time was 12 months (IQR 21.3).
RAPN=robot-assisted partial nephrectomy; OPN=open partia nephrectomy; SD=standard deviation; BMI=body mass index; CCI=Charlson Comorbidity Index; CKD=chronic kidney disease.
During this time, five patients in the OPN and two patients in the RAPN group died. There were two cancer-related death in the OPN group and one cancer-related death in the RAPN group. All the patients with cancer-related death had negative surgical margins on final histologic evaluation. One of the two patients in the OPN group had a 10 cm clear-cell renal-cell carcinoma (RCC) (R.E.N.A.L. score 11, pT3a) and died 3 months postoperatively. The metastatic disease developed in the other patient in the OPN group (R.E.N.A.L. score 10, clear cell, pT1a), who died 4 years after the surgery. The single cancer-related death in the RAPN group was in a patient with a high-grade papillary cancer (R.E.N.A.L. score 5, pT1a) and history of contralateral radical nephrectomy (a high-grade papillary cancer); malignant ascites developed in the patient 1 year postoperatively. New CKD developed in 6 (16.2%) in the RAPN and 22 (26%) in the OPN group after surgery (P=0.5).
Figure 1 demonstrates the number of RAPN cases performed according to volume experience for the operating surgeons. With increasing experience, the number of RAPN cases in a solitary kidney and the number of RAPN for a complex tumor in a solitary kidney increased.
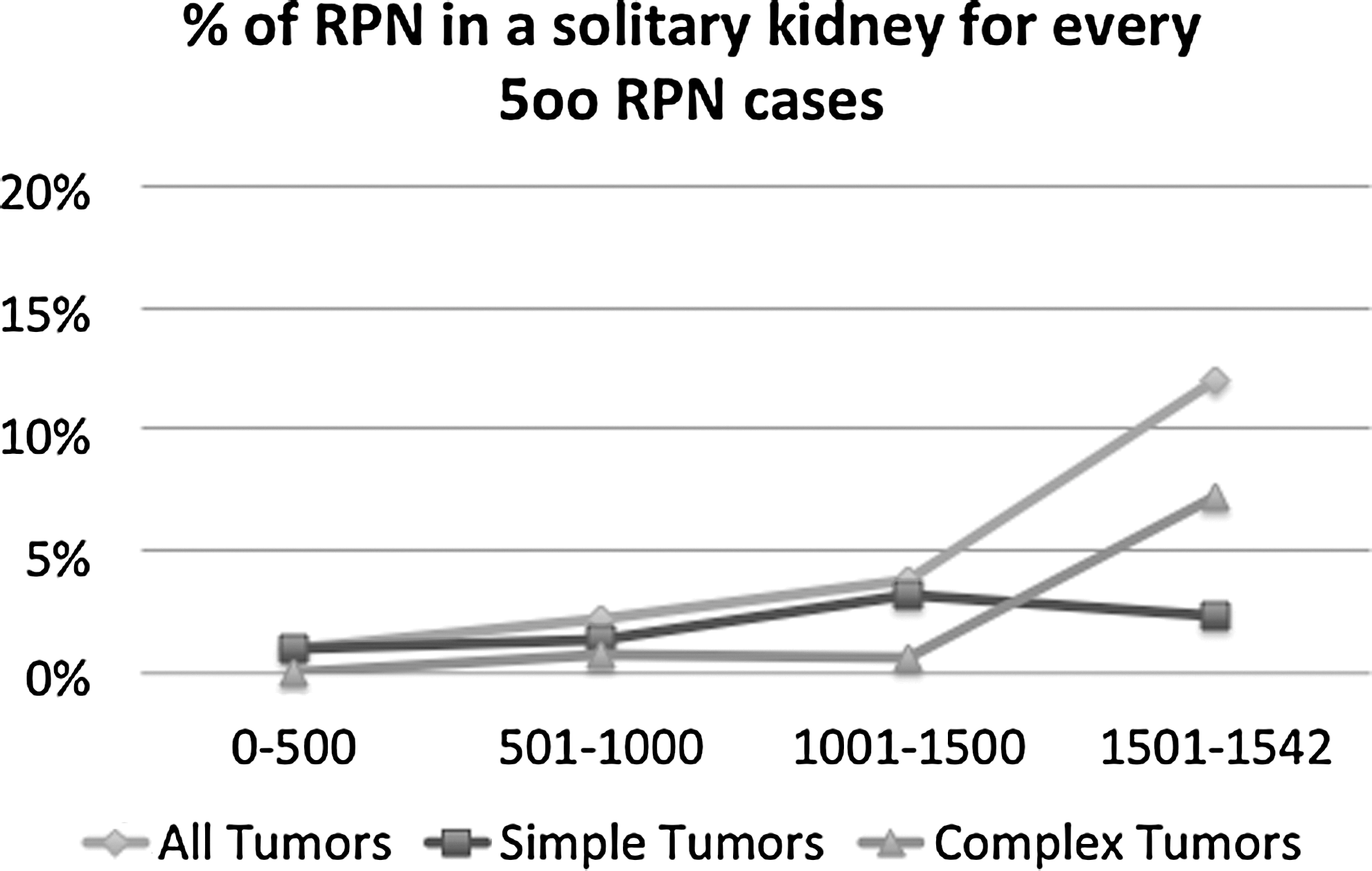
Trends in utility of robot-assisted partial nephrectomy (RPN) in patients with a solitary kidney depending on tumor complexity. The data points, represent every 500 cases (100 per surgeon) performed during the surgeon's RPN experience.
There were 63 patients allocated into the simple group (R.E.N.A.L. score 4–8) and 62 into the complex group (R.E.N.A.L. score 9–12). Higher proportions of OPN cases were in the complex group (61.2% vs 25% for RAPN; P=0.001). The pathologic features and staging information of the tumors for each treatment arm are listed in Table 2.
RPN=robot-assisted partial nephrectomy; OPN=open partial nephrectomy; IQR=interquartile range.
Simple tumor complexity group (R.E.N.A.L. score 4–8)
A total of 63 patients (30 RAPN and 33 OPN) had a R.E.N.A.L. score of 4–8 (Table 3). There was no statistically significant difference between the RAPN and OPN patients in term of age, BMI, sex distribution, or proportions of patients with CCI of ≥5. There was no difference in median R.E.N.A.L. score between the two groups (RAPN 6 vs OPN 7; P=0.06). The intraoperative data were comparable between the two surgical methods; however, the median warm ischemia time (WIT) in the RAPN group (15 min) was shorter than the median WIT in the OPN patients (23 min) where this was used. There was no difference between the groups in terms of intraoperative complications (RAPN 3.3% vs OPN 0; P=0.47). The single intraoperative complication belonged to a patient in the RAPN group who required repair of renal vein injury.
R.E.N.A.L.=radius, exophytic/endophitic, nearness to collecting system or sinus, anterior/posterior, and location relative to polar lines; RAPN=robot-assisted partial nephrectomy; OPN=open partial nephrectomy; IQR=interquartile range; SD=standard deviation; EBL=estimated blood loss.
There was no difference between the groups in the rate of postoperative complications. The high-grade complications in the RAPN group consisted of two grade III complications, one urine leak necessitating stent insertion, and one postoperative bleeding from pseudoaneurysm necessitating selective angioembolization. In the OPN group, high-grade complications consisted of three grade III and four grade IV complications. Grade III complications included two urine leaks treated with stent insertion and one episode of urine infection in a patient with a stent in situ necessitating stent change. Grade IV complications consisted of two cases of temporary dialysis and two intensive care unit (ICU) admission for nonurologic causes (pulseless cardiac arrest and respiratory insufficiency).
The positive surgical margin (PSM) rates were comparable between the two groups (RAPN 6.7% vs OPN 9%; P=1.00). The percentage of GFR preservation at the time of discharge (RAPN 78.6±23.2 vs OPN 65.3±33.2; P=0.07) and beyond 3 months postoperatively (RAPN 82.1±22.7 vs OPN 88.4±32.3; P=0.5) was similar between the two groups. The hospital length of stay was shorter in the RAPN group (3 vs 5 days; P<0.001).
Complex tumor complexity group (R.E.N.A.L. score 4–8)
A total of 62 patients (10 RAPN and 52 OPN) had a R.E.N.A.L score of 9–12 (Table 4). With regard to age, BMI, sex distribution, or proportions of patients with CCI of ≥5, there was no statistically significant differences between RAPN and OPN patients. There was no difference in median R.E.N.A.L. score between the two groups (RAPN 9.5 vs OPN 10; P=0.42). The intraoperative data were comparable between the two surgical methods. There was a trend toward higher rate of intraoperative complications (RAPN 10% vs OPN 1.9%; P=0.06) in RAPN patients. Intraoperative complications included one case of small bowel serosal tear in the RAPN group. In the OPN group, the complications consisted of one pleural injury, necessitating repair and chest tube insertion. In the RAPN group, all of the tumors were resected with warm ischemia; the mean WIT was 22.7±5.8 minutes. In the OPN group, 25(48%) of tumors were removed under warm ischemia, and the mean WIT was 23.9±8.1 minutes.
R.E.N.A.L.=radius, exophytic/endophitic, nearness to collecting system or sinus, anterior/posterior, and location relative to polar lines; RPN=robot-assisted partial nephrectomy; OPN=open partial nephrectomy; IQR=interquartile range; SD=standard deviation; EBL=estimated blood loss.
Postoperative complication rates were similar between RAPN and OPN patients—40% and 38.5%, respectively (P=1.99). The high-grade complication in the RAPN group consisted of a case of urinary leak (Clavien IIIb), which was managed successfully with ureteral stent insertion. There were three grade IV complications in the RAPN group. These included one ICU admission for managing high blood pressure and two cases of temporary dialysis. In the OPN arm, there were six high-grade complications (three IIIs and three IVs). The grade IIIs consisted of two postoperative bleedings and one urinary leak. One of the two bleeding episodes necessitated selective angioembolization and the other one was managed with a return to the operating room without the need for nephrectomy. The urinary leak was managed successfully with urinary stent insertion. The grade IV complications in the OPN group consisted of three cases of temporary renal dialysis. Two had CKD stage II and one had CKD stage III pre-op and all three upstaged one CKD stage after recovery.
The PSM rates were comparable between the two groups (RAPN 10% vs OPN 7.7%; P=0.5). The percentage of GFR preservation at the time of discharge (RAPN 65.5±34.7 vs OPN 55.4±26.4; P=0.29) and at median 6-month follow-up was (RAPN 80.3±23.7 vs OPN 74±22; P=0.4) similar between the two groups. The hospital length of stay was shorter in the RAPN group (4 vs 6 days; P=0.001).
Discussion
PN when possible is the absolute indication for management of renal neoplasm in a solitary kidney. The initial experience with OPN was developed in this setting. With growing experience, NSS has been performed for a variety of tumors with relative or elective indications. 1,2 Newer minimally invasive techniques for NSS, however, have to be tested and proven in these settings before their routine use in the setting of solitary kidney. Previous publications have compared the outcomes of OPN with laparoscopic partial nephrectomy in the setting of solitary kidney. 12 Before introduction of tumor complexity classifications, 7,13 however, direct comparison between surgical techniques lacked this objective factor. Typically, even in centers in which there is a high level of minimally invasive experience, more complex tumors are performed with OPN. As a result, if the tumor anatomic complexity are not accounted for, more complications could be associated with the open approach. 14
In this series, we divided the tumors according to complexity, and although there are a higher percentage of complex tumors performed with OPN (61.2% vs 25%), overall the patients in each complexity group are comparable at baseline. For the less complex tumors (R.E.N.A.L. score 4–8), we have demonstrated that the RAPN and OPN are comparable. There was no difference in terms of complications, PSM, and overall functional outcome between the two surgical techniques. The rate of surgical margins in the RAPN group (6.7%) is higher than our previously reported rate of 2.2% 15 for this technique. This rate is because of only two cases of PSMs and mainly reflective of small cohort size, but could also reflect an attempt by the surgeon to resect close to the tumor to minimize the amount of parenchyma that is being removed during the resection (enucleation).
While some authors have sanctioned surgical enucleation with oncologic outcomes equivalent to standard PN, 16 others have advocated some although minimum healthy renal parenchyma resection. 17 Overall the incidence of PSM in the solitary kidney PN series is higher than in patients with a normal contralateral kidney. 18 Also, there is controversy with regard to considering surgical margins as a surrogate for oncologic outcomes. Some studies have demonstrated that PSM after PN increases the probability of local recurrence without influencing cancer-specific survival, 19 while others have shown that PSM increases the risk of local recurrence as well as metastasis. 15
The median WIT for simple tumors was 15 (IQR 9) minutes, which is within the safe range of <25 minutes described by Thompson and associates. 20 Although a growing body of evidence suggests that the amount of renal parenchyma removed rather than WIT is the determinant of final degree renal function preservation, 21,22 long WIT, especially in the setting of preexisting renal impairment and solitary kidney, is an important modifiable factor. 23 –26 The rates of intraoperative (3.3%) and postoperative complications (30%) are slightly higher than in some of the published RAPN series, 27 but they are comparable with results from other OPN series for solitary kidneys. 12,28,29 From a functional point of view, with the mean follow-up time of 12 months, the degree of GFR preservation was >80% (82.1±22.7) for the RAPN patients with low tumor complexity. This is similar to previous published results for OPN series. 12 The main difference between the open and robotic group was 2 days shorter hospital stay in favor of the robotic cohort.
For more complex tumors, our results were similar between the two treatment arms; however, a significantly larger number of cases were performed with the OPN technique. The rate of intraoperative complications in the RAPN group was 10%, and this was not statistically significantly different from the 1.9% in the OPN group (P=0.06). Both of these values were because of a single intraoperative event in each treatment arm, and it is fair to assume that the intraoperative complications were similar between the two groups. Larger cumulative experience with the OPN and also the ability to perform the procedure under a cool ischemia condition allows the surgeon to perform complex tumor resection and reconstruction with good functional and oncologic outcomes and acceptable morbidity. 12,24,30 Although this series has demonstrated that RAPN in a solitary kidney with a tumor with high nephrometry score is feasible, these results were obtained in high-volume robotic centers and by very experienced robotic surgeons.
Overall, the cumulative robotic experience in this setting is very limited and OPN remains the gold standard technique for treating complex tumors in patients with a solitary kidney. Future developments in RAPN techniques, including intracorporeal cooling, 31 will allow urologists to further their experience in the setting of PN and reproduce every aspect of the open technique with a minimally invasive approach.
One criticism of this study is that the selection of cases for the modality of PN was not randomized, and this is likely a source of bias. With early RAPN experience, only simple tumors were selected for this approach, but as shown in Figure 1, with increasing experience, more complex tumors in a solitary kidney were managed using this modality. Despite this, a larger volume of complex tumors in this setting were managed with the OPN approach. The stratification of the tumors according to complexity allowed us to compare the outcomes between the two approaches, but overall volume experience for RAPN in this setting remains limited.
For tumor stratification based on the R.E.N.A.L. score, other authors have previously used a simple (R.E.N.A.L. 4–6), intermediate (R.E.N.A.L. 7–9), and complex (R.E.N.A.L.10–12) division. 32 Given the small number of cases in the RAPN group, we devised a two-group classification to allow for adequate number of cases for analysis. This, although unlikely to affect the results, but could make future comparison to the results of this study challenging.
Another criticism that could be raised is lack of matching between the two groups in the study design. By finding a matching case for every RAPN patient in the OPN groups, many of the complex cases in the OPN group would have been eliminated from the series. This could have falsely given the impression of comparability, because percentages of complex tumors between the two treatment modalities would have appeared similar and also would have further reduced the size of the already small, solitary kidney PN cohort. Given the small number of cases and small number of events of interests (complications, PSM), we did not perform any multivariable analysis in this study. Trifecta and margin, ischemia, and complication are some of the composite outcomes that have previously been proposed for assessing perioperative outcomes associated with PN 27,33,34 ; however, given the liberal use of cold ischemia in OPN, direct comparison of clamp time between the two groups was not possible.
Retrospective, multi-institutional design of this cohort could have affected certain aspects of our results. For example, the reporting of intraoperative complications was not standardized, and it is likely that minor complications, such as a small pleural/peritoneal tear in the OPN group or minor issues such as difficulty with establishing pneumoperitoneum in the RAPN group, were not readily reported.
This study represents the largest series of RAPN in the setting of a solitary kidney. It also represents the only comparative study comparing the outcomes with OPN. The limitations include the retrospective, nonrandomized nature of the series and the small number of cases in the RAPN groups, particularly the small number of patients with complex tumors. The follow-up is relatively short, and longer follow-up data are needed.
Conclusion
In the setting of NSS in a solitary kidney, presuming careful patient selection and adequate surgical experience, RAPN may offer comparable perioperative and short-term functional outcomes for localized renal masses with low R.E.N.A.L. score when compared with OPN. For more complex tumors, our early experience suggests comparability, but these results were obtained in selected cases and by high-volume surgeons. Future studies will need to validate these results.
Footnotes
Disclosure Statement
Jihad Kaouk is a speaker for Endocare. Mohamad Allaf receives a clinical research grant from Intuitive Surgical. Michael Stifelman is a lecturer for Intuitive Surgical, and a consultant for Surgiquest and Vascular Technology, Inc. Craig Rogers is a consultant for Intuitive, Ethicon, and Vascular Technology, Inc. Sam Bhayani is a consultant for Surgiquest and Intuitive Surgical. Mark Ball receives a clinical research grant from Intuitive Surgical. For the remaining authors, no competing financial interests exist.