
Abstract
Background
Patients and Methods:
From June 2009 to October 2013, 10 patients with PG who were treated with retroperitoneoscopy were included in the study. Minimal effective dosage α-blockade with phenoxybenzamine was routinely used. Preoperative, intraoperative, and postoperative baseline data were collected and analyzed. Meanwhile, two reviewers independently searched and identified 8 retrospective studies and 23 case reports in the Medline, Embase, and Science Citation Index between 1998 and 2013.
Results:
Operations in 9 of 10 patients were successfully completed without conversion; one case was converted to open surgery because of left accessory renal artery injury. Mean operative time, blood loss, and postoperative hospital stay were 97.8±20.6 minutes, 44.4±8.2 mL, and 4.8±3.5 days, respectively. There were three complications in this series, including accessory renal artery injury, renal vein injury, and chylorrhea.
Conclusions:
Retroperitoneoscopic resection is feasible, effective, and safe in the treatment of patients with PG according to our preliminary clinical experience and has distinct advantages including direct access to the tumor, less intraperitoneal interference, precise dissection, and minimal invasiveness.
Introduction
P
Because of its low morbidity, anatomic variation, and unstable hemodynamics during operative manipulation, both open and laparoscopic management are a great challenge even for the experienced urologist. Laparoscopic resection of retroperitoneal PG was first described by Janetschek and associates 4 in 1998. Since then, several surgeons have reported their experiences with laparoscopic PG resection, although these have only been reports of a single case or a small number of cases.
We present our surgical experience and outcomes for retroperitoneal laparoscopic resection in 10 patients and systematically review the relevant literature to evaluate its safety and efficacy.
Patients and Methods
Patients
Between June 2009 and October 2013, retroperitoneal laparoscopic excision for PG was performed in 10 patients (4 men and 6 women), ages 45 to 63 years, by a single surgeon (JW) in our clinical center. Six patients had intermittent hypertension (180–210/160–180 mm Hg) with headache and dizziness. Three patients had persistent hypertension (180–240/160–180 mm Hg and resistant). One patient was asymptomatic, and the PG was discovered incidentally on abdominal sonography during a health examination. All masses located in the retroperitoneal space were primary and diagnosed by CT scanning (Fig. 1). The urinary vanillylmandelic acid (VMA)/24 h level was elevated (normal <13.6 mg/24 h) in five patients. Clinical features of patients are listed in Table 1.

Abdominal CT scan demonstrates a left periaortic lesion below the renal vein. Note the partial necrosis within the tumor (axial section).
VMA=vanillylmandelic acid.
Preoperative preparation
All patients was given α-blockade (phenoxybenzamine, 10–20 mg, twice daily, orally) starting with 30 mg/day and elevated gradually every 2 to 3 days with an increase of 10 to 20 mg to 120 mg/day for at least one week. Other antihypertensive drugs, including β-blockade (metoprolol), calcium channel blockers (nifedipine), and angiotensin converting enzyme inhibitors (captopril), were selected for combination if needed. A stable blood pressure (about 120/80 mm Hg) and heart rate (<90 beats per minute) for 3 days were prerequisites for the surgical procedure. Abdominal CT angiography (CTA) was performed for preoperative assessment and surgical planning (Fig. 2). The patients were hydrated with 5% glucose (1000 mL) and 0.9% sodium chloride (1000 mL) to expand blood volume within 48 hours before operation. Red blood cells (3 U) and plasma (600 mL) were prepared for the operation.
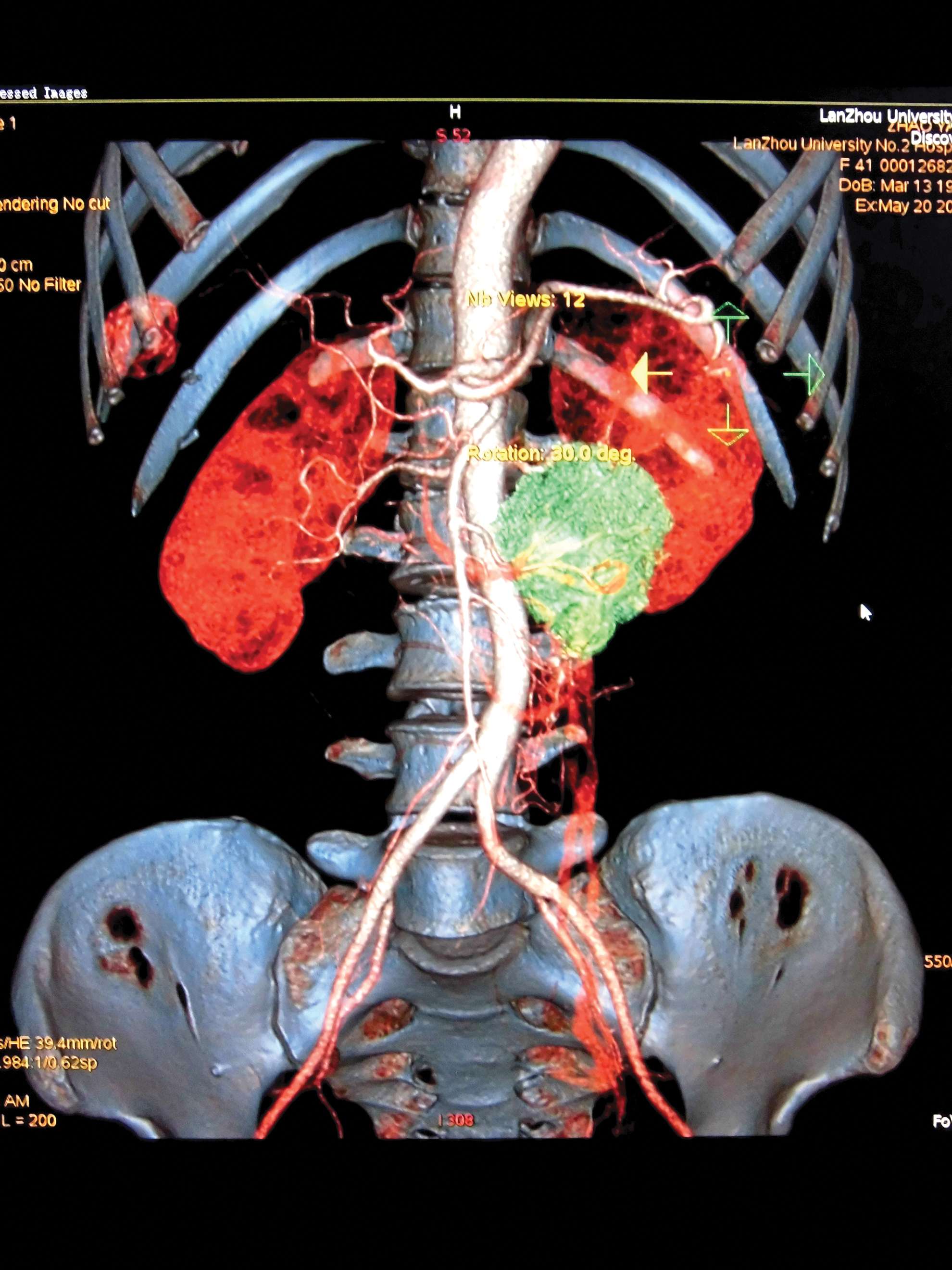
Computed tomography angiography demonstrates the anatomic relationship between the tumor and surrounding major vessels by three-dimensional reconstruction.
Operative procedure
The laparoscopic excisions were performed through the retroperitoneal approach as follows: After induction of general anesthesia, the patient was placed in the lateral decubitus position with the lesion side up. An incision (15 mm) was made in the triangle between the 12th rib and psoas, and then a tunnel was created so that the surgeon's index finger could push the peritoneum forward. One homemade balloon was placed in the extraperitoneal space and infused with 800–1000 mL air to bluntly dissect enough working space. Then, two trocars (5 mm below the costal margin in the anterior axillary line, 10 mm 2 cm above the superior border of the iliac crest in the midaxillary line) were inserted and guided by the index finger. An additional 5 mm laparoscopic port may be placed and used to assist exposure if desired at the subcostal margin of midaxillary line. CO2 was insufflated and maintained at 13 to 15 mm Hg pressure during the operation. The retroperitoneal fat was freed to reveal the Gerota fascia, which was then incised longitudinally (Fig. 3).

Retroperitoneal fat is cleared from the Gerota fascia, which was then incised longitudinally along the psoas muscle.
With these relationships delineated in terms of imaging data and real-time inspection, exploration was performed with the monopolar electrocautery hook by initially incising the overlying peritoneum. Circumferentially, the harmonic scalpel carefully dissected the surrounding major vascular structures and branches supplying the tumor (Fig. 4). Intraoperative laparoscopic ultrasonography aided in tumor localization and its relation to the surrounding structures. Multiple feeding vessels were individually ligated and divided between clips or with the harmonic scalpel directly. To avoid squeezing the tumor, bipolar coagulation forceps were effective and produced less side injury on hemorrhage.

Dissection of feeding vessels by the harmonic scalpel.
Once completely mobilized, the tumor (<3 cm) was removed by a specimen bag from the posterior axillary port. For a tumor >3 cm, specimen removal can be performed by extending the incision (Fig. 5). Drainage of the lumbar fossa was discontinued at an average of 2 days.

The cut surface of the excised retroperitoneal paraganglioma.
Literatures selection and data extraction
A systematic literature review was performed through Medline, Embase, and Science Citation Index to identify relevant studies in December 2013. Searches were restricted to publications in English. Given the paucity of the available evidence, retrospective studies (RS) and case reports (CR) were included in this review. The following terms and search strategy were used: (Paraganglioma OR Ectopic pheochromocytoma OR Retroperitoneal) AND Laparoscop*. The Truncation symbol ‘*’ means all suffix variations of a root word. Both the “related-articles” feature of PubMed and references of articles were also applied to expand the search scope by hand. The latest date for an updating search was December 28, 2013.
Two reviewers (YL, NX) independently extracted data from each study, including: First author, publication data, country, population characteristics, operative time, blood loss, postoperative hospital stay, conversion, complications, and follow-up. The level of evidence of included studies was rated according to criteria by the Center for Evidence-Based Medicine (
Results
Data from patients
All operations were completed by retroperitoneoscopy, except one case converted to an open procedure because of left accessory renal artery injury. The data were tabulated in Table 2 and expressed as mean±standard deviation. Mean operative time, blood loss, and postoperative hospital stay were 97.8±20.6 min, 44.4±8.2 mL, and 4.8±3.5 day, respectively. There were two intraoperative vascular injuries and one postoperative chylorrhea (Clavien II) in this series. The first was a left accessory renal artery injury converted to end-to-end anastomosis; the second was a 2-mm rupture of the renal vein closed by a titanium clip; the third was chylorrhea appearing as a white milky discharge from the drainage tube (50 mL/24 h) on postoperative day 4, which spontaneously ceased through unobstructed drainage after 10 days. Pathologic results showed typical features of PG in all patients (Fig. 6).

Numerous brown neurosecretory type granules housed in the cytoplasm by chromogranin A staining.
Mean follow-up was 16 months with a range of 2 to 29 months. In this period, there were no recurrences. Blood pressure was measured two times by the patients at home every day. Hypertension of three patients gradually decreased to 120/80 mm Hg 1 month after operation; antihypertensive medication was necessary for six patients to maintain blood pressure at 150/110 mm Hg. One patient, however, still had poorly controlled blood pressure (180/140 mm Hg) after combination antihypertensive therapy.
Data from the literature
We preliminarily identified a total of 3106 records through combined search strategies. Two reviewers independently excluded 404 reviews and 2668 clearly irrelevant articles by browsing titles and abstracts. Three articles were further excluded for two unavailable full texts and one non-PG report. 5 –7 Both 8 retrospective studies and 23 case reports that were published between August 1998 and February 2013 were eventually included in this review. 2,4,8 –36 These trials involved 84 patients (male 37, female 25, and unclear 22), with 3 patients who underwent robot assisted operation, 68 patients who underwent the transperitoneal laparoscopic approach, and 13 patients who underwent retroperitoneal laparoscopic approaches. Because of the low evidence level of the literature, the data were only described systematically rather than pooled for meta-analysis.
Medians of operative time, blood loss, and postoperative hospital stay were 202.5 minutes (95–545 min), 100 mL (10–1500 mL), and 4 days (1–13 days), respectively. 2,8 –17,21 –26,28,31,32,34 –36 Four studies described their reasons for conversion to open surgical procedures such as intraoperative bleeding, poor visibility of posterior veins, difficulties in identifying the ureter, and the dense adherence to surrounding structure.s 13,21,34,36 Postoperative complications were only reported by five publications with the transperitoneal laparoscopic approach, which were wound infection, ileus, lymphatic fistula, gluteal hematoma, lymphedema, vena caval bleeding, lymph ascites, as well as pneumonia, 4,12,13,21,22 The overall complication rate was eight of 68 (11.8%), including six (8.8%) Clavien I, one (1.4%) Clavien II, and one (1.8%) Clavien III. Both recurrence and metastasis were not found during 17.5 months (3–108 mos) follow-up in 18 articles. 4,8 –11,16 –18,21,22,24,25,29 –32,34,36
Discussion
Approximately 50% of patients with catecholamine-secreting tumors have true paroxysmal hypertension in clinical practice; 35% to 45% have persistent hypertension, and the remaining patients have no hypertension. 37 Hypertension as one of the typical clinical symptoms is the result of catecholamines (epinephrine, norepinephrine, and dopamine) that are secreted by the tumors and released into the systemic circulation. In our series, six patients had paroxysmal hypertension, three patients had persistent hypertension, and only one was normotensive. It is not difficult to identify retroperitoneal PG with classic clinical symptoms, elevation of 24-hour urinary VMA, and abdominal CT scanning. For any suspected retroperitoneal PGs, especially for patients with atypical symptoms and negative results from a biochemical test, the radio-pharmaceuticals 131I-metaiodobenzylguanidine has been most commonly used for localization and identification.
Once a diagnosis of PG is made, appropriate preoperative pharmacologic preparation, which is similar to that for pheochromocytoma, is necessary to decrease the risk of perioperative complications and involves hypertension control, correction of arrhythmia, as well as volume expansion. All patients with PG in our study had obtained adequate control of blood pressure and heart rate at least 3 days before operation. One patient's blood pressure, however, which was normal before operation, decreased sharply from 120/80 mm Hg to 60/30 mm Hg after removal of the neoplasm. This indicates that unfunctional PG is relative and more attention should be paid to the preoperative preparation in case of possible catecholamine-induced complications and especially hypotensive crisis after tumor removal. 33 It was thus important to monitor hemodynamic changes in real time and have full communication between surgeon and anesthetist during the operation, especially during removal of the neoplasm.
Most recently, abdominal CTA was used to map tumor-related vasculature through three-dimensional reconstruction, which might help to clearly define surrounding anatomic structures and delineate the optimal plane and depth of dissection. Given the deformation and shift of major vascular anatomy compressed with tumor growth, CTA was necessary for preoperative evaluation in our institute. When CTA of vascular structures of interest was unclear, it could be reconstructed and identified to obtain a thorough assessment by means of the intelligent terminal of Picture Archiving and Communication Systems.
With regard to laparoscopic treatment, transperitoneal, retroperitoneal, and robot-assisted approaches can be feasible depending on tumor location and personal preference. In 84 patients of the 31 included articles, the laparoscopic transperitoneal approach was the mainstay because of the broad working space and maximal tumor exposure (trans lap vs retro lap vs robot-assisted: 68 vs 13 vs 3). The da Vinci robotic system was successfully used because of optimal vision with delicate accuracy in three case reports, but there were no distinct advantages compare with the other two approaches. In contrast, switching instruments is a drawback and may lead to difficulties in patients with active bleeding. 11,19,28
Although there were few reports on retroperitoneoscopic treatment, we preferred this access to all patients with PG in our clinical center and have not found obvious drawbacks. The retroperitoneal approach offers the advantage of dissection without the interference of the intra-abdominal organs, thus avoiding the respiratory and hemodynamic effects of the CO2 pneumoperitoneum and facilitating direct access without the need to mobilize the abdominal organs. On the other hand, it is convenient to accurately separate the anatomic plane for a lateral neoplasm and avoids the possible implanted metastasis. It is undeniable that the smaller working space is the biggest shortcoming compared with intraperitoneal space. According to our clinical experience, for a tumor less than 10 cm in diameter, it is enough to get the best visualization of the major vessels adjacent to the tumor. Even if peritoneal rupture takes place during the operation, artificial pneumoperitoneum should be rebuilt through repairing of the peritoneum.
Operative time, blood loss, and complications are the important indicators to assess effectiveness of the procedure, which is associated with tumor site, vascular anatomy, and the degree of adhesion. From our data, operative time and blood loss are 104.3±17.7 minutes and 40.7±5.4 mL, respectively. One case was excluded from the statistic because of conversion to an open procedure. Sixteen studies reported specific operative times, whose median is 202.5 minutes (95–545 min); four trials 4,21,31,34 showed 290.4±119.8 minutes, 123 minutes (80–210 min), 50–600 minutes, 132–300 minutes, respectively. Seventeen of the 33 studies reported blood loss, whose median is 100 mL (10–1500 mL). Six trials 2,4,20,27,31,32 showed 162.0±191.0 mL, <100 mL, 70 mL (10–150 mL), 20 mL (0–1000 mL), 100±175 mL, 516 mL (390–600 mL), respectively. The data from the above studies fluctuated greatly partially because of variability in the number and course of feeding vessels and laparoscopic experience.
Importantly, there were two intraoperative complications and one postoperative complication in our series. In patient 2, one arterial vessel diagonally crossing the surface of the tumor was mistaken for a feeding vessel and transected after using titanium clips. Both obvious pulsatility at the proximal end and a pale lower pole of kidney demonstrated the lesion of accessory renal artery. The procedure was converted to an open operation after quickly removing the tumor; the lower pole turned to red gradually by end-to-end anastomosis. A 2-mm sidewall rupture of the renal vein in patient 3 was closed by a titanium clip. Patient 8 was found to have chylorrhea on postoperative day 4 because of possible thoracic duct injury; it spontaneously ceased through unobstructed drainage after 10 days. The similar complication was described in which a 5×6 cm mass in the left para-aortic region medial to the inferior pole of the left kidney was removed and discharged 200 mL lymph through the drainage on postoperative day 2; this spontaneously ceased after 3 days. 20 Mitchell and colleagues 22 reported that in one case with resection through laparoscopic transperitoneal access, there was high-grade small bowel obstruction from an internal hernia in the early postoperative period, which was reduced and closed by laparoscopy on postoperative day 4.
All tumors in the whole cohort had negative surgical margin with pheochromocytomal features. Metastasis is identified as the feature of malignancy rather than cellular characteristics. 11 Thus, the importance of follow-up is equal to the surgical treatment. In our series, all patients were followed up for a mean of 16 months with a range of 2 to 29 months. Blood pressure had ideal control in 10 patients, except for 1. There were no recurrences and distant metastasis. Similarly, 14 articles described relatively good results of follow-up from 3 to108 months postoperatively.
On the basis of our 10-year retroperitoneoscopic practice, we summarize preliminary experiences as follows: 1. For the lateral decubitus position, dissecting along the psoas muscle is a quick, direct access to the retroperitoneal neoplasm. 2. Retaining some fatty tissues on the surface of the tumor should be helpful to facilitate retraction and avoid an excessive increase in catecholamine level. 3. The so-called breakwater technique is recommended to deal with a vessel <5 mm, which certainly reduces accidental hemorrhage. The dissection of large tissue should be avoided because of vascular displacement oppressed by tumor. In our opinion, the procedure of harmonic scalpel is observation→separation→clamp→cut. 4. Use of bipolar forceps is effective and safe for precise hemostasis without damage to surrounding structures.
38
The electrocautery hook is a safe, simple, and inexpensive instrument for precise separation in a narrow space. Its J-tip may be used to hook and dissect the perivascular tissues. 5. Laparoscopic ultrasonographic guidance could intermittently reassess tumor location, delineation of its vascular supply, as well as relation to surrounding structures.
16
Conclusion
Laparoscopic resection for PG is considered to be more challenging even to experienced surgeons because of the variable anatomic presentation, the rich vascularization, and the potential of hemodynamic instability during operative manipulation. According to our initial clinical experience, however, the risk will be minimum through reconstruction of CTA, intraoperative ultrasonic localization, and skilled use of laparoscopic instruments. Retroperitoneoscopic resection of PG is a feasible, effective, and safe alternative to surgical treatment of PG according to our limited clinical experience, and indicates distinct advantages including direct access to the tumor, less intraperitoneal interference, precise dissection, and minimal invasiveness. Although there were only 10 patients in our study, it is the largest series compared with publication data because of the rareness of PG. Currently, one multicenter study on this project is under way and proposes to report a larger sample size in the near future.
Footnotes
Disclosure Statement
No competing financial interests exist.