
Abstract
Objective:
To compare operative outcomes of robot-assisted radical prostatectomy (RARP) in obese and nonobese patients with prostate cancer.
Materials and Methods:
A literature search of MEDLINE, EMBASE, Google Scholar, and the Cochrane Library was performed up to March 2014. All studies that have assessed operative outcomes of RARP in obese and nonobese patients were included. Outcome measures were perioperative and functional results, including operating time, estimated blood loss (EBL), complications, length of hospital stay (LOS), positive surgical margins (PSMs), and recovery of continence and potency. Pooled odds ratios (ORs) and weighted mean differences (WMDs) with 95% confidence intervals (CIs) were calculated using fixed-effect or random-effect model. Subgroup analysis was performed for institutions with greater experience of RARP in obese cases.
Results:
Thirteen observational studies from 12 study population were included for 1821 obese patients compared with 4801 nonobese patients. Operating time (p=0.0001; WMD: 24.28; 95% CI, 11.93–36.64) and EBL (p=0.003; WMD: 38.28; 95% CI, 13.45–63.11) were significantly increased in obese patients compared with nonobese counterparts. There was no significant difference in complications, LOS, or PSM rates. Subgroup analysis for studies that have involved ≥100 obese cases showed consistent results, but the increases in operating time (9.8 minutes; 95% CI, 1.7–18 minutes) and EBL (14 mL; 95% CI, 5.0–23 mL) were much lower compared with the original analysis. As for functional outcomes, obese patients showed significantly higher probabilities of incontinence (p=0.003; OR: 1.41; 95% CI, 1.13–1.77) and impotency (p=0.02; OR: 1.29; 95% CI, 1.03–1.61) at 1 year.
Conclusions:
Perioperative outcomes of RARP in obese patients are comparable with those in nonobese patients, except for significant but small increases in operating time and EBL. Surgeons should initiate RARP procedures in obese cases after overcoming the learning curve. Further studies should be performed to evaluate the functional outcomes for obese patients undergoing RARP.
Introduction
O
In recent 10 years, tremendous advances have been seen in the development of surgical modalities. Da Vinci robotic surgical system, which incorporates minimally invasive surgery with improved visualization and delicate control, is becoming popular among urologic surgeons. With this profound surgical system, radical prostatectomy using robot-assisted technique has gradually became the preferred approach. Through many series from different institutions, it has been demonstrated that robot-assisted radical prostatectomy (RARP) is a safe and feasible procedure with comparable functional and oncologic outcomes. 5 Compared to open procedure, RARP could be a better option for patients with higher body mass index (BMI). 6 However, controversy still remains about the influence of obesity on operative outcomes of RARP based on previous studies. Meta-analysis draws together conflicting results of individual primary studies and offers higher-level evidences to healthcare providers. Accordingly, we performed a meta-analysis to pool studies currently available to compare the operative outcomes of RARP in obese and nonobese patients.
Materials and Methods
The present study was performed adhering to the PRISMA (preferred reporting items for systematic reviews and meta-analyses) statement, 7 including search strategy, selection criteria, data extraction, and data analysis.
Search strategy
To identify relevant studies, a comprehensive computerized literature search of MEDLINE, EMBASE, Google Scholar, and the Cochrane Library was performed in March 2014. No time restriction was applied. The search terms used to identify potentially eligible studies were “robot,” “robotic,” “robotics,” “robot-assisted,” “robotic-assisted,” and “prostatectomy,” and “obesity.” Additional manual searches were performed of the reference lists of included studies, reviews, and meta-analyses. The searches were restricted to English language publications.
Study selection
The following inclusion criteria were used: (1) studies comparing the operative outcomes of RARP between obese and nonobese patients based on BMI classifications; (2) studies defining obesity as having a BMI ≥30 kg/m2, and binary classification of the study population was available based on this boundary. In the event of duplicate publications by the same institution, the most recent study with larger cohort or higher quality was included in the meta-analysis.
The following exclusion criteria were used: (1) the inclusion criteria not being met, (2) nonobese cohort comprising only overweight patients or those with normal BMI, and (3) studies comparing operative outcomes between obese and nonobese patients with just high-risk or locally advanced prostate cancer. The authors of included studies were contacted wherever the data were unavailable. For articles without full text (i.e., conference abstract), the study was excluded for a lack of data when only one or none of outcome measures was extractable in the abstract.
Three reviewers (T.X., X.W., and L.X.) identified all studies that appeared to fit the inclusion criteria for full review. Each reviewer independently selected studies for inclusion in the review. Disagreement between the extracting authors was resolved by consensus or referred to a third author (S.Z.). The methodological quality of included studies was assessed with a modification of the Newcastle-Ottawa Scale: scores >5 were defined as high quality, and a score <5 as low quality. 8
Data extraction
Two reviewers (X.Z. and L.Q.) independently extracted data from the included studies, and disagreements were resolved by discussion until a consensus was reached. The objectives were to evaluate perioperative and functional outcomes of RARP for obese patients compared with nonobese counterparts. The following variables were extracted from each study: author, year of publication, patient age, initial prostate-specific antigen (PSA) level, prostate size, pathologic stage, operating time, estimated blood loss (EBL), complications, length of hospital stay (LOS), and positive surgical margin (PSM) rates. Urinary and erectile functions after RARP were evaluated among patients who were preoperatively continent and potent, respectively. In the process of data extraction, prostate size was uniformly expressed as weight measures, the value of which could be estimated multiplying the volume by a correction factor of 1.2 in the few studies providing only prostate volume 9 ; a binary classification was applied for pathologic stage and patients were categorized as those with locally advanced (pT3–4) disease or not.
Statistical analysis
The meta-analysis was performed using Review Manager (RevMan 5.2). The weighted mean difference (WMD) and odds ratios (ORs) were used to compare continuous and dichotomous variables, respectively. For studies that presented continuous data as median and range values, the means and standard deviations (SDs) were calculated using algorithms described by Hozo et al. 10 If interquartile range (IQR) values were provided, SDs were calculated using formula IQR/1.35 according to the Cochrane Handbook. 11 All results were reported with 95% confidence intervals (CIs). Statistical heterogeneity was assessed using the χ 2 test with a p-value of <0.05 considered to indicate statistical significance, and heterogeneity was quantified using the I 2 statistic. I 2 values of 25%, 50%, and 75% corresponded to low, medium, and high levels of heterogeneity, respectively. Data were pooled using the fixed-effect model, unless a statistically significant high heterogeneity (i.e., I 2>50%) existed across studies; otherwise, the random-effect model was used if heterogeneity existed. To evaluate the difference in results for studies with greater experience of RARP in obese patients, subgroup analysis was also performed considering studies that involved ≥100 obese cases. Sensitivity analysis for all included cohorts was performed to explore the influence of relatively low-quality studies (studies without full text and those with small-numbered cohorts).
Results
Literature search
The process of study selection was depicted in Figure 1. The initial literature search found 134 potential studies. Based on the inclusion and exclusion criteria, 103 studies were excluded after reading the title, abstract, or full text. Of the remaining 31 studies, 12 duplicate reports with relatively small cohorts were excluded and most of them were published as conference abstracts. Other six conference abstracts, which provided only one extractable outcome of interests or none, were not included in our meta-analysis because of a lack of data. 12 –17 Of the remaining 13 studies, Zilberman et al. 18,19 reviewed the records of a prostate cancer cohort from North Carolina and reported the impact of BMI on PSM and other perioperative outcomes separately. Thus, 13 articles based on 12 study populations were included in a pooled meta-analysis. 18 –30

Flow diagram of study selection.
Characteristics of the included studies
The studies included were published between 2005 and 2013. Eleven studies were published as full text 18 –27,30 and two as abstracts, 28,29 and all the full-text studies were deemed to be high quality according to the Newcastle-Ottawa Scale. Eight of the study populations were from the United States, 18 –21,23 –26,30 one from Germany, 29 one from the United Kingdom, 27 one from Netherlands, 28 and one from Australia, 22 respectively. All the studies were retrospective analyses comparing RARP between obese and nonobese patients. A total of 6622 patients were included: 1821 patients in the obese group and 4801 patients in the nonobese group.
Nine studies provided the extractable data of the patients' age and initial PSA level. 18,20 –26,30 Prostate size was available in seven studies, 18,20 –22,25,26,30 one of which reported on the prostate volume. 25 Eight studies with full text provided available values of operating time, 18,20,22 –26,30 and seven provided values of EBL. 18,20,23 –26,30 Complications were reported in 10 studies, 20 –26,28 –30 two of which further performed classifications according to the Clavien system 26,30 and three graded the complications as minor and major. 23,24,29 Minor complications are those classified as Clavien grade 1–2, while major complications are Clavien grade ≥3. LOS was available in only six studies. 20,22 –26 All 12 study populations were included in the meta-analysis of the patients' pathologic stage and PSM rates. As for functional results, three studies 20,21,26 provided continence rates at 6 months and four 23,25,26,29 provided values at 1 year; three studies 25,26,29 reported potency rates at 1 year. Hence, 1-year postoperative functional outcomes were evaluated in our meta-analysis.
Meta-analysis results
The baseline characteristics of selected studies and their perioperative results are summarized in Table 1. In the current meta-analysis, obese patients were noted to be younger (60.1 vs. 61.7 years; p=0.0004; WMD: −0.76; 95% CI, −1.19 to −0.34) and have larger prostate size (52.2 vs. 50.7 g; p=0.007; WMD: 2.15; 95% CI, 0.58–3.71) compared with the nonobese group. There was no significant difference between two groups regarding initial PSA level (p=0.12; WMD: −0.23; 95% CI, −0.52 to 0.06) and the proportion of patients with locally advanced prostate cancer [p=0.10; OR: 1.12; 95% CI, 0.98–1.29 (Fig. 2)].
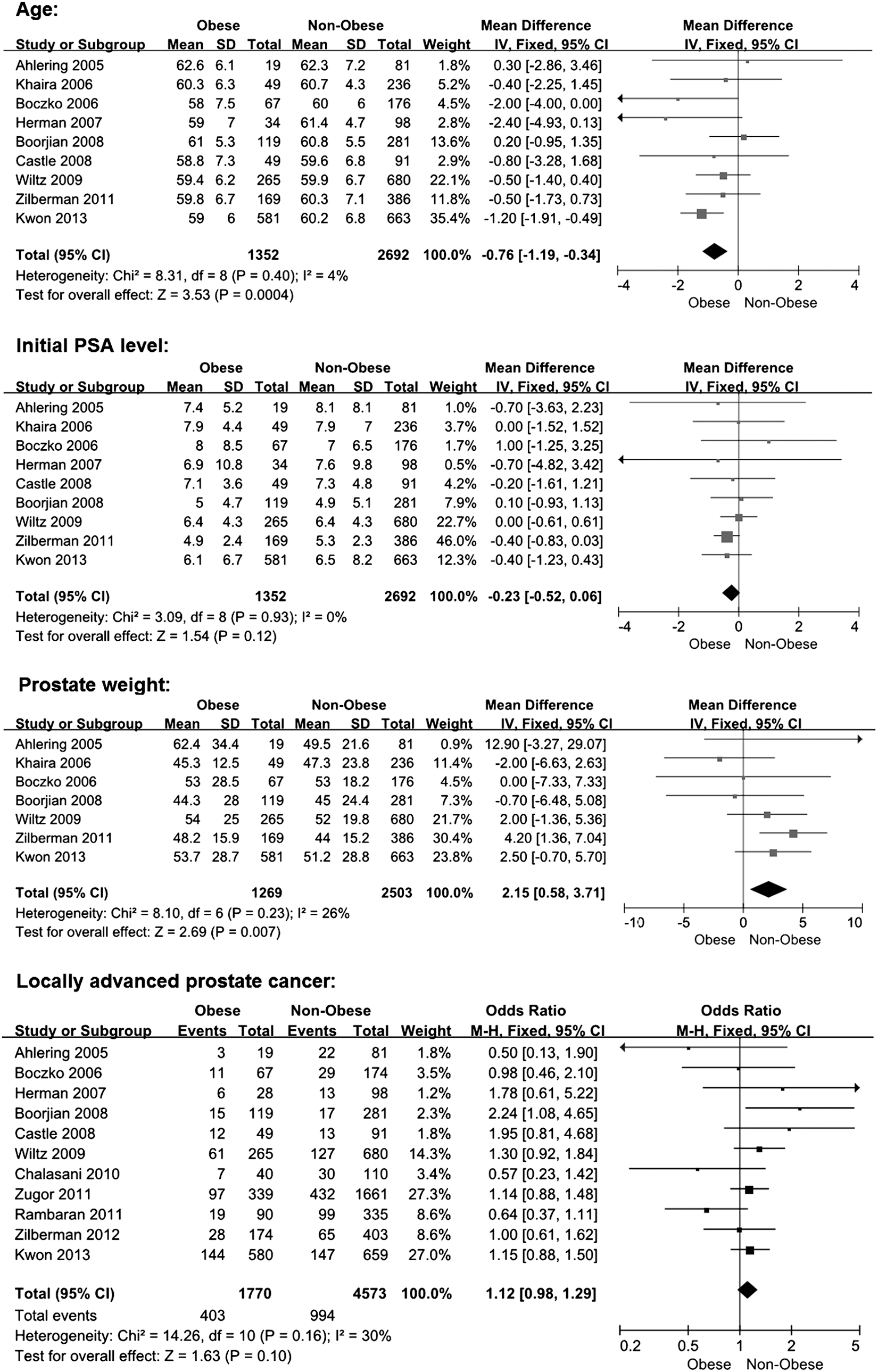
Forest plots of baseline characteristics of patients. CI, confidence interval; SD, standard deviation.
BMI, body mass index; EBL, estimated blood loss; LOS, length of hospital stay; NOB, nonobese; OB, obese; OT, operating time; PSA, prostate-specific antigen; PSM, positive surgical margin.
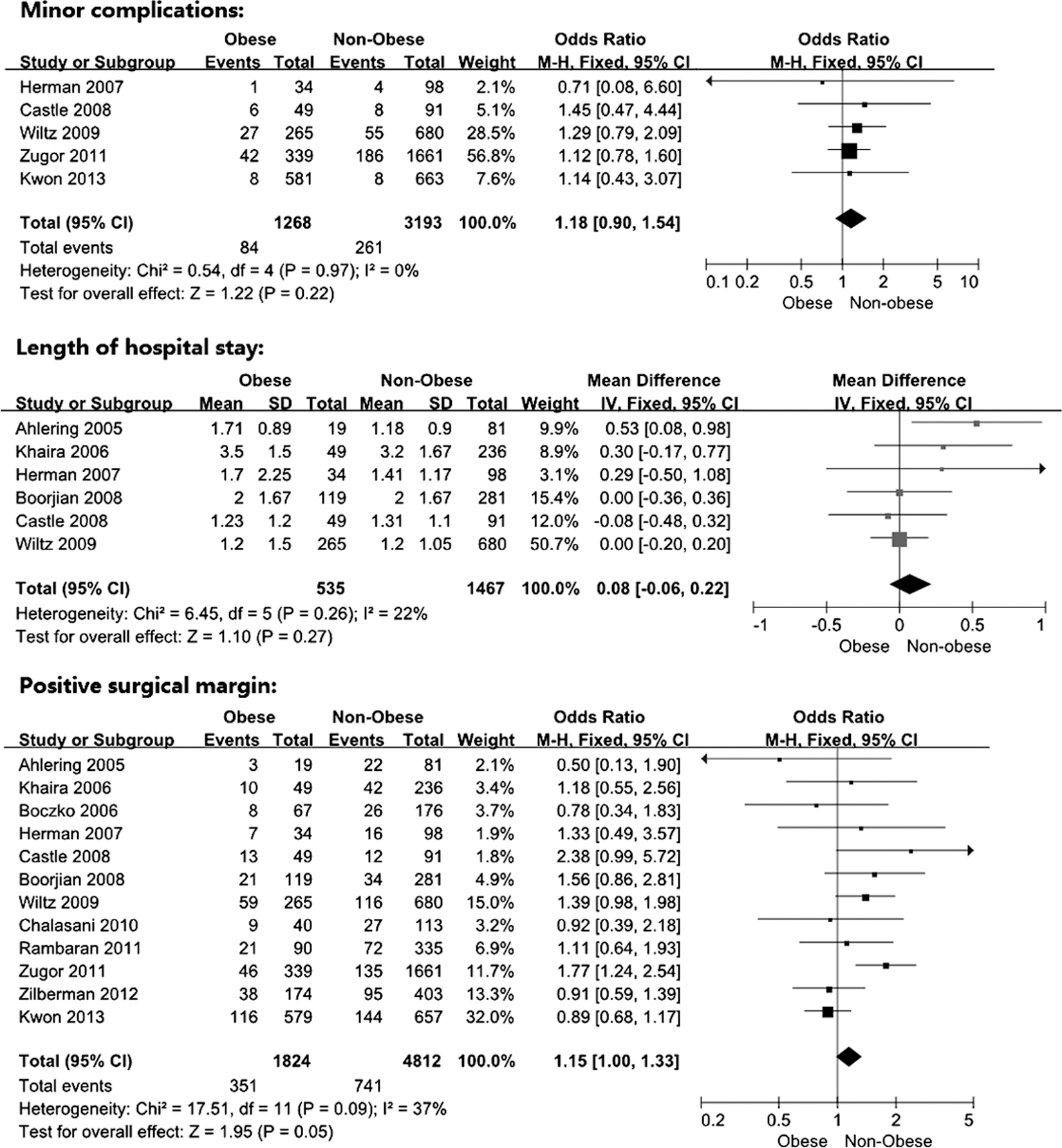
Figure 3 shows the forest plots of perioperative outcomes. The nonobese group had significantly shorter operating times (p=0.0001; WMD: 24.28; 95% CI, 11.93–36.64) and less EBL (p=0.003; WMD: 38.28; 95% CI, 13.45–63.11) than the obese group. There was no significant difference between two groups for similar overall complication rates (10.0% vs. 10.3%; p=0.05; OR: 1.21; 95% CI, 1.00–1.48). For studies in which surgical complications were graded, no significant difference was observed in either major (p=0.60; OR: 1.14; 95% CI, 0.69–1.87) or minor complications (p=0.22; OR: 1.18; 95% CI, 0.90–1.54). LOS was comparable between two groups (p=0.27; WMD: 0.08; 95% CI, −0.06 to 0.22). Compared with the nonobese patients, the obese exhibited a slight but insignificant tendency for a PSM status (19.2% vs. 15.4%; p=0.05; OR: 1.15; 95% CI, 1.00–1.33).
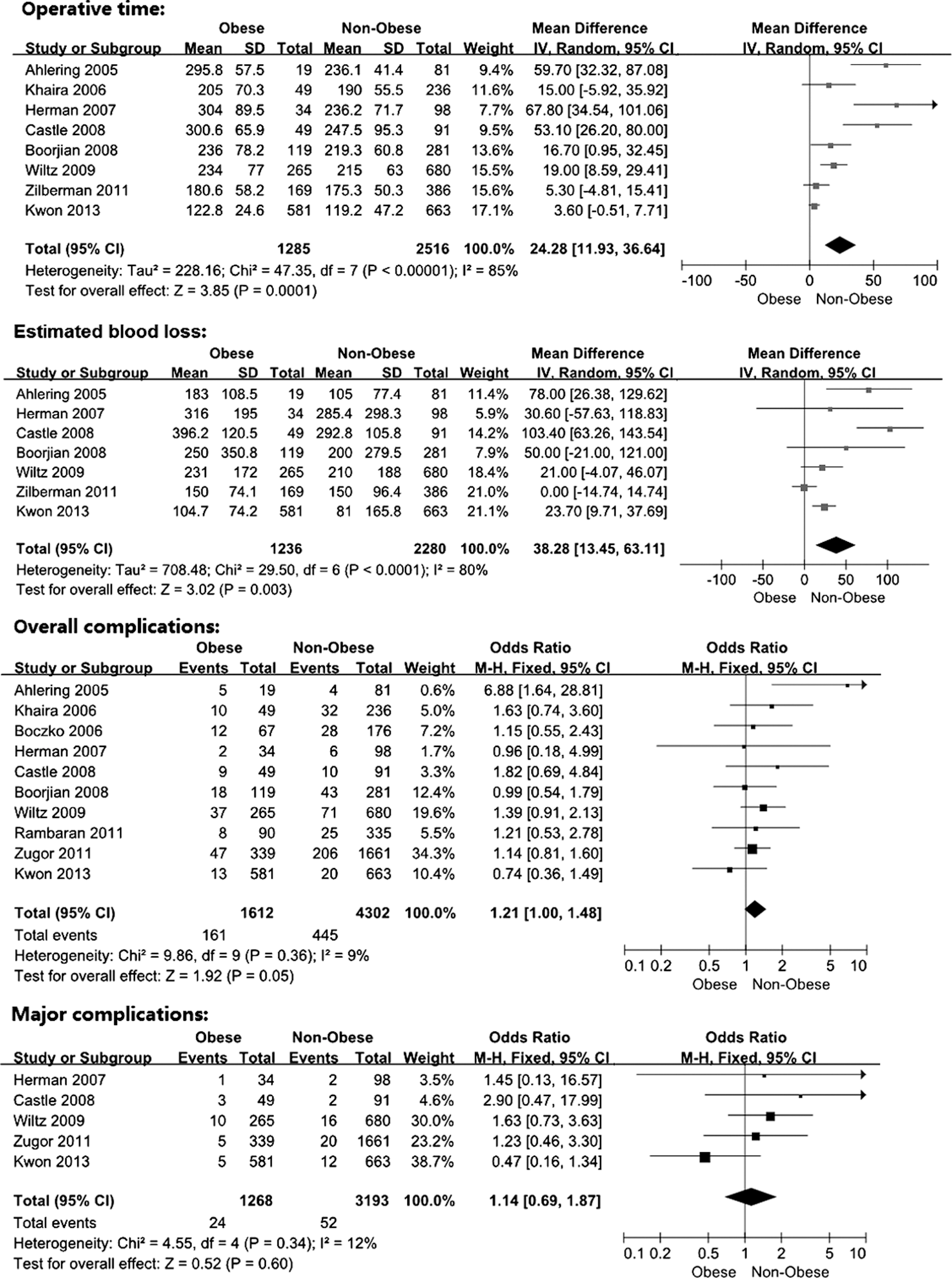
Forest plots of perioperative outcomes.
Pooled results of functional outcomes from four available studies were provided in Figure 4. The obese group showed significant inferiority in 1-year postoperative recovery of continence (p=0.003; OR: 1.41; 95% CI, 1.13–1.77) and potency (p=0.02; OR: 1.29; 95% CI, 1.03–1.61).
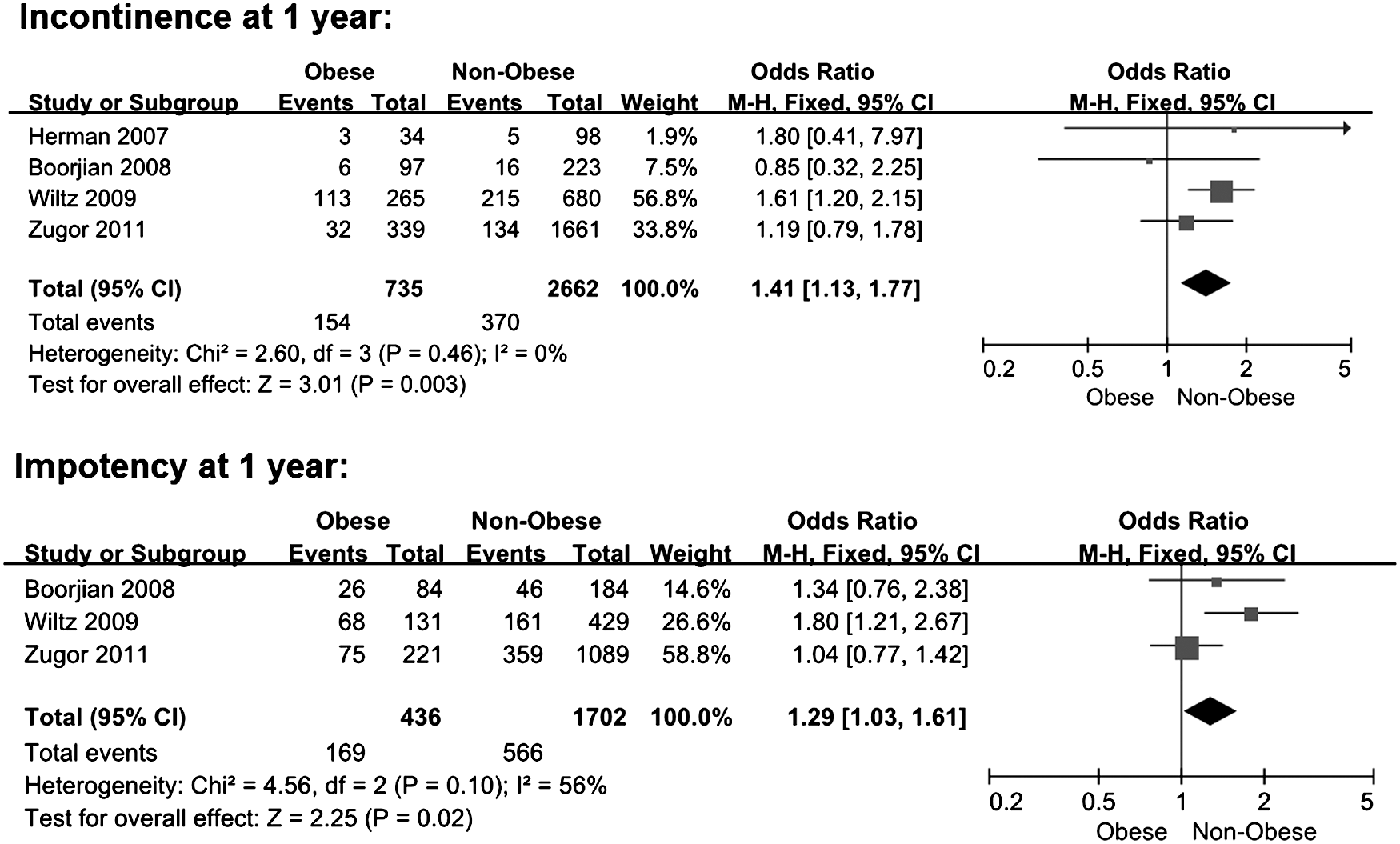
Forest plots of functional outcomes.
Subgroup analysis
As shown in Figure 5, subgroup analysis of perioperative outcomes for institutional experience in obese cases included five study populations with ≥100 obese patients. 18,19,25,26,29,30 It continued to demonstrate significant increases in both operating time (p=0.02; WMD: 9.75; 95% CI, 1.70–17.81) and EBL (p=0.003; WMD: 14.30; 95% CI, 4.97–23.62) in obese patients compared with nonobese counterparts. Overall complication rates were comparable between two groups (p=0.32; OR: 1.12; 95% CI, 0.89–1.41). When the complications were graded, there was no significant difference in either major (p=0.88; OR: 1.04; 95% CI, 0.61–1.77) or minor complications (p=0.25; OR: 1.17; 95% CI, 0.89–1.55). No significant difference in LOS between groups was observed (p=1.00; WMD: 0.00; 95% CI, −0.17 to 0.17). There was no significant difference between groups in PSM status, either (p=0.17; OR: 1.23; 95% CI, 0.92–1.66).

Forest plots displaying perioperative outcomes of subgroup analysis including studies with ≥100 obese cases.
Sensitivity analysis
Sensitivity analysis was performed for all included studies by removing two conference abstracts without full text 28,29 and full-text studies with small-numbered cohorts. There were still no differences between two groups regarding complications (overall: p=0.17; OR: 1.20; 95% CI, 0.93–1.54; major: p=0.76; OR: 1.10; 95% CI, 0.61–1.97; minor: p=0.23; OR: 1.28; 95% CI, 0.85–1.92), LOS (p=0.70; WMD: 0.03; 95% CI, −0.12 to 0.18) or PSM rates (p=0.34; OR: 1.08; 95% CI, 0.92–1.28). RARP procedures still showed less than ideal efficacy in obese patients, including significantly longer operating time (p=0.0008; WMD: 19.57; 95% CI, 8.15–31.00) and more EBL (p=0.01; WMD: 32.67; 95% CI, 7.47–57.86), which were similar to the general analysis. Unfavorable functional outcomes in obese patients also remained regarding incontinence (p=0.003; OR: 1.52; 95% CI, 1.15–2.01) and impotency rates (p=0.004; OR: 1.80; 95% CI, 1.21–2.67) postoperatively.
Discussion
Obesity has been implicated as an acknowledged risk factor for unfavorable outcomes of surgeries. Numerous comparative studies compared operative outcomes of RARP between obese and nonobese patients, but no consensus has ever been reached so far. 12 –30 Using the meta-analytical methods, we tried to make an objective and scientific assessment by pooling the currently available studies including a total of 6622 patients. The present study found significant increases in both operating time and EBL in obese men undergoing RARP (Fig. 3). Several reasons could explain the association between obesity and the technical difficulties of RARP. (1) Unique body habitus, especially the large abdominal girth, makes inconvenient manipulations, including suboptimal port placement and long distance from skin to operative field. (2) Excessive fat tissue leads to suboptimal visualization and narrowed working space. It also makes surgical manipulations (e.g., anastomosis and nerve sparing) difficult and time consuming. (3) Prolonged operating time inevitably increases the intraoperative blood loss. Obesity is also associated with higher risk of bleeding due to disorders of coagulation and hemostasis. 31 (4) Since excessive intraperitoneal contents tend to fall into the pelvis, surgeons would compensate for this by using exaggerated Trendelenburg position during RARP. 22 However, it might aggravate the impairment of cardiorespiratory function and exert an effect on local operation. The vasodilatation resulting from elevated CO2 concentration might also be adverse for hemostasis. Besides, it is noteworthy that the obese population in our meta-analysis had a significantly larger prostate size. Previous studies have observed this phenomenon in men with or without prostate cancer. 32,33 The enlargement of prostate might confer surgical complexity and go against favorable outcomes following radical prostatectomy to some extent. Studies by Khaira et al. 22 and Zilberman et al. 18 suggested that the surgical step of vesicourethral anastomosis would be elongated by the larger prostate, which constituted an obstacle to anterior urethral dissection and resulted in a shorter urethral stump and a technically challenging anastomosis. Hence, it can be deduced that the obesity, either alone or in combination with its influence on the prostate, might reduce the efficacy of RARP procedures more or less.
Although RARP was less efficacious in obese patients, increases in operating time (WMD: 24 minutes; 95% CI, 12–37 minutes) and EBL (WMD: 38 mL; 95% CI, 13–63 mL) were likely of limited clinical impact. LOS, another important variable reflecting the surgical efficacy, was comparable between two groups. Subgroup analysis for large obese cohorts still showed significantly elevated operating time (WMD: 9.8 minutes; 95% CI, 1.7–18 minutes) and EBL (WMD: 14 mL; 95% CI, 5.0–23 minutes) in the obese group, but the increases were much lower (Fig. 5). Herein, it is speculated that the experience of RARP operated on obese cases could be a key determinant of surgical results. Wiltz et al. 26 found a dramatic improvement from the initial 100 cases to 200 cases in operating time, EBL, and transfusion rates for all BMI subgroups and particularly so for obese patients. With a higher level of surgeon's proficiency, technical difficulty associated with obese patients might be attenuated after the infancy of the learning curve process.
In respect of the safety of RARP, there was no significant difference for overall, major, or minor complications in comparison with nonobese group (Fig. 3). Similar complication rates between two groups suggest that RARP is a safe option for patients with higher BMI. Open conversion rate, another classic parameter, was not included in the current meta-analysis and very few of robotic surgeries in five studies were converted to open procedures for failure to progress. 20,23,24,26,27 Only one of these studies showed an increased requirement of open conversion in obese patients, but most occurred during the initial 100 cases. 26 The safety of RARP should be attributed to technical advantages of da Vinci robotic system, including three-dimensional vision and master-slave delicate hand motion. Besides, some adverse events potentially occurring in obese cases could be avoided by experienced surgeons.
PSM, the surrogate of surgical quality, is treated as an important pathologic outcome for malignancy surgeries as well. Surgeons should endeavor to minimize the likelihood of PSM as oncologic control is the ultimate aim of radical prostatectomy. As previously mentioned, obesity is associated with relatively difficult manipulation. More importantly, the correlation between obesity and the increased risks of aggressive prostate cancer has been observed in both clinical and experimental researches. 34 –36 In the current study, we also observed greater involvement of the prostate gland with tumor in obese cohorts for all available studies describing the tumor size. 24 –26,30 Accordingly, significant association between obesity and the increased PSM following open radical prostatectomy has been suggested by previous studies. 4,34 By contrast, our meta-analysis showed that RARP provided a noninferior surgical quality in obese patients, and this conclusion became more statistically robust when small obese cohorts were isolated (Figs. 3 and 5). Open surgeries in the obese population are limited by anatomical difficulties, which would be completely or partly resolved with the aid of robot-assisted system. However, one of the included studies with a large obese cohort found higher PSM rates in the prostate base area based on the surgical specimens from obese patients, and the authors attributed it to the vague identification of the demarcation line between the prostate and the bladder neck. 19 Previous study proved that the incidence of PSM in RARP procedures correlates significantly with the level of proficiency. 37 To eliminate positive margins, surgeons should overcome the learning curve before initiating RARP procedures in obese patients.
Functional outcomes were also analyzed in the current meta-analysis. We found inferior functional outcomes of obese patients in comparison with nonobese counterparts at 1 year (Fig. 4). Although this result that was obtained from only four studies is less than robust, the association of obesity with worse functional outcomes after radical prostatectomy has been the predominant conclusion in relevant studies of recent 5 years. 4,26,38 –40 It is reasonably intuitive that excessive periprostatic fat tissue would result in suboptimal visualization and manipulation and higher risks of trauma to the neurovascular bundle or membranous urethra during the course of RARP. However, it should be noted that obese patients had significantly worse baseline erectile function due to endothelial dysfunction and inflammation. Obesity might also bring about additional physical strain on the bladder, thus resulting in more preoperative urinary problems and a prolonged duration of return to continence. Considering these underlying issues unrelated to surgical expertise, suboptimal functional outcomes should be discussed with obese patients during preoperative counseling. In the era of RARP, propensity score-matched studies are needed to evaluate the influence of obesity on long-term functional outcomes after adjusting confounding factors.
The present study has some limitations. There was no randomized controlled trials (RCTs) included in the meta-analysis. Some obese patients might have been excluded from undergoing RARP because of cardiorespiratory comorbidities. Two of the selected studies were published as conference abstracts, and some details of included studies were not applicable. Besides, there was variability in surgical technique as well as a lack of standard definitions of outcome measures among institutions. Functional analysis was also relatively immature in this study. However, sensitivity analysis was performed to minimize the heterogeneities, and the results remained similar to the original analysis after removing relatively low-quality studies. We also performed subgroup analysis to reveal the influence of confounding factors on the results. Our study has a very large sample size through including all available studies related to RARP in a comparison between obese and nonobese patients for the first time. In the case of these two distinct cohorts (obese vs. nonobese), randomization and blinding of RCTs are not feasible when comparing RARP procedures between groups. The meta-analysis of observational studies could commendably fill in the blanks, thus providing constructive suggestions for both clinical urologists and healthcare policy makers.
Conclusions
Based on the current meta-analysis, perioperative outcomes of RARP in obese cohorts were equivalent to those in the nonobese counterparts, except for the less than ideal efficacy that might be of limited clinical impact. RARP could be a feasible option for obese men with prostate cancer after the infancy of the surgeon's learning curve process. Further studies should be performed to evaluate the functional outcomes for obese patients undergoing RARP.
Footnotes
Acknowledgments
This work was supported by the Science and Technology Commission of Shanghai Municipality (No. 12140901200) and the National Natural Science Foundation of China (No. 81270695).
Disclosure Statement
No competing financial interests exist.