
Abstract
Objective:
To determine the incidence of prostate cancer identified on holmium laser enucleation of the prostate (HoLEP) specimens and evaluate variables associated with prostate cancer identification.
Patients and Methods:
All patients undergoing HoLEP between 1998 and 2013 were identified. Patients with a known history of prostate cancer were excluded. Multivariable logistic regression assessed variables associated with identification of prostate cancer on HoLEP specimens and Gleason 7 or higher prostate cancer among the malignant cases. The Gleason grade was used as a proxy for disease severity. Each of the models was adjusted for age, preoperative prostate-specific antigen (PSA), and HoLEP specimen weight.
Results:
The cohort comprised 1272 patients, of whom 103 (8.1%) had prostate cancer identified. Prostate cancer cases had higher pre-HoLEP PSA (p=0.06) but lower HoLEP specimen weight (p=0.01). On multivariate logistic regression, age and preoperative PSA were associated with increased odds of prostate cancer being present (p<0.01 each), while increasing HoLEP specimen weight was associated with decreased odds of prostate cancer (p<0.001). Men older than 80 had 20% predicted probability of being diagnosed with prostate cancer. Seventy-eight percent of prostate cancer cases were Gleason 6 or less. The pre-HoLEP PSA was associated with increased adjusted odds of intermediate- or high-grade prostate cancer.
Conclusion:
Prostate cancer identified by HoLEP is not uncommon, but is generally a low-risk disease. Older patients with smaller prostate glands have the highest odds of prostate cancer identification.
Introduction
B
Before the adoption of prostate-specific antigen (PSA) screening, almost 20% of prostate cancer was diagnosed from TURP. 6 –8 However, since the introduction of PSA screening, this rate has declined significantly to 6% to 8%. 8 Previous studies have demonstrated that up to 12% of men undergoing HoLEP will be found to have prostate cancer in their analyzed tissue. 9,10 Most studies have suggested that prostate cancer identified on HoLEP is generally indolent, but some men may ultimately require subsequent treatment of their prostate cancer. In our experience, post-HoLEP robot-assisted radical prostatectomy, although feasible with encouraging oncologic outcomes, is a more challenging operation associated with longer functional recovery times compared to historical controls. 11 Thus, identifying men at increased risk for clinically significant prostate cancer is an important consideration in managing patients with BPH disease who are considering enucleation surgery.
Our primary objective was to identify the incidence of prostate cancer identified by HoLEP in men with no history of prostate cancer. In addition, we sought to determine preoperative variables that can be used to predict the presence of prostate cancer in men undergoing HoLEP and to examine the burden of prostate cancer disease in this at-risk patient population.
Patients and Methods
A retrospective analysis of patients who underwent HoLEP at the IU Health Methodist Hospital between 1998 and 2013 was performed. Patients with a prior history of prostate cancer diagnosis were eliminated from the analysis (n=34). Preoperative data, including age, PSA, transrectal ultrasonography (TRUS) of prostatic volume, and PSA density, were collected. In addition, postoperative data, including final specimen weight and pathological tissue findings, were recorded. Patients without preoperative PSA were eliminated (n=221). Patients with elevated PSAs (at the referring urologist's discretion) had negative preoperative prostate biopsies. Prostate volume as assessed by TRUS was identified for 76% of patients. The PSA density was calculated from preoperative PSA and TRUS prostate volume and was available for 75% of patients. We acknowledge that the likelihood of identifying prostate cancer may vary between patients with a history of TRUS biopsy and those without; however, to the extent of our documentation, the detection of cancer at the time of HoLEP did not vary between patient populations (p=0.314).
HoLEP was performed in similar manner to our previously described technique. 12 Briefly, using a 550-μm end-firing laser fiber through a 28F continuous flow resectoscope, the transition zone of the prostate was completely enucleated. Next, using a Lumenis morcellator (Yokneam, Israel), morcellation was completed removing the excised tissue from the bladder and prostatic fossa. The entire HoLEP specimen was submitted for pathologic analysis by dedicated genitourinary pathologists.
The relationship between pre- and postoperative variables and identification of the presence of prostate cancer was assessed using univariate and multivariate logistic regression models. A separate multivariate logistic regression model was performed on patients with prostate cancer to evaluate the relationship between preoperative variables and Gleason 7 or higher disease. The variables chosen for univariate analyses were age, preoperative PSA, preoperative TRUS volume, final weight of prostate specimen from HoLEP, and percent of prostate resected. For multivariate analyses, only age, preoperative PSA, and the HoLEP specimen weight were included. As TRUS volume was not available for 24% of patients, we chose to use the HoLEP specimen weight in the analysis as it was available for 97% of patients. Patients with missing data were excluded from the regression analyses. All statistical analyses were performed using Stata version 12.1 (Stata Corp. LP, College Station, TX). In all tests, a two-tailed significance level of p<0.05 was used. Institutional Review Board approval was granted for the conduct of this study.
Results
Patient preoperative and postoperative characteristics are demonstrated in Table 1. A total of 1272 patients undergoing HoLEP between 1998 and 2013 were analyzed. One hundred three (8.1%) patients had prostate cancer identified on final pathological prostatic tissue analysis. Average pre-HoLEP PSA was 7.2 ng/mL (range: 0.04–121). Of note, two patients had pre-HoLEP PSA values higher than 65 ng/mL in the benign group (120, 121 ng/mL). Both patients presented with retention and prostatitis before HoLEP. Average volume resected during HoLEP was 78.9 g (SD: 53). The mean percent prostate tissue resected was 84%, which varied between 77% for the patients with prostate cancer and 85% among the nonmalignant cases. Patients with prostate cancer identified on final pathological analysis were older, had higher preoperative PSA, smaller preoperative TRUS prostatic volume, and smaller HoLEP specimen weight (Table 1). The length of stay was similar between the two groups.
p-Value represents Pearson's chi-squared test or the Mann–Whitney test.
Two patients in the benign group had pre-HoLEP PSAs higher than 65 ng/mL. Both of these patients were admitted with retention and prostatitis.
TRUS volume not available for 24% of cases, PSA density not available for 25% of cases.
HoLEP=Holmium laser enucleation of the prostate; PSA=prostate-specific antigen; SD=standard deviation; TRUS=transrectal ultrasonography.
Prediction of prostate cancer
On univariate logistic regression analysis, age and preoperative PSA were significantly associated with increased odds of identifying prostate cancer on final pathological analysis after HoLEP (Table 2). The weight of the HoLEP specimen was associated with decreased odds of prostate cancer identification in the HoLEP specimen (Table 2). On multivariate logistic regression, the age, preoperative PSA, and decreasing specimen weight remained significantly associated with the presence of prostate cancer (Table 2). Figure 1 depicts the relationship between age and identification of prostate cancer when adjusting for preoperative PSA and HoLEP specimen weight. Patients who were 80 years of age were at 20% predicted probability of having prostate cancer identified on HoLEP (<0.001).
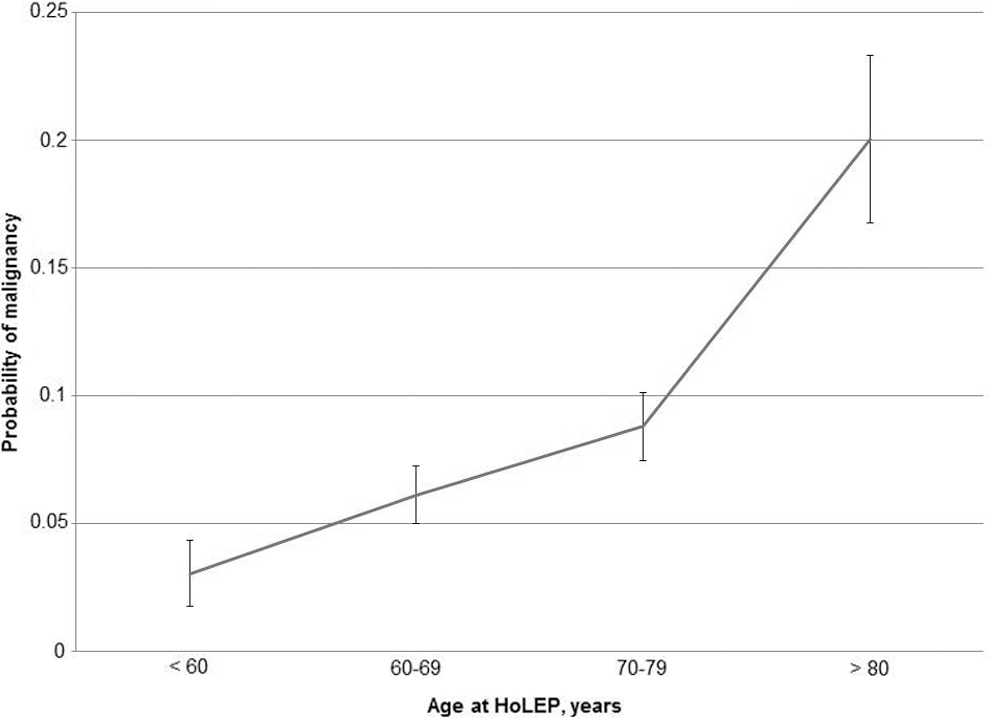
Predicted probability of prostate cancer by age.
Prediction of Gleason 7 or higher prostate cancer
Of the 103 patients with prostate cancer, 80 were Gleason 6 or less (78%), 14 were Gleason 7 (12 Gleason 3+4; 2 Gleason 4+3), and 9 were Gleason 8 or higher. Univariate regression results are shown in Table 3. On multivariate logistic regression, increasing preoperative PSA was associated with increased odds of Gleason 7 or greater prostate cancer (p=0.002) (Table 3).
Among the 103 patients identified with prostate cancer on HoLEP, follow-up information was available for 48. Thirty-five of 48 patients (73%) were followed with active surveillance and had received no treatment for their diagnosed prostate cancer at last follow-up. Twelve of the 48 patients (25%) underwent some form of primary therapy: 7 received external beam radiation, 3 underwent radical prostatectomy, and 2 received hormonal therapy. One patient with advanced disease underwent bilateral orchiectomy. A total of three patients from this cohort had developed metastatic prostate cancer. At last follow-up, three patients from the surveillance cohort had died of nonprostate cancer-related causes, while two men with metastatic disease in the intervention cohort had died.
Discussion
Prior reports have identified the majority of prostate cancer in analyzed HoLEP tissue to be primarily a low-grade, indolent disease that has not required subsequent intervention. A recent study by Rivera and colleagues suggested that more than 90% of patients found to have prostate cancer at the time of HoLEP were managed effectively with active surveillance. 13 Previous authors have reported a strong correlation between preoperative PSA and TRUS volume. 9,14 Similar to simple prostatectomy for BPH, the PSA values drop dramatically following HoLEP 14,15 and subsequent increases in PSA-velocity are associated with increased risk of prostate malignancy. 9 The PSA kinetics of patients discovered to have prostate cancer after HoLEP have not been well studied, although it would be reasonable to hypothesize that increases in PSA in this patient population may represent disease progression as the primary PSA producing transition zone has been completely eliminated. In our study, preoperative PSA was the only variable associated with intermediate- and high-grade prostate cancer and it was significantly higher in the prostate cancer than benign cohorts. As demonstrated in Figure 1, men older than 70 years with smaller prostates were at the greatest risk of harboring prostate cancer and may warrant further workup before HoLEP.
A recent study by Zlotta and colleagues found that 40% of the men older than 60 years and nearly 60% of men older than 80 years had prostate cancer on autopsy specimen. 16 Over 40% of the prostate cancer identified in this older group was found in the transition zone, which is the primary prostatic tissue removed during HoLEP. 16 These results contrast with our finding of only 8% incidental prostate cancer in our HoLEP patients. Despite this discordance, low rates of prostate cancer in HoLEP specimens was recently reported by Rivera and colleagues who cited a 13% cancer rate among their HoLEP patients. 13 Differences in comparison with historical autopsy series may be at least partially attributable to the vast majority of HoLEP patients having regular PSA checks or, in some cases, preoperative prostate biopsies. Prior publications have suggested an association between BPH and prostate cancer that may be inflammatory mediated, even suggesting that the presence of BPH may increase the risk of malignancy. 17 In contrast, our results suggest a potentially protective effect of BPH and obstructive symptoms on the presence of prostate cancer. Whether this represents a true cause and effect phenomenon or merely isolating a prescreened patient population remains unknown. In any event, future research exploring the relationship between BPH and prostate cancer should be considered.
It is well established that the risk of prostate cancer increases with age. Because BPH is the primary contributor to PSA rise and, as previously discussed, BPH may impact the incidence of prostate cancer, the relationship of prostate cancer in aging men with BPH is less understood. Despite the fact that we report a significant increase in the adjusted odds of prostate cancer detection for each decade of life over 60 (Fig. 1), we did not find an association between age and Gleason score. Although the relationship between age and prostate cancer was anticipated based on prior research, it does provide valuable support that the relationship between prostate cancer and age remains present even in men with coexisting BPH and obstructive symptoms, although it does not appear to impact the clinical significance of malignancy.
Unlike the positive association between age and the presence of prostate cancer, the relationship between prostate size and prostate cancer has previously been shown to be inverse. 18 Similar to prior findings, our cohort again demonstrated a decrease in the odds of prostate cancer identification as the prostate gland size increased beyond 30 g. Prior studies have hypothesized that the seemingly protective effect of larger glands harboring prostate cancer may be hormone mediated or related to a longer time before a nodule penetrates the prostate capsule. 19 In addition, preoperative PSA, TRUS volume, and PSA density were all significant on univariate analysis. These findings suggest that prostate volume and PSA density may be important predictors of the presence of prostate cancer in men with BPH undergoing HoLEP and that these tests should be considered before surgery, particularly in men with higher risk of prostate cancer detection.
Although the limitations of PSA are well documented, PSA continues to be widely used as both a screening tool and a method of detecting prostate cancer recurrence. 20,21 Our results suggest that there is value in obtaining a PSA preoperatively for men with BPH who are scheduled to undergo HoLEP. All patients with an elevated PSA should be considered for prostate biopsy or repeat prostate biopsy before surgery. If localized prostate cancer is identified before HoLEP, some of these men may elect to pursue alternative procedures to address both BPH and prostate cancer concomitantly.
Predicting the biologic behavior of prostate cancer found at HoLEP remains challenging. As documented in the past on autopsy and whole-mount tissue studies, typically only 20% to 40% of prostate cancer originates in the prostate transition zone. 16,22 Therefore, our data may be underrepresenting the true incidence and volume of disease present and is in no way a perfect surrogate for predicting prostate cancer-related risk. Despite this, interpretation of our results does allow us to make relevant observations regarding prostate malignancy in patients with BPH undergoing complete transition zone enucleation: (i) HoLEP candidates who are older men with small glands are more likely to harbor cancer in their enucleated tissue. More specifically, independent of PSA and specimen weight, an estimated 20% of men who are at least 80 years old will have prostate cancer identified on HoLEP specimens; (ii) the number of patients with prostate cancer in this cohort is low (<10%) with a predominantly low-grade disease; and (iii) preoperative PSA may be predictive of both the presence and aggressiveness of disease. Significantly, we have limited follow-up for our patients who were identified with prostate cancer on HoLEP, as only 48 of the 103 continued to receive care at our institution. As we are a tertiary referral center, this is not unexpected; however, it does limit conclusions that can be drawn regarding the prognosis of patients diagnosed with prostate cancer from HoLEP specimens.
The majority of patients were outside referrals and cancer management was often directed by the referring provider and not captured in our database. For our internal HoLEP patient population diagnosed with prostate cancer, a general discussion of options was standard. Patients with low-risk disease were recommended surveillance with a baseline PSA at 6 weeks, followed by serial PSA checks and digital rectal examinations every 6 months. Patients with a rising PSA or an abnormal examination were offered restaging TRUS biopsy and then treatment if indicated. Patients with intermediate- and/or high-risk disease post-HoLEP were staged appropriately and then offered definitive management, surgery versus radiation (external beam or IMRT) versus radiation and androgen deprivation typically without restaging biopsy.
Ultimately, the creation of a treatment and surveillance algorithm for managing this patient population based on numerous preoperative variables is warranted. Similar treatment flowcharts for prostate cancer and non-HoLEP-related BPH procedures are well documented. 23 Future studies that evaluate PSA kinetics in patients with prostate cancer identified by HoLEP will aid in determining appropriate follow-up recommendations for this unique population. In our population of post-HoLEP patients with negative final prostate pathology, we anticipate PSA levels to fall below 1. If levels do not nadir below 1 or rise quickly in follow-up, we recommend repeat TRUS prostate biopsy as suspicion for prostate cancer is high. In the present study, our data offer potentially useful counseling data for patients before HoLEP regarding the risk of prostate cancer being identified, as well as predicting higher risk disease in this patient population.
Our study has inherent limitations. It is retrospective and the number of prostate cancer patients is relatively low. In addition, because a high percentage of our patients are referred from outside facilities, preoperative TRUS techniques likely demonstrated interoperator variability and TRUS volume was missing for a significant proportion of patients. Because 24% of TRUS volumes were missing, we used HoLEP specimen weight in all of our analyses. Additionally, TRUS biopsy was not standardized among referring physicians and this variable was not completely captured in our database. As a tertiary referral center, some post-HoLEP patients are lost to follow-up and therefore information on prostate cancer treatment initiation was not available for the entire cohort. It is possible that a disproportionate number of patients who required subsequent therapy received follow-up at our institution, thus creating a selection bias in the descriptive findings that we present. Despite the stated limitations, our study represents one of the largest analyzed cohorts of prostate cancer in HoLEP patients.
Conclusion
The existence of incidentally detected prostate cancer at the time of HoLEP in men with BPH and obstruction is low and the majority of patients will have low-grade disease. Men older than 70 years with smaller glands are at the highest risk of harboring prostate cancer in their analyzed tissue. Optimal treatment and surveillance strategies for the management of men with prostate cancer after HoLEP need to be established.
Footnotes
Disclosure Statement
James E. Lingeman is a Consultant/Advisor, Meeting Participant/Lecturer for Lumenis. He is also a Consultant/Advisor, Investor, Meeting Participant/Lecturer for Boston Scientific Corp. No competing financial interests exist for all other authors.