
Abstract
Purpose:
To evaluate the efficacy of endoscopic combined intrarenal surgery (ECIRS) using retrograde flexible ureteroscopy and miniature percutaneous nephrolithotomy (PNL) for the treatment of patients with staghorn calculi in the prone split-leg position.
Patients and Methods:
We retrospectively reviewed the records of 42 patients with staghorn calculi (45.8±3.2 mm) who underwent ECIRS using retrograde flexible ureteroscopy and miniature PNL in the prone split-leg position for the treatment of staghorn calculi in our center between December 2010 and August 2013. A flexible ureteroscope with a laser fiber was inserted through a ureteral access sheath, and lithoclast lithotripsy was performed through a mini-percutaneous tract. Both procedures were performed simultaneously by two urologists. Surgical parameters, including surgical time, stone-free (SF) rates, modified Clavien complication grades, and risk factors for residual stones, were analyzed.
Results:
Fifteen patients (35.7%) had complete staghorn calculi. Among the 42 staghorn calculi treated, 23 had 0 to 5 stone branches, 14 had 6 to 10 stone branches, and 5 had ≥11 stone branches. All procedures were performed successfully using a single lithotripsy tract with the patient in the prone split-leg position. The mean surgical time was 143.2±9.2 minutes. The initial SF rate was 71.4%, and the final SF rate was 83.3% after further treatment. One patient required a blood transfusion (2.4%), but no patient experienced a ≥3 Clavien grade complication. Risk factors for residual stones were stone size, stone surface area, complete staghorn calculi, and the number of stone branches.
Conclusions:
ECIRS for staghorn calculi in the prone split-leg position is a safe, efficient, and versatile method for the effective management of staghorn calculi without the creation of multiple percutaneous tracts.
Introduction
S
Endoscopic combined intrarenal surgery (ECIRS) using retrograde flexible ureteroscopy (fURS) and PNL was developed as a single-step treatment for the removal of renal calculi to avoid the morbidity associated with the creation of multiple access points while still achieving a high stone-free (SF) rate. 7 –12 The Galdakao-modified supine Valdivia position is most commonly used for this procedure, because it enables quick patient positioning, reduced pressure in the renal pelvis (reducing the risk of fluid absorption), and convenient ureteroscopic access. 7,8 However, urologists are also familiar with the use of the prone position for PNL, as it provides a larger area for percutaneous renal access and a wide space for instrument manipulation. Some studies have reported the efficacy of the prone position in performing ECIRS. 10 –12
This study aimed at evaluating a new ECIRS technique that involved the simultaneous use of fURS and mini-PNL in the prone split-leg position (prone-ECIRS) for the treatment of staghorn calculi.
Patients and Methods
Preoperative evaluation
Between December 2010 and August 2013, 75 patients presenting with large calculi underwent ECIRS in the prone split-leg position (prone-ECIRS) at Toyota Kosei hospital. We retrospectively reviewed and analyzed the records of 42 patients with staghorn calculi. This study was approved by the institutional review board of Toyota Kosei Hospital. Written informed consent was obtained from all patients, and all patients completed a minimum follow-up period of 3 months. Patients who were eligible for inclusion were those with complete or partial staghorn calculi who were candidates for PNL surgery as the primary indication based on EAU and AUA guideline. Treatment of patients was based on the presence of symptoms of flank pain, hematuria, and/or urinary tract infection. Patients were excluded for the following reasons: age <18 years, inability to understand informed written consent, severe ureteral stricture, suspected pregnancy, and American Society of Anesthesiologists classification of physical status grade ≥3. Preoperative patient evaluation included a clinical examination and routine laboratory tests. Preoperative imaging, including plain abdominal radiography, ultrasonography, and computed tomography (CT), were used to determine the location, size, and radiodensity of the stones, as well as the number of stones branching into minor renal calices. Stone branch number represents the number of renal calices occupied by stones extending from the renal pelvis. If CT could not provide adequate information regarding the spatial structure of calculi to determine stone branch number, excretory urography was performed. Size was defined by the longest stone diameter observed during preoperative imaging. Stone surface area was estimated using the formula described by Tiselius and Andersson (length×width×3.14×0.25). 13 We performed preprocedural urine cultures as a part of the protocol, and revised antibiotic therapy based on the results of the urine culture. If the urine culture was negative, we administered cefazolin before and for 2 days after the procedure. Patient characteristics and stone features are summarized in Table 1.
Hb=hemoglobin; Hct=hematocrit; SD=standard deviation.
Surgical techniques
The patient was oriented in the prone split-leg position during the procedure, enabling both retrograde and antegrade access (Fig. 1a). Flexible cystoscopy was performed to locate the ureteral orifice, which was easily observed with the patient in the prone position. Under fluoroscopic guidance, the ureteral orifice was cannulated with a 0.035-mm guide wire that was passed into the upper urinary tract, while a 12-F/14-F ureteral access sheath was inserted to enable frequent passage of the ureteroscope (Flex X-2®; Karl Storz, Tuttlingen, Germany) to the renal calculi sites.
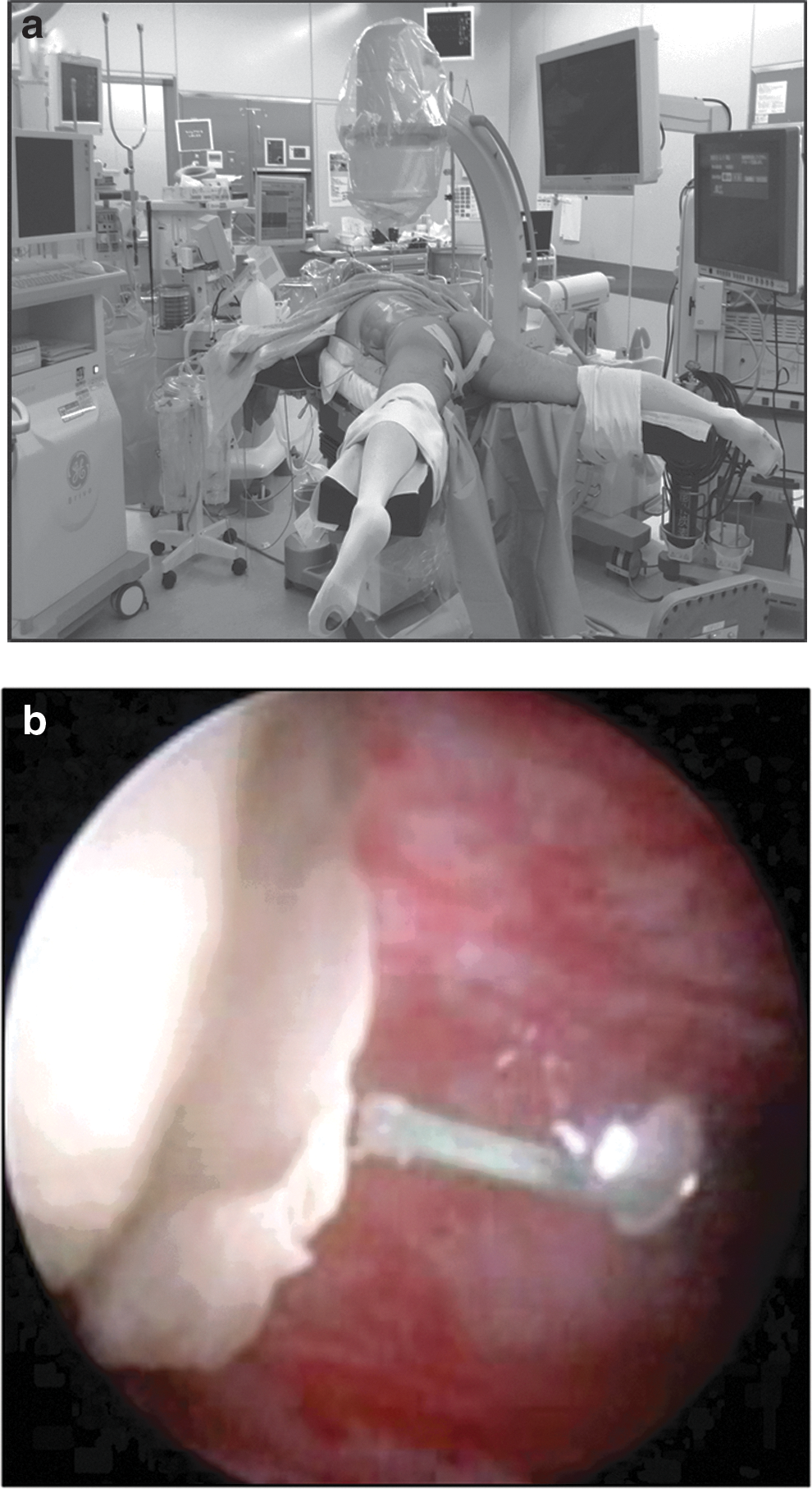
Two urologists worked simultaneously to fragment the staghorn calculi. One performed retrograde intrarenal surgery (RIRS) using a Holmium-YAG laser with a ureteroscope through a ureteral access sheath. A single action pumping system (SAPS; Boston Scientific Japan, Tokyo, Japan) was used for controlled irrigation during RIRS. A 200- or 365-μm YAG laser fiber was used in conjunction with fURS to fragment the renal calculi. The commonly used laser settings were 0.5 to 1.0 J at 5 to 10 Hz. The other urologist performed PNL using lithoclast lithotripsy (Boston Scientific Japan) through 18-F (or 19.5-F) mini-PNL tracts (Karl Storz) as previously described (Fig. 1b). 10 Stones were broken into fragments using a lithoclast, and smaller fragmented stones were washed through the mini-PNL tract by retrograde irrigation without the use of stone baskets. At the end of the procedure, the urinary tract was stented with a 4.7-F Double-J ureteral stent and an 18-F nephrostomy tube. The nephrostomy tube was removed 2 days postoperatively, and the ureteral stent was removed 1 month later.
Postoperative evaluation
Laboratory tests, including tests for hemoglobin and hematocrit levels, were performed at baseline and the day after surgery. The SF rate was determined at 3 months posttreatment by plain abdominal radiography, renal ultrasonography, or CT. The SF status was defined as the absence of residual fragments measuring <4 mm in diameter. Complications were graded according to the modified Clavien classification, 14 and fever was defined as a body temperature of >38.5°C.
Statistical analysis
Continuous data were recorded as the mean±standard deviation and analyzed using Student's t-test and chi-square tests. A value of p<0.05 was considered statistically significant.
Results
Stone features
Stone features are summarized in Table 1. The mean stone size was 45.8±3.2 mm, and the mean stone surface area was 1074.0±132.7 mm2. Fifteen patients (35.7%) had complete staghorn calculi. The mean radiodensity of the stones was 1031.2±46.2 HU. Among the 42 staghorn calculi treated, 23 had 0 to 5 stone branches, 14 had 6 to 10 stone branches, and 5 had ≥11 stone branches.
Surgical data
Surgical parameters are summarized in Table 2. All procedures were successfully performed using only a single tract with the patient in the prone split-leg position. The mean surgical time was 143.2±9.2 minutes, and the mean hospital stay was 6.8±0.5 days. The mean decreases in hemoglobin and hematocrit levels were 1.14±0.15 g/dL and 3.9%±0.5%, respectively.
PNL=percutaneous nephrolithotomy; SWL=extracorporeal shockwave lithotripsy.
Complete stone clearance after a single prone-ECIRS treatment session was achieved in 30 patients (71.4%). Nine patients required ancillary treatments with SWL (n=5), fURS (n=2), or PNL (n=2). The final SF rate, including those who underwent ancillary treatment, was 83.3% (n=35).
Univariate analyses for factors affecting the SF status after PNL monotherapy are summarized in Table 3. Risk factors for residual stones were stone size, stone surface area, complete staghorn calculi, and number of stone branches.
SF=stone-free.
Complications
The overall complication rate was 21.4%. The Clavien grades and the type of complications are summarized in Table 4. Four patients experienced transient fever during the first two postoperative days (which promptly resolved with specific broad-spectrum antibiotic therapy), and three patients experienced urinary tract perforation. One patient required blood transfusion; however, no injury to neighboring organs, acute or delayed kidney injury, or anesthesiological complications were noted. None of the patients had complication of Clavien grade ≥3.
Discussion
Since the first report of PNL for the treatment of staghorn calculi by Clayman et al. in 1983, 15 there has been significant improvement in PNL techniques and instrumentation. PNL has become the gold standard technique for the management of staghorn calculi. The goal of treatment is to achieve an SF status with minimal morbidity.
The SF rate of 71.4% in our study was higher than the 56.9% reported by Desai et al. in their series of 1446 cases 4 or the 56.6% SF rate reported by El-Nahas et al. in their series of 251 cases. 16 The identified risk factors for residual stones were almost related to stone characteristics, including stone size, stone surface area, staghorn status, and the number of stone branches (Table 3). Recently, staghorn calculi with more than five stone branches have been reportedly found to be associated with a lower rate of stone clearance and a longer hospital stay. 17 Generally, these problems can be overcome through the extensive use of flexible nephroscopy and multiple-tract PNL; however, these techniques are not always efficacious. In addition, the creation of multiple tracts can increase the incidence of bleeding complications. 6
The AUA Nephrolithiasis Clinical Guidelines Panel on staghorn calculi reported complication rates of 7% to 27% and a transfusion rate of approximately 18% for PNL. 1 The overall complication rate in our study was 21.4%, and the transfusion rate was 2.4%. The mean decrease in the hemoglobin level was low in our series.
Our newly developed combined technique, prone-ECIRS using mini-PNL combined with retrograde fURS, resulted in the use of a single percutaneous tract with a high single-step SF rate and minimal complications. This procedure provided the following advantages: (1) efficient stone fragmentation by simultaneous antegrade-retrograde lithotripsy; (2) better visibility with retrograde irrigation that enabled removal of small stone fragments easily through the PNL tract; (3) fragmentation of previously inaccessible stones (e.g., in a calyx next to the PNL tract [Fig. 2]) with minimal movement of the PNL tract through the use of ureteroscopy, reducing the risk of renal parenchymal bleeding; and (4) a reduced risk of bleeding with the use of a mini-tract for lithotripsy. In this study, an 18-F or 19.5-F mini-PNL tract was used instead of the conventional 30-F PNL tract. Mini-PNL can be performed with a tract size of 16F to 20F, and it is associated with reduced procedure-related morbidity. 10,18 However, this technique has several disadvantages, including low therapeutic efficacy for the removal of large stones due to diminished intraoperative field visibility and increased surgical time. 10,19 In this study, simultaneous use of antegrade and retrograde devices compensated for this limitation of mini-PNL by increasing the efficiency of fluid irrigation during stone removal and reducing the number of residual stones.

A schema of endoscopic combined intrarenal surgery (ECIRS) using mini-percutaneous nephrolithotomy (PNL) combined with retrograde fURS. Retrograde fURS fragments stones that were inaccessible via the rigid nephroscope (e.g., a calyx next to the PNL tract) and reduce excessive movement of the PNL tract, thereby reducing renal parenchymal bleeding.
The Galdakao-modified supine Valdivia position is a more common approach for the simultaneous use of fURS and PNL. 7 –9 In 1988, Bagley used a modified prone position for nephroscopic and ureteroscopic procedures in female patients. 20 Five years later, a prone split-leg position with simultaneous antegrade and retrograde endoscopy using a two-team approach was reported. 21 However, to our knowledge, the effectiveness of the prone split-leg position in treating renal calculi has not previously been examined, and urologists are not currently familiar with the use of this position during ECIRS. The supine position is advantageous, because it requires less time for patient positioning, reduces pressure on the renal pelvis, and enables easier ureteroscopic access. It also helps prevent cardiovascular, respiratory, neuroendocrine, and pharmacokinetic anesthesia problems typical of the prone position, particularly in obese patients. 22 However, the supine position may have some disadvantages, including smaller range of potential access angles. 23 In the modified Valdivia position, the kidney is hypermobile, which appears to increase the risk of renal puncture, making guide wire manipulation more difficult.
The prone position for PNL is familiar to urologists and provides a larger area for percutaneous renal access and more space for instrument manipulation. For obese patients and those with staghorn calculi, prone PNL is associated with shorter surgical time and slightly better SF rates than supine PNL. 24,25 The prone position is also associated with significantly reduced nephrostomy tract length and more potential access sites, which may improve the ease and safety of PNL. 23 In addition, we previously reported that the normally curved ureter between the orifice and the ureteropelvic junction straightens when the patient is in the prone position based on three-dimensional helical CT results. RIRS in the prone position enables easy access of the ureteral sheath to the renal pelvis similar to the supine position approach without major problems. 11 Similar to the Galdakao-modified supine Valdivia position, prone-ECIRS is effective for the removal of large renal stones.
A major limitation of this study was that it was a retrospective review. Further studies are needed to compare the effectiveness of prone ECIRS to the standard technique of multi-tract PNL. In addition, there are several potential drawbacks to this procedure such as the need for two surgeons, increased cost (access sheath, laser, etc.), increased instrumentation needs (two monitor, laser system, etc.), and the risk of complications from ureteroscopy compared with a standard PNL without retrograde access.
Conclusions
Prone ECIRS is a safe, efficient, and versatile procedure that often provides complete resolution of staghorn calculi in a single step without multiple PNL tracts. This promising new technique represents a significant improvement in the treatment of patients with staghorn calculi.
Footnotes
Acknowledgments
The authors would like to thank K. Ichikawa and M. Noda for secretarial assistance, including data input and data analysis.
Disclosure Statement
The authors declare that they have no competing interests.