
Abstract
Background and Purpose:
Urology practices frequently encounter individuals who experience various degrees of pain/discomfort after ureteral stent removal. These symptoms have been previously proved to greatly affect functionality, convalescence time, quality of life, and healthcare costs. The etiology is unclear, but the condition is often self-limiting. We counsel individuals on their risk of having post-ureteral stent removal pain based on anecdotal data. We sought to evaluate the incidence of post-ureteral stent removal pain and attempt to find the probable cause.
Patients and Methods:
All individuals who had a ureteral stent placed and subsequently removed for various etiologies (between January 2012 and May 2013) were evaluated by filling a survey conducted by a member of the healthcare team 1 to 3 weeks after ureteral stent removal. Univariate and multivariate analysis were used to assess correlation between demographics, operative procedures, convalescent time, and post-ureteral stent removal symptoms. All statistical analyses were performed using SAS® software, and a P value of less than 0.05 was considered to indicate statistical significance.
Results:
Of the 104 individuals in the final cohort, 64% had symptoms after stent removal (pain, hematuria, frequency, urgency, or fever), and among those with symptoms, 60% experienced pain/discomfort. On univariate analysis, stone basketing and indwelling stent discomfort correlated positively with pain after stent removal. On the other hand, the use of anticholinergics and a longer indwelling stent duration were associated with less pain after stent removal. On multivariate analysis, correlation with procedures involving basket extraction and indwelling stent discomfort maintained significance.
Conclusion:
Our series suggests that two of three individuals who undergo ureteral stent removal experience symptoms thereafter. Individuals undergoing stone basket extraction and those who experienced stent discomfort were more likely to have pain after stent removal. Anticholinergic use and stents indwelling for a longer time were associated with less pain after stent removal.
Introduction
U
The symptoms associated with indwelling ureteral stents include, but are not limited to, urinary frequency, urgency, hematuria, and flank pain. 2,4 Trigonal irritation by the intravesicular portion of the stent and the pressure transmitted to the renal pelvis during micturation have been postulated as important factors in these symptoms. 5 The side effects have been well documented in the literature and, in fact, are the focus of a validated metric, the Ureteral Stent Symptom Questionnaire, a self-administered questionnaire addressing six domains of stent-related malaise including urinary symptoms, body pain, general health, work performance, sexual matters, and additional problems. 6
For all the knowledge attained regarding stent-associated symptoms while in situ, data regarding symptoms after its removal are very limited. To our knowledge, only one study has exclusively evaluated symptoms (pain) after stent removal. 7 This study, however, evaluated only 22 individuals, half of whom were given a non-steroidal anti-inflammatory drug (NSAID) to help mitigate such symptoms. Without baseline knowledge of incidence and severity of such post-stent removal symptoms, however, such a study is very limited. Hence, we report our experience with symptoms after ureteral stent removal, including incidence, severity, possible associations with certain procedures, and symptoms while the stent was indwelling.
Patients and Methods
General
A phone survey was designed by an experienced practitioner and conducted with the intent to evaluate the incidence and possible associations related to symptoms after stent removal. This survey was administered by a member of the healthcare team from January 2012 to May 2013. All individuals who underwent ureteral stent placement (imperative or prophylactic) and subsequent removal (either by attached string or cystoscopic retrieval in the office) by one of three surgeons (JM, AS, and ZO) were offered to participate in the survey during stent removal, and those who wanted to were encouraged to closely monitor symptoms and their timing. All the individuals were contacted within 1 to 3 weeks after stent removal.
Procedure/technique
All ureteroscopies were performed by urologists skilled in semirigid and flexible ureteroscopy, with two of the urologists having specialty training in endourology (AS, ZO). The ureteroscopic technique used included cystoscopy with safety wire placement and retrograde pyelography. For ureteral stones, semirigid ureteroscopy alongside a safety wire was performed and if unable to safely advance to the ureteral stone, then a flexible ureteroscope was used. If relatively few ureteral passes with the ureteroscope were anticipated, then no ureteral access sheath was placed. When multiple passes were anticipated, then a ureteral access sheath was used, the size of which was left to surgeon discretion. Small stones relative to a given individual's ureter were removed with a stone basket alone, without fragmentation. Impacted stones and those considered too large for simple basket extraction were fragmented with the holmium:yttrium-aluminum-garnet laser. Stone dusting vs stone fragmentation with basket extraction was left to the judgment of the surgeon.
Cohort
Of 137 individuals who were approached for the survey, 113 (82%) responded to the phone questionnaire (Appendix 1) within 3 weeks of ureteral stent removal. Individuals (9) with chronic indwelling stents (>30 days) or those needing interval stent exchanges were excluded, making a total of 104 individuals in the study cohort.
Survey
The questionnaire (Appendix 1) collected the following information: in situ stent symptoms, method of stent removal, symptoms after stent removal, medication use and hospital readmission. All reported symptoms after stent removal such as hematuria, flank discomfort/pain, frequency, urgency, fever, were subjectively graded by the participants who completed the phone survey. The time interval between stent removal and onset of these symptoms was recorded and categorized as either “immediately,” “within a few hours,” “after half a day,” “after 1 day,” “after few days,” or “after 1 week.” Furthermore, the duration for these symptoms to subside or resolve was categorized as either “less than a few hours,” “more than half a day,” “more than 1 day,” “more than few days,” or “more than 1 week.” Other parameters such as return to activity, medication use, and hospital admission were also recorded (Appendix). The survey data were then tabulated and reviewed.
Statistical analysis
The data set was stratified by the presence or absence of pain after removal of the ureteral stent. Individuals (4) whose in situ and/or post-stent removal parameters (frequency and urgency) could not be assessed because of confounding factors (presence of an ileal conduit, Foley catheter, and chronic preexisting back pain) were excluded from their respective analysis. Univariate analysis (Tables 1 and 2) was performed to assess the correlation between pain after stent removal and perioperative parameters. Kruskal-Wallis test and Fisher exact tests were used for continuous and categorical variables, respectively. Multivariate analysis was conducted to identify the variables most independently predictive of pain after stent removal. A P value of less than 0.05 was considered to indicate statistical significance. All statistical analyses were performed using SAS® Software version 9.3.
In the presence of rigid or flexible ureteroscopy.
Any procedure other than those listed above.
Two individuals were excluded from the analysis because of the presence of post-ileal conduit (1) and use of a Foley catheter for 1 week after stent removal (1).
Median (interquartile range) and number (percentages) are used to describe continuous and categorical variables, respectively.
OR=odds ratio; CI=confidence interval.
Two individuals were excluded from the analysis due to the presence of post-ileal conduit (1) and use of a Foley catheter for 1 week after stent removal (1).
Nonsteroidal anti-inflammatory drugs, acetaminophen, narcotics, anticholinergic, alpha blocker, or antibiotics.
One patient was excluded from analysis because of preexisting chronic back pain.
Within 30 days of admission (emergency department or clinic).
Abdominal radiography, abdominal ultrasonography, computed tomography, or magnetic resonance imaging.
Results
Baseline characteristics
The baseline characteristics of the final cohort (104 individuals) and the procedures undergone are presented in Table 1. There were a total of 64 men and 40 women with an overall median age of 60 years.
Indication for procedure
Our cohort was stratified into those who had stents placed for stone disease (74%) and those who had a stent placed for indications other than stone disease (26%) including diagnostic ureteroscopy for hydronephrosis, ureteral strictures, and hematuria evaluation. We found no correlation of post-stent symptoms between procedures performed for stone disease and non-stone disease (P=0.496) (Table 1).
Type of procedure/technique
All individuals underwent a combination of procedures (Table1) before insertion of the ureteral stent. The most common procedures were stone basket extraction (64%), semirigid ureteroscopy (57%), and flexible ureteroscopy (52%). On univariate analysis, only the use of the basket during ureteroscopy was significantly associated with more symptoms after stent removal.
In situ symptoms
The ureteral stent was in situ for a median duration of 6 days. There were 101 (97%) individuals who experienced various symptoms while the stent was in situ; specifically, 82 (79%), 79 (76%), 71 (68%), 67 (64%), and 21 (20%) experienced urgency, frequency, discomfort/pain, hematuria, and incontinence, respectively (Table1). Of the 71 individuals who experienced discomfort or pain, the median pain score was 4 (on a scale of 0–10). The location of discomfort was most commonly reported at the “bladder and back” (34%). The timing of pain was more “during voiding” (52%) than “with movement” (13%). Apart from the back and bladder, men reported pain at the “tip of their penis” (13%) and women reported pain at the “vagina” (4%). On univariate analysis, only in-situ discomfort was predictive (odds ratio [OR]=2.66) of pain after stent removal (P=0.047). Certain individuals (36) were administered an anticholinergic agent for the duration of the indwelling stent as prophylaxis for stent discomfort as per surgeon discretion. These individuals were found to experience less post-stent removal pain (P=0.005) (Table1).
Stent removal
The ureteral stent was removed either by pulling on the attached string (59%) or cystoscopic retrieval in the office (41%) (Table 2). Overall, 23 (20%) individuals experienced pain during stent removal. Of those who underwent stent removal by string, 46% (28/61) experienced pain after stent removal compared with only 28% (12/43) among those who underwent stent removal by cystoscopy. Although not significant (P=0.06), the cystoscopy method had a negative correlation (OR=0.45) with pain after stent removal.
Symptoms after stent removal
In our cohort, 67 (64%) individuals experienced symptoms after ureteral stent removal. Although multiple symptoms may have occurred in an individual, the distribution of symptoms was 45 (43%), 40 (38%), 15 (16%), 14 (14%), and 8 (8%) for hematuria, pain, frequency, urgency, and fever (Table 3). Among those affected, the median onset and duration of the symptoms were estimated as “immediately after the procedure” and “less than few days,” respectively (Table 3). Most of the individuals were able to return to normal activity either the “same day” (10%) or “next day” (42%) after the stent removal. Most of the individuals (70%) who had pain after stent removal took medications such as acetaminophen, NSAIDS, narcotic medications, anticholinergics, alpha blockers, and even antibiotics to relieve their symptoms. Overall, 5 (4%) individuals needed hospital readmission (for hematuria observation [4] and pain control [1]) and 15 individuals (14%) needed imaging studies. Univariate analysis showed a significant correlation between pain after stent removal and other post-stent symptoms such as hematuria (P=0.002), frequency (P<0.001), urgency (P=0.002), medication use after stent removal (P<0.001), and convalescent time (P<0.05) (Table 2).
Among those who had the corresponding symptom (one person may have more than one symptom); onset and duration are based on the responses to our questionnaire (Appendix).
Two individuals were excluded because of the presence of post-ileal conduit (1) and use of a Foley catheter for 1 week after stent removal.
Multivariate analysis
During multivariate analysis for predictors of pain after stent removal, all significant variables (on univariate analysis) before and until stent removal (“basket stone extraction procedure,” “in-situ stent discomfort,” and “anticholinergic agent during stent removal”) were included into a two-step backward-Wald model. As a result, “basket extraction procedure” (P=0.005) and “in-situ stent discomfort” (P=0.047) were found to be most predictive for pain after stent removal (Table 4).
Only variables before stent removal and those found significant on univariate analysis were used for this analysis.
In the presence of rigid or flexible ureteroscopy.
Discussion
Most, if not all urology practices deal with ureteral stents. Certainly, clinicians are well aware of the symptoms associated with an indwelling ureteral stent and their ramifications on functionality and quality of life. 2,3 Many stent characteristics have been evaluated in an attempt to decrease such indwelling stent symptoms with only stent location 8 (distal coil crossing midline) and use of metal mesh stents 9 (no distal coil) showing significance. While the in-situ stent symptoms are well studied and reported, very little is published on symptoms after stent removal. 7 The impetus for this survey was the anecdotal observation that a significant number of individuals in our practice experienced various symptoms after stent removal, irrespective of their seemingly uneventful clinical course. Fortunately, these symptoms were self-limiting. As a result, we began counseling individuals on the possibility of such symptoms, but found no recent literature to guide our advice.
Only recently has one other article been published regarding symptoms after stent removal. In this prospective, randomized, double-blind, placebo-controlled trial by Tadros and associates, 7 22 individuals were randomized to receive either a single dose of placebo or an NSAID (rofecoxib 50 mg) in the form of a cyclooxygenase-2 inhibitor just before stent removal. Fifty-five percent of individuals (6 of 11) in the placebo arm experienced severe pain (Visual Analog Scale score ≥7) compared with none in the treatment arm (up to 24 hours after stent removal). This well-conducted study, however, did not evaluate other symptoms associated with removal of the ureteral stent and is also limited by its small cohort size.
Our report is the second to evaluate symptoms after the removal of ureteral stents and the first to investigate their correlation with perioperative proceedings and in-situ stent symptoms. The incidence of pain after stent removal in our study was 38% (40 of 104) as opposed to 55% (6 of 11) in the study 7 mentioned above. This difference may be because of our larger cohort size. Our overall incidence of symptoms after stent removal (urgency, frequency, hematuria, or fever) was 63% (Table 3). From our data, “basket extraction procedure” and “in-situ stent discomfort” showed positive correlation, whereas a longer “stent duration” and the “use of anticholinergic agent” showed negative correlation with pain after stent removal. Only “basket extraction procedure” and “in situ stent discomfort” maintained significant association with pain after stent removal on multivariate analysis, however.
It is expected that individuals experiencing pain after stent removal will take longer to return to regular activities and take medications for relief of discomfort (Table 2). Medications that have been studied for in-situ stent pain include NSAIDs, narcotics, alpha 1 blocker, anticholinergics, and periureteral Botox injection with some degree of relief from symptoms. 10 –14 In our practice, we typically encourage hydration, offer NSAIDs, and or offer oral narcotics (e.g., oxycodone/acetaminophen) to individuals with stent-related or post-stent removal symptoms. Despite conservative outpatient management of these symptoms after stent removal, 5% and 14% of the individuals returned for readmission (four for pain and one for hematuria), and imaging studies to elucidate the potential source of symptoms. Three of the five individuals had residual stones; however, all five individuals only needed symptomatic management of symptoms and had no complaints thereafter. No patient needed return to the operating room for obstructing ureteral stone. To our knowledge, there are no data in the literature to compare with our readmission rate after stent removal.
While this information is quite worthwhile for the counseling of individuals who are about to undergo stent removal, several questions are raised by our findings. Perhaps such pain episodes are related to transient occlusion of the affected ureter, or whether this occlusion is caused by a self-limited ureteral spasm or by a small stone fragment in transit post-stent removal. Most of the individuals (74%) in our cohort had a stent placed after a definitive procedure for their “stone disease.” We speculated that the difference in the indication of the procedure may have contributed to the symptoms after removal. Analysis showed no correlation in symptoms (Table 1) after stent removal, however, between a procedure performed for stone disease and non-stone disease.
Kuehhas and colleagues 15 reported an equal perception of pain during removal of the stent by string or by rigid cystoscopy. It is possible that the use of a rigid cystoscope had contributed to their results. In fact, in our study, flexible cystoscopy-assisted stent removal (41%) had a lower likelihood (OR=0.45) of experiencing pain after stent removal compared with the string method (59%) (Table 2). This is an unexpected and interesting finding, because one would assume that additional instrumentation would contribute to more post-stent removal pain. On closer look (Fig. 1), however, we found that the median duration of stent in situ” for the cystoscopy and string cohort were 9 (interquartile range [IQR]: 7–13.5) and 4 (IQR: 3–6) days, respectively. Hence, we postulate that this negative correlation is because of a longer duration (P<0.05) between initial instrumentation and stent removal, which has probably given the ureter more time to accommodate the stent.
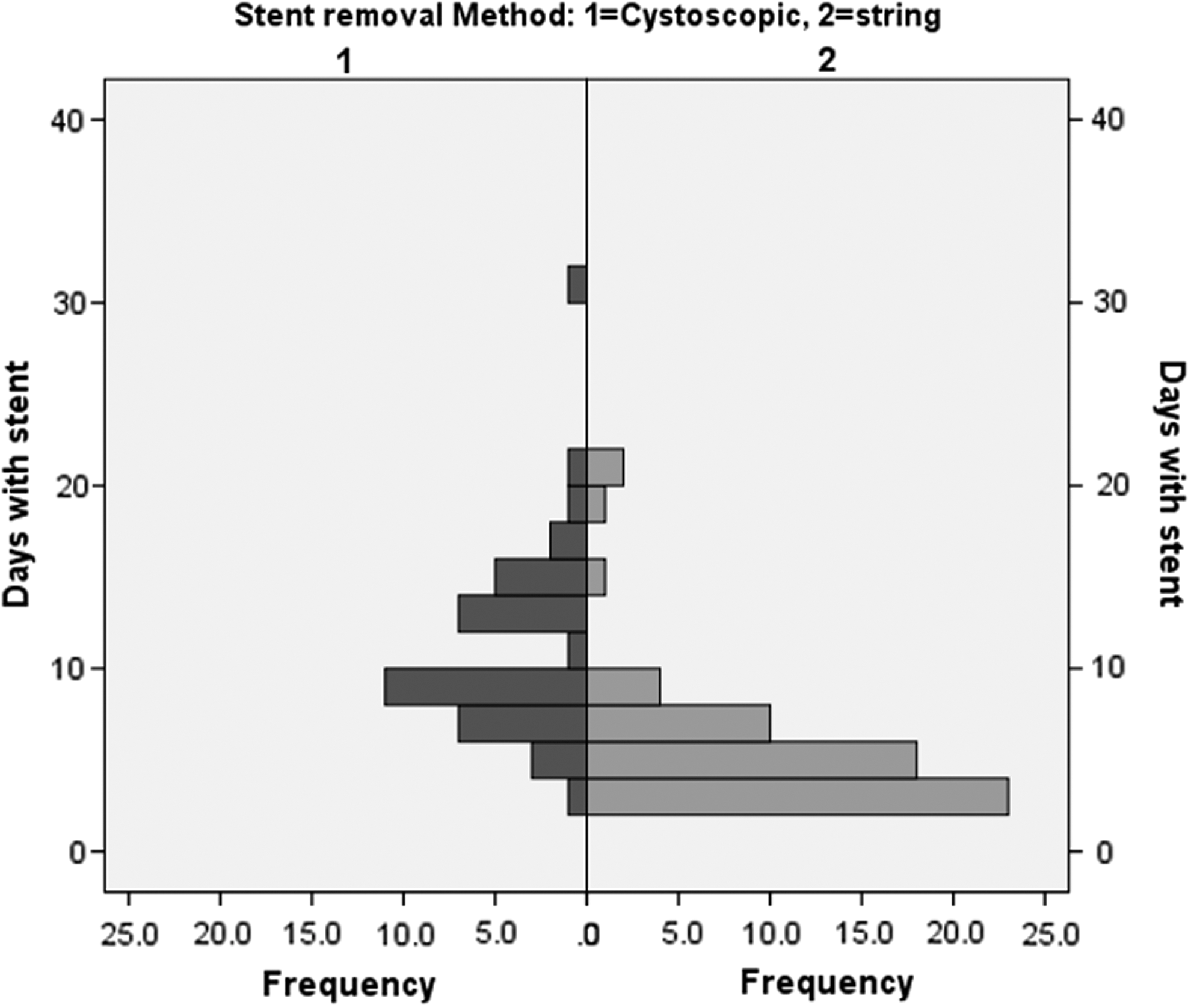
Stent removal method. 1=cystoscopic; 2=string.
To our knowledge, this is the first study that directly evaluates the distribution of symptoms after stent removal and predictors of pain after stent removal. The retrospective nature of our study and relatively small cohort size may be potential limiting factors. In addition, the subjective characterization of symptoms by individuals, using a phone survey may potentially introduce a recall bias. All individuals were counseled preoperatively on the post-stent removal symptoms and informed that a survey will be done after stent removal, however. The survey was then conducted within a short interval (<3 weeks) after the stent was removed when the individuals still have a clear recollection of their symptoms, thereby eliminating or minimizing recall bias.
Conclusion
Our series suggests that more than half the individuals experience symptoms after stent removal. While individuals undergoing basket extraction procedure (in the presence of rigid or flexible ureteroscopy) and those who experience discomfort while the stent is in situ have a higher likelihood of experiencing pain after stent removal, a longer stent duration and use of anticholinergics for the duration of the indwelling stent seems to reduce the likelihood. Individuals should be counseled about such pain after stent removal and reassured that return to baseline activity should be possible by the day after stent removal. This pilot study emphasizes the need for a larger cohort study to further investigate and explore the correlation between post-stent removal symptoms and perioperative parameters.
Disclosure Statement
No competing financial interests exist.