
Abstract
Objectives:
The study compared the transurethral resection in saline (TURis), transurethral vaporization in saline (TUVis), bipolar plasma enucleation of the prostate (BPEP), and open prostatectomy (OP) in a single-center, prospective, randomized controlled clinical setting exclusively involving large prostate patients.
Patients and Methods:
During a 4½ year enrollment period, 320 cases of prostate volume over 80 mL, maximum flow rate (Qmax) below 10 mL/second, International Prostate Symptom Score (IPSS) over 19, or urinary retention were included in the trial and equally randomized in the four study arms. Patients were assessed preoperatively as well as at the 1-, 3-, 6-, and 12-month follow-up checkups using the IPSS, quality of life (QoL) score, Qmax, postvoiding residual urinary volume (PVR), and prostate-specific antigen (PSA).
Results:
Similar preoperative parameters were established in the four series. OP and BPEP were characterized by resembling operating times, while TURis and TUVis displayed prolonged surgical durations. TURis emphasized a substantially decreased mean resected tissue weight. TUVis showed the lowest mean hemoglobin level drop, followed by TURis and BPEP (equivalent results) and finally OP (highest bleeding). OP described the longest mean catheterization period and hospital stay, followed by TURis, and afterward by TUVis and BPEP (similar data). During the follow-up period, statistically equivalent IPSS, QoL, Qmax, and PVR outcomes were established for OP, BPEP, and TURis. TUVis displayed significantly smaller Qmax improvements, but similar other functional features. Significantly lower mean PSA levels were determined secondary to OP and BPEP when compared to bipolar resection and subsequently to vaporization.
Conclusions:
OP and BPEP emphasized the highest surgical efficiency (prolonged postoperative recovery for OP), while TUVis displayed the lowest hemorrhagic risks. On the medium term, generally resembling functional outcomes were determined for the four techniques, with significantly decreased mean PSA values secondary to OP and BPEP.
Introduction
T
While monopolar transurethral resection of the prostate (TURP) was generally ruled out as a valid choice for this category of cases due to the high risk of TUR syndrome implied by the prolonged procedures, 5 bipolar electrosurgery largely benefited from the lack of operation time and prostate volume limitations. 6 In addition, this technology created the premises for a rather versatile endoscopic approach that was occasionally tailored to fit all three previously mentioned BPH therapeutic principles. 7
Bipolar TURP has been repeatedly outlined as a true competitor to the classical monopolar resection in light of the resembling efficacy and diminished blood loss. 8 Bipolar vaporization has been initially slow in gaining reliable scientific support, but it presently benefits from increasing popularity and the numerously emerging comparative trials. 9 Bipolar enucleation still remains an insufficiently assessed field of transurethral electrosurgery, awaiting more consistent clinical research to become available. 10 In any case, the three types of procedures are still far from reaching a worldwide acknowledgement as standard alternatives within the therapeutic armamentarium of large BPH cases. 11
To the best of our knowledge, the present analysis constitutes the first report analyzing the bipolar endoscopic resection, vaporization, and enucleation of high-volume prostates within a unitary clinical setting emphasizing a prospective, randomized controlled comparison to open surgery. The primary endpoint of this study was to provide an evidence-based parallel between the three types of techniques using the same cutting current and technological setup and the standard OP in terms of perioperative safety profiles, BPH tissue ablation capabilities, and medium-term functional outcomes.
Patients and Methods
Between January 2009 and May 2013, a total of 320 large prostate patients were enrolled in a single-center prospective randomized controlled trial and previewed for a 1-year follow-up evaluation protocol. The cases were equally randomized (80 patients in each study arm) for transurethral resection in saline (TURis), transurethral vaporization in saline (TUVis), bipolar plasma enucleation of the prostate (BPEP), and classical OP. The trial was approved by the local ethics and research scientific committee. All included patients were enrolled under approved written informed consent. The randomization process was achieved by means of sealed envelopes equally nominating one of the four techniques. Allocation concealment was performed using the SNOSE method (sequentially numbered, opaque sealed envelopes). All the four types of procedures were randomly completed by three different surgeons with more than 10 years of experience in both BPH endoscopic as well as open surgery. None of these urologists was in the learning curve with regard to any of the four treatment alternatives.
The inclusion criteria were represented by prostate volume over 80 mL (measured by transrectal ultrasound [TRUS]), maximum flow rate (Qmax) below 10 mL/second, International Prostate Symptom Score (IPSS) over 19, or urinary retention imposing catheter indwelling. The exclusion criteria consisted of associated comorbidities preventing BPH surgery, in general, from being performed (such as severe heart, respiratory, hepatic, or renal failure, ongoing anticoagulant therapy that could not be stopped 7 days before the intervention for cardiovascular reasons, unstable angina, recent stroke, or myocardial infarction), previous prostate surgery, urethral strictures, and not BPH-related voiding disorders. If required, prostate cancer was screened for and subsequently ruled out by using TRUS-guided biopsy.
Concerning the technological setup, the bipolar electrosurgical procedures were carried out using the SurgMaster UES-40 generator (280–320 W for the cutting mode and 160–180 W for coagulation), the 26F OES-Pro bipolar resectoscope (Olympus Europa SE & CO KG), standard resection loops for TURis, and hemispherical-shaped button electrodes for the plasma vaporization and enucleation techniques. With regard to the surgical procedure, OP was performed by a standard transvesical approach. Bipolar TURP and TUVis followed the classical steps of BPH endoscopic surgery (first the median, then the lateral lobe and anterior lobe ablation) by either classical single wire loop resection or gradual plasma button vaporization (layer by layer prostatic tissue removal—the so-called hovering technique).
BPEP began with the median lobe enucleation by 5- and 7-o'clock incisions from the bladder neck up to verumontanum and subsequent pushback toward the bladder. A deep 12-o'clock incision separated the two lateral lobes and was continued by their descendant enucleation from the 1- and 11-o'clock positions. Similarly so, the lobes' detachment was completed by ascendant separation from the prostatic capsule begun at the 5- and 7-o'clock incisions. The residual adenoma tissue was removed by simple vaporization, followed by a careful coagulation of all hemorrhagic sources. The prostatic lobes' morcellation was performed at the end of the procedure using the Wolf Piranha device.
The evaluation protocol consisted in the preoperative and follow-up assessment (at 1, 3, 6, and 12 months after the initial intervention) of the IPSS, quality of life (QoL) score, Qmax, postvoiding residual urinary volume (PVR), and prostate-specific antigen (PSA). Pathologically confirmed prostate cancer patients as well as those who did not complete the periodical checkups were excluded from the continuation of the study.
The statistical analysis was performed using the IBM SPSS (Statistical Package for the Social Sciences, Inc.) 20.0 software. With a statistical significance level set at p<0.05, the two-sided chi-square test and the analysis of variance (ANOVA) test (with post hoc analysis—Tukey's B test) were applied. The primary endpoint of the trial was to evaluate the null hypothesis that the BPH tissue ablation capacity, perioperative blood loss, postoperative recovery period, and follow-up functional features were similar subsequent to any of the four types of techniques. With a sample size of 80 patients distributed in each treatment arm and a confidence level of 95%, the study was determined to have an 83% power to reject the considered null hypothesis.
Results
The preoperative assessment revealed resembling parameters among the four series in terms of mean patients' age and prostate volume, urinary retention rate, hemoglobin and PSA levels, IPSS and QoL scores, as well as Qmax and PVR values (Table 1).
ANOVA test.
Chi-square test.
ANOVA=analysis of variance; BPEP=bipolar plasma enucleation of the prostate; IPSS=International Prostate Symptom Score; OP=open prostatectomy; PSA=prostate-specific antigen; PVR=postvoiding residual urinary volume; Qmax=maximum flow rate; QoL=quality of life; TURis=transurethral resection in saline; TUVis=transurethral vaporization in saline.
Similar mean operation times were established for BPEP and OP, afterward followed by bipolar resection, and finally, by plasma vaporization (significantly prolonged surgical durations). By comparison to OP and plasma enucleation (equivalent BPH tissue removal outcomes), TURis emphasized a significantly decreased mean resected adenoma weight. TUVis was characterized by the lowest mean hemoglobin level drop, followed by bipolar resection and enucleation (resembling results). The morcellation stage of the BPEP procedure was not affected by significant drawbacks. OP was marked by the highest bleeding risk, which was subsequently confirmed by the substantially increased blood transfusion rate and mean irrigation length (similarly lower values in the other three series). The transvesical prostatectomy group displayed the longest mean catheterization period and hospital stay, next followed by TURis, TUVis, and BPEP (similar parameters for the latter two study arms) (Table 2).
ANOVA test.
Post hoc test: Tukey's B.
Chi-square test.
Within the immediate postoperative period (up to 1 month after surgery), a resembling safety profile was outlined for the four techniques, as emphasized by the similar rates of secondary coagulation (significant active bleeding that could not be managed by conservative measures and imposed reintervention for hemostatic purposes), recatheterization (for failed spontaneous voiding at the time of indwelling catheter removal), and urinary tract infections. As far as the medium-term complications were concerned (encountered between the months 1 and 12 of the follow-up period), equivalent data were established regarding the rates of bladder neck sclerosis and urethral strictures (diagnosed by flexible cystoscopy), as well as urinary incontinence (Fig. 1).

Short- and medium-term complication rates. BPEP, bipolar plasma enucleation of the prostate; OP, open prostatectomy; TURis, transurethral resection in saline; TUVis, transurethral vaporization in saline.
During the 1-year evaluation period, statistically similar outcomes were determined in the TURis, BPEP, and OP study groups at the 1-, 3-, 6-, and 12-month checkups concerning the mean IPSS, QoL, Qmax, and PVR features (Table 3). Therefore, the proportional improvements when compared to the preoperative measurements were equivalent among the respective three series (Fig. 2). On the other hand, the TUVis approach was marked by significantly less pronounced Qmax progresses but otherwise equivalent functional parameters (Table 3), results further confirmed by the related ameliorations when compared to the initial assessment (Fig. 2).
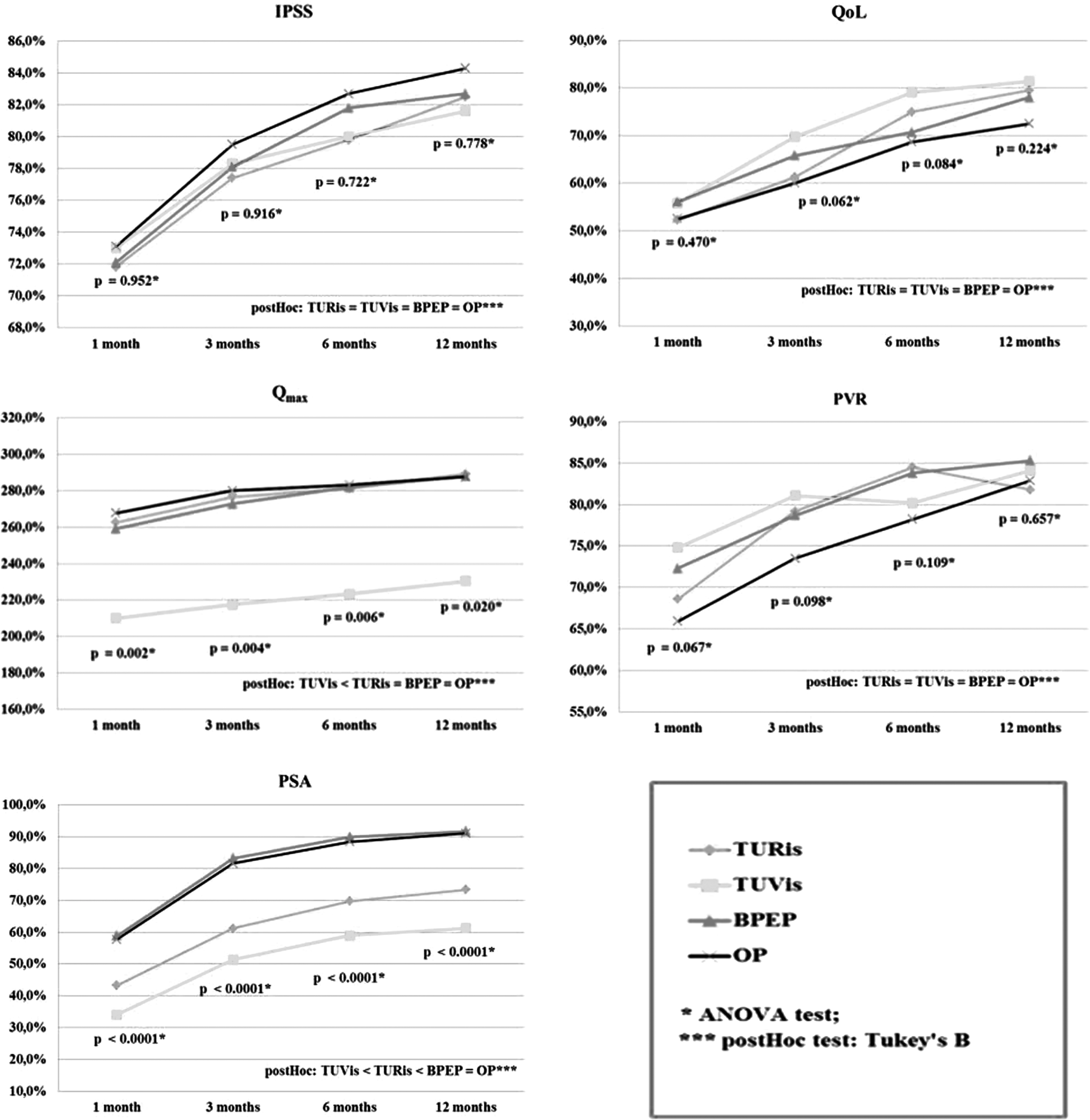
Follow-up improvements. ANOVA, analysis of variance; IPSS, International Prostate Symptom Score; PSA, prostate-specific antigen; PVR, postvoiding residual urinary volume; Qmax, maximum flow rate; QoL, quality of life.
ANOVA test.
Post hoc test: Tukey's B.
Moreover, significantly lower mean PSA levels were found subsequent to the OP and plasma enucleation procedures by comparison to bipolar resection and eventually to plasma vaporization (Table 3). Consequently, the OP and BPEP study arms similarly emphasized the highest calculated PSA value reductions by comparison to the preoperative determinations. During the 1-year follow-up protocol, these outcomes were subsequently followed by those of bipolar resection and simple plasma vaporization (on the last place). Ultimately, the TUVis approach achieved the lowest PSA level decrease at all stages of the evaluation process (Fig. 2).
Last but not least, the TRUS-based 12-month postoperative prostate volume assessment revealed significantly lower values (p<0.0001, ANOVA test; TUVis>TURis>BPEP=OP, post hoc test: Tukey's B) for BPEP and OP (20.5 and 19.7 mL) by comparison to TURis and afterward to TUVis (41.9 and 60.7 mL, respectively). Consequently, when drawing a parallel with the preoperative determinations, the calculated prostate volume reduction was substantially more pronounced (p<0.0001, ANOVA test; TUVis<TURis<BPEP=OP, post hoc test: Tukey's B) secondary to plasma enucleation and OP (83.3% and 84.7%), followed by bipolar resection (65.6%), and finally, by the simple plasma vaporization (52.1%).
Discussion
During the recent years, an increasing number of publications analyzed various aspects of bipolar electrosurgery while aiming to establish a rightful place among the acknowledged BPH treatment options. 12 The occasionally considered selection criteria of high-volume prostates imposed a parallel to open surgery in an attempt to minimize morbidity while maintaining therapeutic efficacy and functional improvements. 13 Within the race between the three main tissue ablation principles, bipolar resection seems to benefit from the extensive success of conventional TURP further improved by the reduced bleeding and lack of TUR syndrome. 14 Bipolar vaporization brings in the upper hand of superior hemostatic properties but has to deal with serious questions regarding tissue removal capacity, especially when large BPH bulks are involved. 15 Bipolar enucleation is based on the advantage of reproducing the cleavage plane of OP in a minimally invasive manner, thus optimizing coagulation as well as prostate ablation. 16 However, a standard technique for this procedure is not yet established as it may remain both technically challenging and difficult to learn. 17
Based on these premises, the present trial was designed to reach toward a premiere clinical analysis among the literature data while evaluating a single-center, prospective, randomized controlled comparison concomitantly involving all three types of endoscopic approaches as well as the standard simple OP.
Bipolar TURP displayed a constantly satisfactory efficiency when performed using the previous generation PlasmaKinetic Tissue Management System (PK-TURP; Gyrus ACMI). The technique emphasized resembling mean surgical times (89–92.3 minutes 18,19 ) and resected tissue weights (50.6–74 g 18,19 ) when compared to the presently analyzed TURis procedure (99.5 minutes and 77.9 g) while dealing with relatively similar initial prostate volumes (105.2–109.4 18,19 and 121.8 mL, respectively). When analyzing the plasmakinetic enucleation of the prostate (PKEP), at preoperative volumes of 110 to 113.8 mL, the literature data underlined rather variable surgical times (94–121.2 minutes) implied by this technique to remove a satisfactory quantity of BPH tissue (64.2–118.2 g). 18,20 From this perspective, the presently discussed BPEP approach followed the upper limit of initially measured prostate volume (122.6 mL) treated within a good procedural duration (87.4 minutes) and supported by a satisfactory ablation capability (98.7 g of resected tissue). Finally, outcomes specific for the conventional OP study group (110.3 g removed from an initial 128.7 mL mean volume within 79.4 minutes) subscribed to the average parameters established by the available literature concerning this aspect (98.7–116.8 g, 118.2–138.4 mL, and 55.4–109.5 minutes, respectively 13,21 ).
When outlining a comparison regarding the perioperative bleeding risks, bipolar vaporization stands out as enjoying the lowest mean hemoglobin level drop, both according to the published articles (0.43–0.9 g/dL 22,23 ) on the plasmakinetic vaporization of the prostate (PKVP) and to the present study (0.9 g/dL). Concerning this feature, the literature reports as well as the study arms of this analysis confirmed bipolar resection (1.55–1.8 7,19 and 1.7 g/dL) and enucleation (1.02–1.75 16,18 and 1.6 g/dL) as shortly following, but characterized by somewhat elevated hemoglobin decreases. As expected, OP described substantially higher level drops (2.9–3.15 24,25 and 3.1 g/dL, respectively), also associated with significant blood transfusion rates (6.8%–12.7% 26,27 and 7.5%) and prolonged irrigation requirements (2.7–4 28,29 and 3.8 days). In the same manner as that underlined by the previously published data, 7,16,18,19,30,31 this clinical comparison emphasized remarkably low values for the latter two parameters when referring to any of the bipolar procedures.
As far as the postoperative recovery was concerned, TUVis patients benefitted from the shortest catheterization period and hospital stay (1.3 and 2.1 days), results that favorably matched the available trials (1.14–1.45 catheter and 2.9–3.0 hospitalization days 30,31,32 –34 ). Resembling outcomes in this regard were also established for BPEP (1.6 and 2.5 days, respectively), thus outlining a satisfactory parallel with the literature data on plasmakinetic enucleation (1.47–2.8 and 3–4.2 days 18,20,35 ). On the other hand, both the TURis group of this study (2.2 and 3.2 days) as well as the PK-TURP published results (0.81–4.1 and 3.3–4.9 days 7,19,36 ) showed relatively longer catheterization and hospital periods. A substantially prolonged convalescence was defined among the OP cases of this trial (5.4 catheter and 6.7 hospitalization days) as well as of the literature series (4.42–5.6 37,38 and 5.4–9.2 days, 21,39 respectively).
The viability of the four types of procedures ultimately relies on the short- and medium-term functional benefits achieved when compared to the preoperative characteristics. From this perspective, at the 1- to 12-month check-ups, resembling progresses were obtained concerning the mean postoperative IPSS improvements subsequent to TURis (71.8%–82.5%), TUVis (73%–81.6%), BPEP (72.1%–83%), and OP (73.1% to 84.3%). Although not yet currently available within a single unitary clinical setting, the reliability of these outcomes described during the same follow-up period was supported by the literature reports regarding PK-TURP (67.9%–68.8% to 83.6%–83.7% 7,18 ), PKVP (65%–77.3% to 61.9%–66.6% 23,30 –32 ), PKEP (65.7%–72.6% to 84.3%–90.3% 16,20 ), and open surgery (66.5%–78.2% to 61.1%–85.7% 16,25 ).
During the 1- to 12-month evaluations, the mean QoL assessment revealed similar progresses among cases of the four study arms in the present analysis (52.3%–79.5% for TURis, 55.8%–81.4% for TUVis, 56.1%–78% for BPEP, and 52.5%–72.5% for OP) at comparable levels while drawing a parallel to the literature findings (23.3%–71.7% to 63.8%–80.3% for PK-TURP, 7,19,40 60.8%–80% to 59.5%–83% for PKVP, 22,30,33 28.6%–51.9% to 71.2%–73.1% for PKEP, 16,18 and 51.9%–65.9% to 57.7%–71.4% for OP 13,21 ). At this point of discussion, it may be underlined that, regardless of the substantial variability among trials taken into consideration so far, the three varieties of transurethral approaches emphasized a resembling tendency toward symptom score improvements, otherwise quite similar to those constantly specific for the classical OP.
By comparison to the preoperative parameters, the amelioration of the mean Qmax values described during the first 12 months after the initial procedure displayed a generally similar profile when considering the TURis (262.5%–289.1%), BPEP (259.1%–287.9%), and OP (267.7%–287.7%) techniques. Despite some rather wide variations, this perspective was also followed by the published studies evaluating the 1- to 12-month maximum urinary flow improvements (129.8%–192.6% to 224.1%–280.1% for PK-TURP, 7,19,36 233.3%–286.2% to 353.4%–358.6% for PKEP, 16,19,40 and 190%–229.9% to 236.1%–333.9% for OP 16,21,26,38 ). Otherwise, TUVis was characterized by statistically poorer medium-term Qmax outcomes (210.1%–230.4%), however, in respect of the PKVP literature outlines determined at 1 to 12 months after surgery (111.8%–183.3% to 113.3%–166.7% 30,32,33 ). In other words, the simple bipolar vaporization seems marked by a somewhat lower capacity to improve voiding when compared to the resection and enucleation procedures as well as to the conventional open intervention.
Last but not least, the PSA level decrease constitutes a relevant factor when attempting to assess the prostatic tissue removal capability of a certain treatment alternative in a relatively proportional manner. 41 In this regard, the plasma enucleation technique provided a substantial mean PSA value reduction at the 1- to 12-month follow-up (58.8%–91.7%), practically similar to OP results, both according to the published data (45.1%–48.9% to 83%–86.5% 16,20 ) as well as to the present findings (57.7%–91.1%). These outcomes were also consistent with the specific PKEP postoperative features (33.9%–52.6% to 80.4%–88.4% 16,20 ). Despite the lack of extensive reports concerning this parameter, a certain tendency toward an inferior PSA level decrease was occasionally underlined with regard to PK-TURP (19.1%–64% 7 ) and bipolar vaporization (29.4%–51.2% to 58.7%–59.1% 30,34,42,43 ). During the respective 12-month evaluation period of this trial, both bipolar resection (43.3%–73.4%) and vaporization (34%–61.3%) were significantly surpassed (in this particular order) by the previously mentioned BPEP and OP parameters. While correlating these figures with the substantially elevated mean resected tissue weights achieved during plasma enucleation and open surgery by comparison to TURis, it becomes clear that BPEP and OP have the upper hand over transurethral resection in terms of BPH bulk ablation capacity.
Furthermore, in this particular clinical setting, the TUVis approach provided a significantly reduced mean PSA level decrease, thus suggesting a diminished adenoma removal rate when compared with the other treatment alternatives. This shortcoming negatively reflected upon the Qmax determinations, which constantly remained inferior when drawing a parallel to the TURis, BPEP, and OP features. From another perspective, the symptom scores and PVR values displayed relatively resembling data in the four series. In other words, at least on the medium term, the differences concerning the prostatic tissue ablation capability seem to significantly influence improvements concerning the urodynamic parameters, but do not substantially affect the IPSS, QoL, and PVR outcomes.
In light of all of the above, it should be emphasized the considerable variability of clinical outcomes related to the various plasmakinetic techniques 10 as well as the quite insufficient number of available studies thoroughly analyzing the evidence-based progresses achieved through these types of endoscopic interventions. 20 While also taking into account the growing modern tendency toward widely replacing PK-based procedures with the newer generation of transurethral plasma surgery in the daily urological practice, the present analysis may provide a reliable basis when aiming to determine the appropriate place of bipolar electrosurgical approach as part of the large BPH standard treatment protocol.
Conclusions
OP and plasma enucleation emphasized the highest surgical efficiency, as confirmed by the significantly improved mean operation times and resected prostatic tissue weights. Bipolar resection was ranked below OP and BPEP and over TUVis in terms of surgical speed and efficacy. Although clearly slower, the simple plasma vaporization benefited from the lowest perioperative blood loss and shortest convalescence period. OP was marked by the drawbacks of invasive surgery related to the substantially increased mean hemoglobin level drop, blood transfusion rate, irrigation time, catheterization period, and hospital stay. The TURis and BPEP techniques displayed equivalent hemostatic properties, constantly ranked between TUVis and OP. The plasma enucleation and vaporization patients benefited from the fastest postoperative recovery.
During the 1-year follow-up period, resembling functional outcomes were determined for TURis, BPEP, and OP, as shown by the similar mean symptom scores, urinary flow rates, and postvoiding residual volumes determined at all periodical check-ups. The TUVis procedure displayed similar IPSS, QoL, and PVR results. On the other hand, the plasma vaporization series emphasized constantly less pronounced Qmax improvements. Furthermore, the significantly lower mean PSA levels and related proportional reductions by comparison to the preoperative measurements confirmed the substantially superior and similar BPH tissue removal capability of open surgery and plasma enucleation, followed by TURis, and finally by the TUVis technique.
Footnotes
Disclosure Statement
Bogdan Geavlete is a speaker in Olympus sponsored symposiums. The remaining authors have no competing financial interests.