
Abstract
In recent years, robot-assisted radical cystectomy (RARC) has shown similar oncologic outcomes compared with the gold standard open radical cystectomy with the added benefit of less blood loss and shorter hospital stay. Robot-assisted cystectomy with intracorporeal ileal neobladder is a complex surgical procedure and is usually performed in centers with experienced surgeons. We propose robot-assisted cystectomy with intracorporeal neobladder using the Y pouch previously described in open radical cystectomy. We think that the Y pouch is easier to perform than conventional spherical pouches without compromising functional outcomes. It may therefore be a good alternative for patients undergoing RARC with intracorporeal diversion.
Introduction
T
Since then, various reports have shown that RARC is safe and feasible with superior outcomes in terms of blood loss, shorter hospital stay, and earlier return to bowel function. 2 –6 Beecken and associates 7 reported the first case of RARC with intracorporeal ileal neobladder. Long operative time, however, has remained an important issue, and many centers preferred extracorporeal urinary diversion to reduce the operative time and costs.
A recent report from the International Robotic Cystectomy Consortium has shown that intracorporeal urinary diversion is feasible with lower risk of complications including gastrointestinal complications 8 compared with extracorporeal urinary diversion. This could be attributed to shorter wound incision, less pain, and decreased bowel exposure. Intracorporeal ileal neobladder, however, remains technically challenging with a significant learning curve and is usually performed only in centers with experienced surgeons.
In this article, we report the first case of robot-assisted radical cystoprostatectomy with intracorporeal Y pouch neobladder. The Y pouch, also known as a Tanta pouch, was first described by the Egyptian group in 1988. 9 The Y pouch was reconstructed using 40 cm of terminal ileum, which consists of the central detubularized segments arranged in a U shape and two limbs for ureteroileal anastomosis. 9 A recent report from the same group has also demonstrated similar functional outcomes of the Y pouch compared with the conventional spherical pouch with daytime and nighttime continence of 93.3% and 85.5%, respectively at 3 years. 10 It has been shown that the Y pouch is a low pressure, high volume reservoir with similar long-term functional outcomes compared with other spherical pouches. 10
In this article and the accompanying video demonstrating this technique (available at
Technique
Under general anesthesia, the patient was placed in a Trendelenburg position with adequate padding to prevent neuromuscular injury. A 20F Foley cathether was inserted into the bladder. A five-port approach is used. The 12-mm optical trocar was inserted 2 cm above the umbilicus using the Hassan approach. Two 8-mm robotic ports were inserted about 8 cm away from the umbilicus. A 12-mm assistant port was inserted 8 cm away from the right robotic port. Another 5-mm port for suctioning was inserted between the camera and right robotic port (Fig. 1). After the port insertion was completed, the patient was placed in a steep Trendelenburg position and the robot was docked. The nerve-sparing cystoprostatectomy was completed followed by a standard pelvic lymph node dissection.
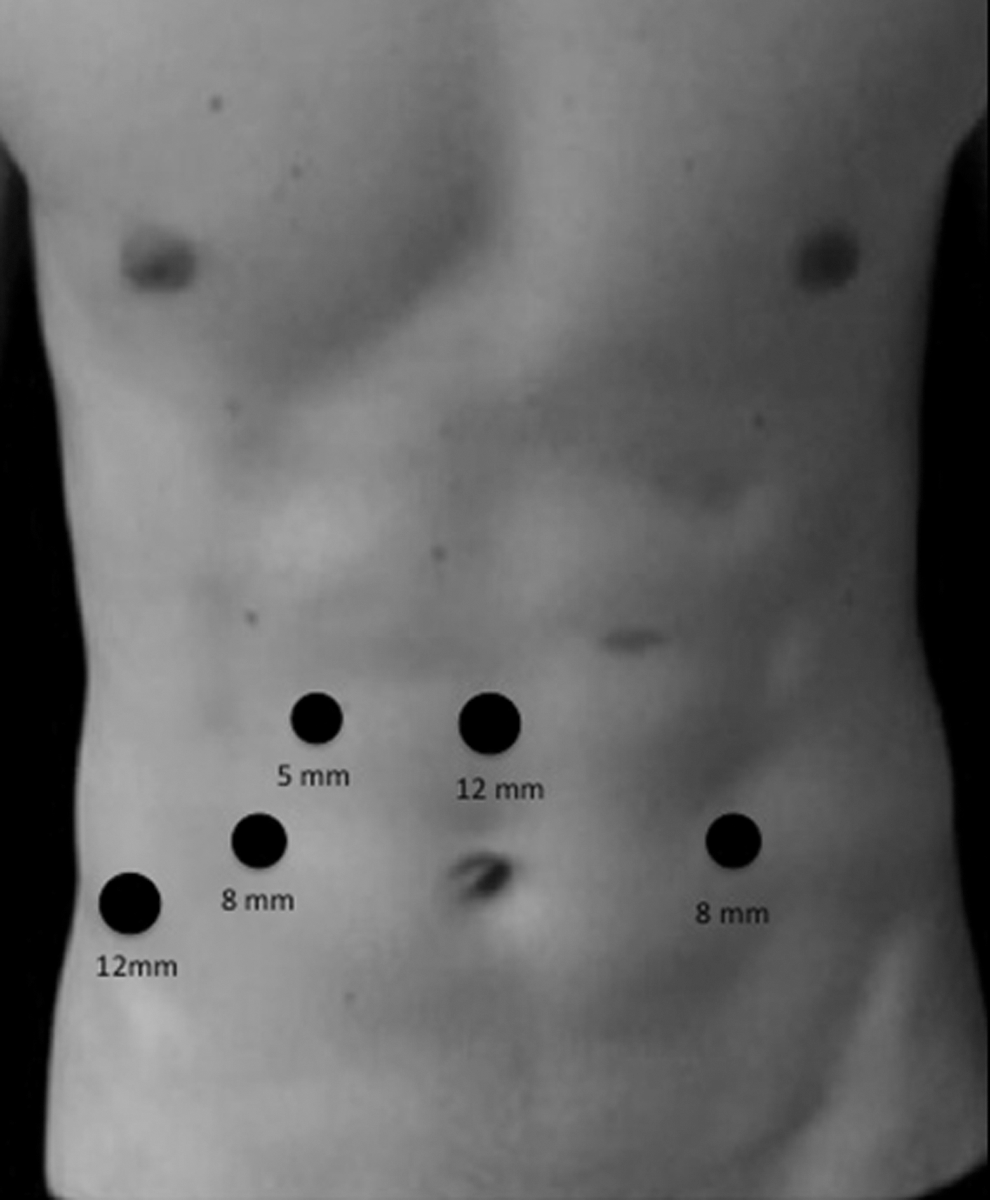
Port placements: 12-mm supraumbilical camera port; 8-mm robotic port×2; 5-mm assistant port for suction; and a 12-mm assistant port.
For creation of the Y pouch neobladder, after completion of the radical cystoprostatectomy and lymphadenectomy, both ligated ureters were left in their respective side, and there was no need to transpose either ureter below the sigmoid mesocolon. At this point, the robot was undocked, and the Trendelenburg position was reversed approximately 20 degrees to allow the bowels to descend into the pelvis.
An estimated 40-cm segment of terminal ileum 25 cm away from the ileocecal valve was identified as the bowel segment was measured using visual estimation, as well as relation to pelvic anatomy. The ileal segment was brought down to the pelvis to ensure adequate mesenteric length to allow for a tension-free urethroileal anastomosis. The 40-cm segment was arranged in a U-shaped configuration that was made out of two central segments of 14 cm each and two limbs of 6 cm each. 10 A stay suture was placed to mark the most distal portion of the U-shaped loop. An opening was made close to the stay suture for the urethroileal anastomosis.
The urethroileal anastomosis was completed using the 3/0 Stratafix™ suture over a 20F Foley catheter. The proximal and distal end of the 40-cm segment was transected using an Endo-GIA™ stapler. The bowel continuity was restored by performing functional end-to-end or anatomical side-to-side anastomosis using an Endo-GIA stapler. The two central limbs were detubularized at the antimesenteric borders, and the two limbs were left intact. The posterior plate of the two central detubularized segments was joined using 3/0 V-Loc™ sutures in a running fashion. This was followed by closure of the anterior plate in a similar fashion.
The ureters were anastomosed to the dorsal aspect of the two limbs with 4/0 Vicryl® sutures using the Nesbit technique. 11 In this case, the ureteroileal anastomosis was performed over a 7F Double-J stent. After the completion of the anastomosis, the Y pouch was tested; no leakage was seen. One surgical drain was placed and pneumoperitoneum was evacuated.
Equipment
• da Vinci® Surgical System
• 0-degree telescope
• 12-mm port×2, 8-mm robotic port×2, 5-mm port×1
• 60-mm Endo-GIA staplers with reloads
• 3/0 Stratafix suture
• 3/0 V-Loc sutures
• 4/0 Vicryl sutures
• 7F Double-J stent×2
Role in Urologic Practice
To date, we have performed three cases of RARC with Y pouch neobladder. In this reported case, the postoperative cystogram and intravenous urogram showed an intact neobladder with no upper tract dilatations (Fig. 2). The operating time was 340 minutes with minimal intraoperative blood loss. There were no perioperative and postoperative complications reported. The urethral catheter and Double-J stents were removed at postoperative day 14 after satisfactory cystography showing an intact neobladder with no significant upper tract dilatation.
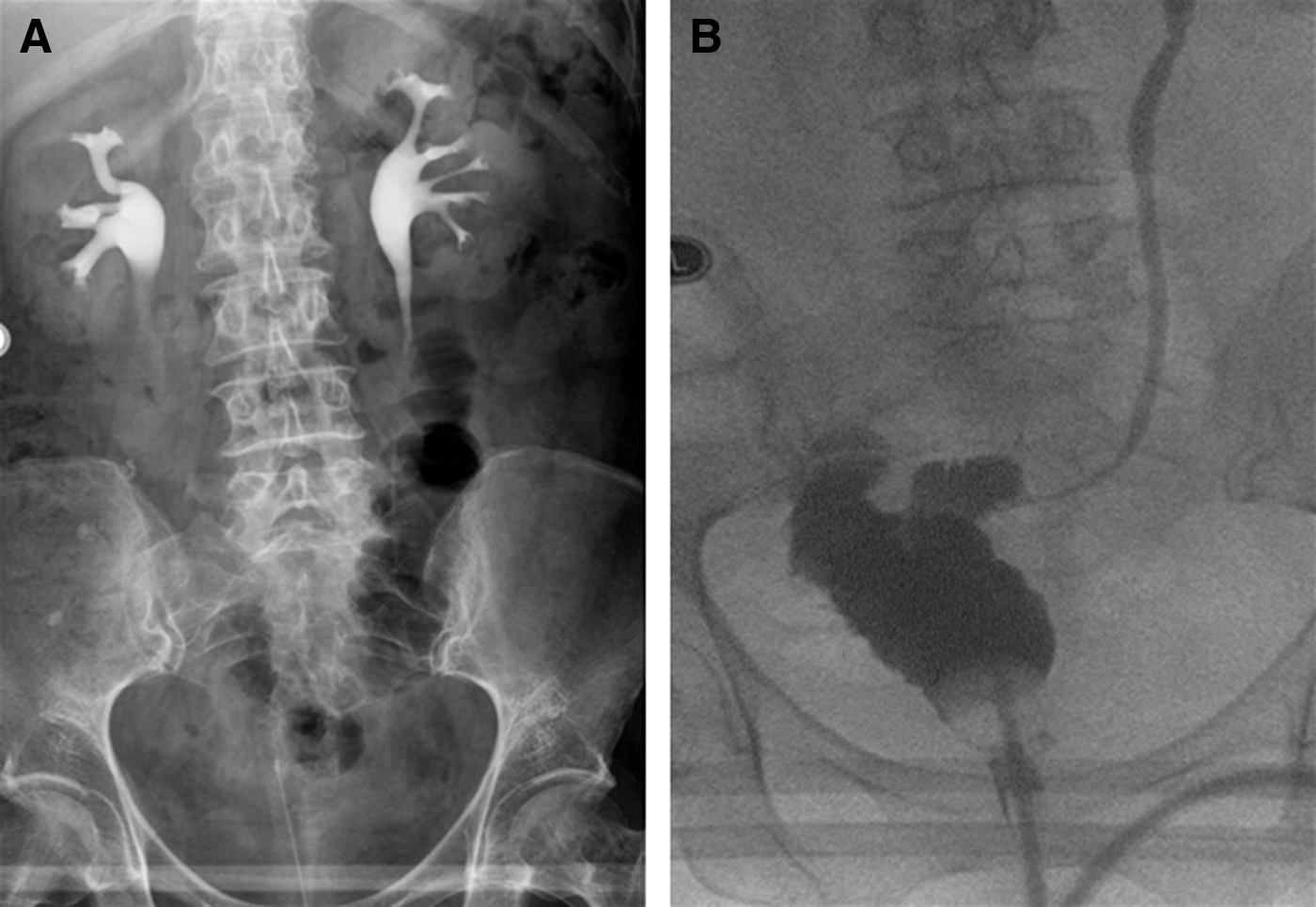
Postoperative intravenous urogram
In this reported case, the ileal segment was taken approximately 25-cm away from the ileocecal valve to ensure adequate mesenteric length for the urethroileal anastomosis. Before transecting the bowels, the ileal segment was brought down to the pelvis to ensure that the mesentery was long enough to ensure a tension-free urethroileal anastomosis.
Previous studies have shown that robot-assisted cystectomy with intracorporeal ileal neobladder is safe and feasible. In most series, however, the operative time is still significantly longer than extracorporeal urinary diversion, and a steep learning curve is expected to perform surgery of such complexity. 12,13 We think that the Y pouch neobladder has a few advantages over the more complex spherical pouches. The Y pouch is easy to construct without any need to fold the bowel segments and less manipulation of the bowel is needed. With the presence of dual limbs for the ureteroileal anastomosis, there is no need to transpose either ureter under the sigmoid mesocolon. This means less traction and less skeletalization of the ureters, therefore making the Y a suitable option in cases with short ureteral length.
Previous authors also proposed that a Y pouch provides an easy retrograde approach to the upper tract if necessary. With upper tract recurrence, diagnostic and therapeutic ureterorenoscopy can be performed easily in retrograde fashion. 10 In the event of upper tract recurrences, radical nephroureterectomy can be performed by resecting the affected kidney and ureter with a portion of the limb without having to take down a Wallace anastomosis in the case of conventional neobladder. In this case, we opted to complete the ureteroileal anasotomis over Double-J stents instead of a conventional single J stent. Previous studies has shown that use of the Double-J stent is superior over a single J stent in terms of patient comfort and shorter hospital stay with no difference in the stricture formation and complication rates. 14,15
Conclusion
An intracorporeal Y pouch neobladder is safe and feasible and provides a good alternative for patients undergoing robotic-assisted cystectomy with intracorporeal neobladder. More patients and longer follow-up will be needed to conclude the functional outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.