
Abstract
Purpose:
Previous studies analyzing the relationship between Body Mass Index (BMI) and complications after partial nephrectomy have been underpowered. We use a national surgical database to explore the association of BMI with postoperative outcomes for Open Partial Nephrectomy (OPN) and Minimally Invasive Partial Nephrectomy (MIPN).
Patients and Methods:
Years 2005–2012 of the National Surgical Quality Improvement Program (NSQIP) were queried for OPN and MIPN. Postoperative complications were organized according to Clavien Grades and compared across normal weight (BMI kg/m2=18.5–<25.0), overweight (BMI=25.0–<30.0), and obese (BMI≥30.0) patients using standard descriptive statistics and multivariate regression modeling.
Results:
Of 1667 OPNs and 2018 MIPNs, 46.2% of patients were obese. Operative time was 16.91 minutes longer on average for obese patients (p<0.001). The overall complication rate after OPN was 17.9%, 17.2%, and 17.9% (p=0.945) for normal weight, overweight, and obese patients, respectively; while the overall complication rate after MIPN was 6.9%, 6.3%, and 8.7% (p=0.147). Multivariate regression analysis demonstrated that overweight and obese patients were not at increased risk for any complication grade after OPN and MIPN compared to normal weight patients. When comparing procedures, MIPN had a lower complication rate compared to OPN for obese (8.7% vs 17.9%, p<0.001) and morbidly obese patients (9.2% vs 22.2%, p=0.001).
Conclusions:
Although surgery in obese patients is longer compared to normal weight patients, it does not appear to increase the likelihood of 30-day postoperative complications for OPN or MIPN. However, obese patients undergoing MIPN had lower complication rates than those undergoing OPN.
Introduction
A
As a result, several institutions have evaluated outcomes for both open partial nephrectomy (OPN) and minimally invasive partial nephrectomy (MIPN) across BMI categories, with some series demonstrating no difference 1–2 while others reporting increased operative complications among obese patients. 3–4 A systematic review and meta-analysis were conducted to reconcile these results specifically in laparoscopic partial nephrectomy and concluded that while the overall complication rate did not differ significantly between obese and nonobese patients, obese patients were more likely to experience a Clavien Grade 3 or greater complication than normal weight patients. 5
Nevertheless, several institutional series released after the above meta-analysis report no difference in complication rates between obese and nonobese patients. 6 –8 Furthermore, on closer analysis of the institutional series comparing obese to nonobese patients, most analyzed data from less than 150 obese patients. 1 –4,6 –11 In fact, even the meta-analysis by Aboumarzouk et al. only studied 256 obese patients undergoing laparoscopic partial nephrectomy and its finding of increased grade 3 or higher complications was based on an absolute difference of only five complications between groups.
To address this lack of statistical power in the existing literature, we used the American College of Surgeons' multi-institutional National Surgical Quality Improvement Program (NSQIP) database to critically analyze the impact of BMI on postoperative complications during both OPN and MIPN. We also sought to compare complication rates between OPN and MIPN for obese and morbidly obese patients to assess if these patients fared better with either approach.
Patients and Methods
Population
We queried years 2005 to 2012 of the American College of Surgeons' National Surgical Quality Improvement Program with Current Procedure Terminology codes for all patients undergoing a partial nephrectomy (50240) or a laparoscopic partial nephrectomy (50543). Institutional review board approval is not required at our institution to analyze ethically preapproved datasets. NSQIP tracks over 240 variables, such as patient demographics, clinical characteristics, comorbidities, lab values, and 30-day postoperative complications for a participating institution's inpatient and outpatient procedures. Reviewers entering data undergo rigorous training, and NSQIP data undergo several audits to ensure accuracy. Further information on NSQIP is available elsewhere. 12
Patients were stratified according to BMI into four classes: underweight (BMI<18.5), normal weight (18.5≤BMI<25), overweight (25≤BMI<30), and obese (BMI≥30). A subanalysis was conducted for morbidly obese patients (BMI≥40). All underweight patients and those with missing BMI data were excluded from the analysis. Patients undergoing any concurrent scheduled surgical procedures besides OPN or MIPN were also excluded from the study due to potential confounding.
Data collection
The data collection methods of the NSQIP database have been previously described. Despite being a multicenter collaborative, intensive standardized training of reviewers and internal audit mechanisms have led to reproducible and reliable data. An overall disagreement rate of 1.8% was found among all assessed variables. 12
Outcomes and statistical analysis
The postoperative complications tracked through NSQIP were grouped according to Clavien Grades. Although NSQIP does not stratify its complications by Clavien grade, we grouped postoperative morbidities based on how they are treated in routine clinical practice under Clavien grading criteria. For instance, Clavien grade 1 complications such as compression neuropathies, acute renal failure, and superficial surgical site infections are almost always treated conservatively and thus qualify as grade 1.
The main outcome of the study was the incidence of complications of each Clavien grade across BMI categories for both OPN and MIPN. Multivariate regression models were then constructed to adjust for patient age, comorbidities, functional status, American Society of Anesthesiology (ASA) score, and procedure type. Total operation duration was compared for patients instead of total room time or total anesthesia time because of differences in transferring patients to the operating table or differences in time to induce anesthesia. Over 40 patient comorbidities were recorded for patients, and a comorbidity count was employed in the regression models. Patients with null values for comorbidities were counted as not having the given comorbidity. Lastly, complication rates were compared between OPN and MIPN for the subset of obese and morbidly obese patients, enabling analysis of procedure type in these patients. All statistical analysis was conducted via Statistical Package for the Social Sciences (SPSS®) version 20.
Results
Description of patient population
After excluding underweight patients, 17 patients with incomplete BMI data and those patients undergoing additional procedures, 1667 (45.2%) underwent OPN and 2018 (54.8%) underwent MIPN. In the entire group, 18.9% were normal weight, 34.8% overweight, and 46.2% obese.
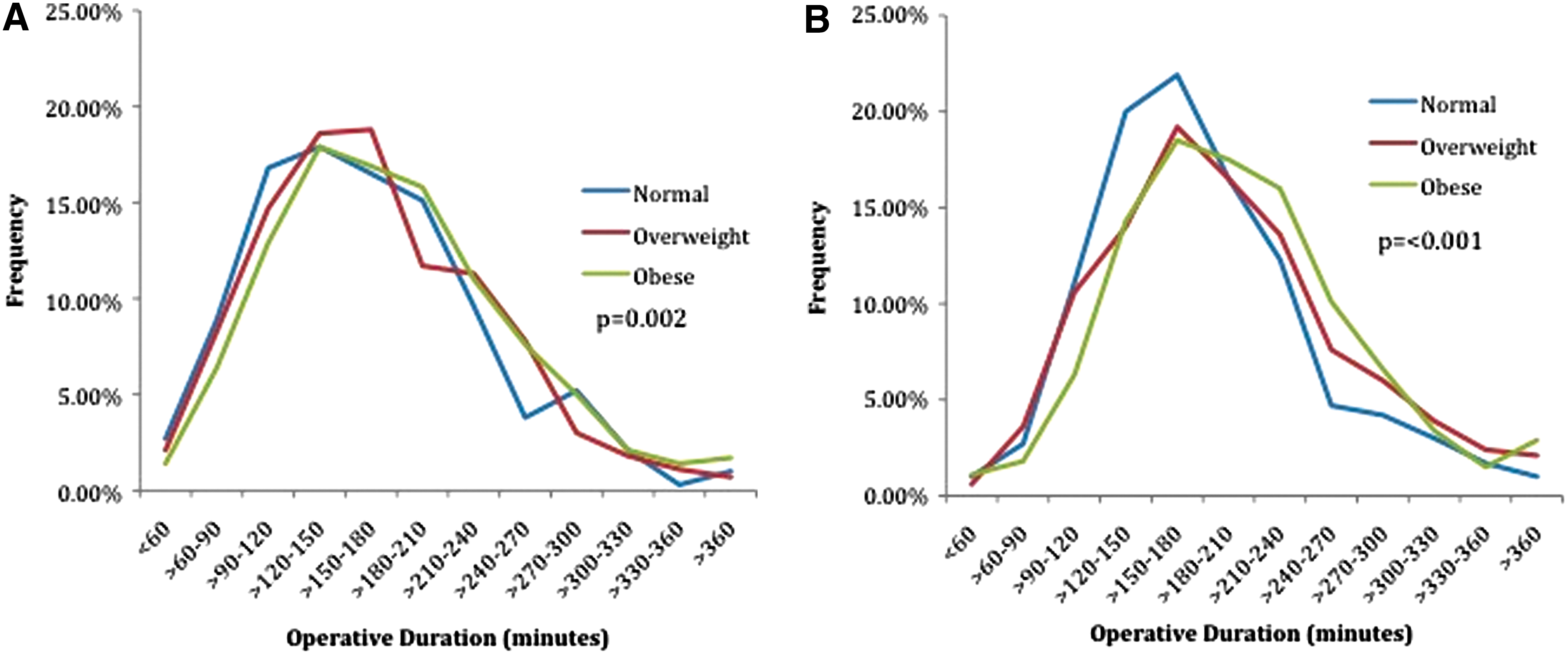
Table 1 presents the baseline characteristics of patients across the BMI categories. Overweight and obese patients had more comorbidities (p<0.001) and a higher ASA (p<0.001) when compared to normal weight patients. Specifically, obese patients were more likely to have diabetes, dyspnea, hypertension, and a greater ASA score. Obese patients also had significantly longer operative times regardless of the technique used (+16.91 minutes, p<0.001). For OPN (Fig. 1A), the mean operation time for normal weight, overweight, and obese patients was 165.27, 168.93, and 179.26 minutes (p=0.002). For MIPN (Fig. 1B), the mean operation time was 180.28, 192.73, and 201.53 minutes (p = <0.001). Lastly, there were no differences in functional status (independent or dependent) across BMI categories (p=0.943).
p values represent the results of an ANOVA indicating whether or not there were any differences in rates across BMI category.
ASA=American Society of Anesthesiology; ANOVA=analysis of variance; BMI=body mass index.
Complication rates by BMI category
Postoperative complication rates were stratified across BMI classes for OPN or MIPN (Table 2). The rate of any complication for OPN patients was 17.9%, 17.2%, and 17.9% for normal weight, overweight, and obese patients, respectively (p=0.945). The rate of any complication for MIPN patients was at 6.9%, 6.3%, and 8.7% for normal, overweight, and obese patients, respectively (p=0.147). Furthermore, there were no differences across BMI categories for OPN or MIPN across each of the Clavien grades. Multivariate regression models (Table 3) confirmed that increasing BMI did not increase the risk of any complication of any grade, after controlling for patient age, comorbidities, ASA score, functional status, and procedure type.
DVT=deep vein thrombosis; MIPN=minimally invasive partial nephrectomy; NA=not applicable; OPN=open partial nephrectomy; PE=pulmonary embolism; SSI=superficial surgical site infection; UTI=urinary tract infection.
CI=confidence interval; OR=odds ratio.
Comparing procedure type for obese and morbidly obese patients
Table 4 compares complication rates between OPN and MIPN for normal weight, overweight, obese, and morbidly obese patients. For normal and overweight patients, OPN had a higher complication rate than MIPN (Normal weight: 17.9% vs 6.9%, p =<0.001; Overweight: 17.2% vs 6.3% p =<0.001), with significantly different rates of grade 1, 2, and 4 complications. MIPN had a markedly lower overall complication rate than OPN for obese patients (8.7% vs 17.9%, p<0.001), and this difference was sustained across complication grades 1 through 4. For the subset of morbidly obese patients, while MIPN did have a lower overall complication rate than OPN (9.2% vs 22.2%, p=0.001), this difference was mainly driven by a significant difference in grade 2 complications alone.
Discussion
Previous studies analyzing the impact of BMI on complications after partial nephrectomy have been contradictory and inconclusive in their findings largely due to inadequate sample size, institutional differences, and discrepancies between provider learning curves. In our analysis of a multi-institutional dataset spanning the course of 8 years, over 1200 overweight patients and over 1700 obese patients were compared to 700 normal weight controls in an effort to overcome any institutional and statistical discrepancies. Our analysis determined that obese or overweight patients are no more likely to experience a postoperative complication after either OPN or MIPN. This observation was confirmed by multivariate regression models that did not uncover significantly increased odds of any complication with increasing BMI after adjusting for patient age, comorbidities, functional status, ASA classification, and procedure type.
Operating on obese and morbidly obese patients presents many challenges to surgeons and anesthesiologists. Anesthesia presents many difficulties such as ventilatory, cardiovascular, drug dosing, and intubation/extubation challenges. Surgeons will have no hesitation in describing the many technical challenges with operating on obese and morbidly obese patients, including oftentimes difficult postoperative care. Therefore, our results may seem surprising and counterintuitive. Indeed, our results partially contradict the systematic review and meta-analysis by Aboumarzouk et al. looking at the impact of obesity on outcomes in laparoscopic partial nephrectomy. 5 Our analysis agrees with the meta-analysis' finding of no significant difference in overall complications between obese and nonobese patients. However, the meta-analysis did find that grade 3 or higher complications were more common in obese patients while our analysis found no significant difference. This discrepancy may be explained by differences in sample size, as we studied over three times more surgeries (2018 MIPNs vs 659 for the meta-analysis)—assuming the larger sample size in our dataset evens out the complications between BMI classes that clinical experience would suggest otherwise. In addition, our study is in accordance with more recent investigations reporting nonsignificant differences in complication rates of MIPNs across BMI categories. 1,6 –8 Our data also support previous efforts by Romero et al. demonstrating that obese and nonobese patients had similar outcomes during OPN. 9 Thus, as a whole, our findings corroborate the recent literature on obesity in both MIPN and OPN by demonstrating no significant increase in complications among obese patients.
We also thought it was unusual that higher BMI did not correlate with increased complications based purely on operative duration. Obese patients in our series had a significantly longer operative time than normal weight patients for both OPN and MIPN, yet lacked increased complications such as airway complications, deep vein thrombosis, or pulmonary embolism for example. Recent NSQIP studies in other disciplines have quantified that 60-minute increases in operative duration were associated with increased complication rates. 13,14 However, our study found that operative duration for obese patients increased only by an average of 14 minutes (OPN) and 21 minutes (MIPN), suggesting that minor differences in operative duration may not result in increased complications. We are not the first to describe an increased operative duration with increasing BMI, but this is controversial with partial nephrectomy. For instance, in MIPN some studies have shown longer duration 10 while others have not 5,8 and one study in OPN reports increased operative time for obese patients. 9 Our series adds to this volume of literature in both OPN and MIPN to demonstrate that while total operation time may be increased for obese patients, the difference does not appear to clinically manifest in the form of increased complication rates.
A second aim of our study was to verify if previous reports of lower complication rates with MIPN versus OPN applied to all BMI classes. 15–16 We found that MIPN was associated with a lower complication rate than OPN in every BMI class. The differences in total complication rates between MIPN and OPN for obese patients (8.7% vs 17.9%) and morbidly obese patients (9.2% vs 22.2%) were substantial (Table 4), but the majority of this difference was achieved by grade 1–2 complications and rates of grade 3+complications were relatively similar between operative approaches. This result, however, should be interpreted with caution, as surgeons will generally reserve OPN for perceived complexity and thus we are not comparing like with like. Therefore, this part of the analysis is likely to suffer considerably from surgical selection bias. However, it is interesting to note that with increasing BMI the numbers of patients receiving MIPN was slightly higher than OPN (BMI≥30 class: MIPN 52.3% vs OPN 47.7%, BMI≥40 class: 54.6% vs 45.4%), which would suggest that BMI as a categorical variable alone may not be a major technical hurdle. Of course this dataset may consist of purely open surgeons or minimally invasive surgeons who would proceed in their preferred approach regardless of BMI. It does suggest that the considerations for approach are tumor based and not dependent on BMI class.
This study is subject to the standard limitations of administrative datasets and assumes the reliable coding of medical and surgical events across institutions. We also could not adjust for tumor size, grade, location, surgical learning curve, surgeon volume, and specifics of operative technique in our analysis as this information is not provided in NSQIP. Additionally, NSQIP is known for its granularity with regard to 30-day postoperative complications but it does not capture intraoperative parameters such as clamp time or procedure specific complications such as warm ischemia time, urine leak, and conversion rates. Furthermore, our dataset also does not account for visceral fat versus peripheral fat distribution in obese individuals, which may be a significant limitation of using BMI to predict complications. 17 A recent study found that perinephric fat was a better predictor of increased operative time and blood loss than BMI in robot-assisted partial nephrectomy, explaining that there may be variations in amount of perinephric fat for patients with similar BMIs. 18 In addition, robotic and laparoscopic partial nephrectomies have the same CPT code, precluding any distinction between the two procedures in our BMI analysis. Lastly, given that the study is retrospective and not protocol driven, we cannot account for the possibility of obese patients being treated differently in the perioperative period that may have compensated for their increased risk of complications. Nevertheless, these limitations are not unique to our study and often plague retrospective and administrative studies in general.
Conclusion
In a multi-institutional analysis of 3685 partial nephrectomies, our data suggest that despite increased operative duration, obese or overweight patients are no more likely to experience a postoperative complication after either OPN or MIPN based on bodyweight, even after adjusting for patient age and comorbidities. We also verified that the lower overall complication rates of MIPN relative to OPN seen in previous administrative studies apply across patient BMIs.
Footnotes
Disclosure Statement
The authors declare no conflict of interest.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.