
Abstract
Background and Purpose:
The urothelium represents “the tightest and most impermeable barrier in the body.” We investigated the distribution of paclitaxel (PTX) in the ureteral wall after the inflation of a paclitaxel-eluting balloon (PEB) in an attempt to elucidate the possibility of clinical application of PEBs in the ureter.
Materials and Methods:
Nine domestic pigs were used. Nine PEBs and nine conventional percutaneous angioplasty balloons (CB) were inflated in the right and left ureter of each animal, respectively. The ureter treated by CB was the control for the contralateral ureter. Specimens were removed: Immediately after inflation (group A), after 12 hours (group B), and after 24 hours (group C). Two samples were obtained from each ureter of groups A, B and C. One sample was investigated by nuclear magnetic resonance spectroscopy (NMR), the other by histology and immunohistochemistry (IHC) using a specific for PTX polyclonal antibody.
Results:
Reduced inflammation was observed in the group B and C samples in comparison with their controls. PTX was distributed mostly in the urothelium and submucosal layer in group A (IHC). The agent was present in the urothelial, submucosal, and muscle layer in groups B and C. The concentration of PTX (NMR) has been reduced in group C compared with the tissue extracts of group B.
Conclusion:
The distribution of PTX includes the urothelial, submucosal, and smooth muscle layers. Inflammation was reduced in the case of drug-eluting balloons.
Introduction
D
Balloons used for the dilation and minimally invasive management of ureteral strictures are similar in concept to the angioplasty balloons. 5 The minimally invasive management of ureteral strictures is related to various success rates. 5 –9 The restenosis of previously treated ureteral strictures has been related to collagen rich connective tissue with few fibroblasts and smooth muscle fibers in the scarred area. 10 Excess type 3 collagen in comparison with type 1 collagen has been detected in ureteral strictures and is considered to cause ureteral fibrosis and stenosis of the lumen. 11 –14 Smooth muscle cells (SMCs) are the major collagen producers in the ureter. 14 Paclitaxel (PTX) is a chemotherapeutic substance that stabilizes cellular microtubules and results in the inhibition of cell replication. 15 –17
PTX has a dose-dependent effect on ureteral SMC and urothelial cell proliferation. The antiproliferative effect of PTX on SMCs results in the reduced production of type 3 collagen by these cells. This phenomenon is practically the mechanism for the prevention of fibrotic reaction that leads to ureteral strictures. 18
Considering the above, the use of DEB with PTX in the ureter would represent an interesting concept for the improvement of the outcome of the minimally invasive treatment of ureteral strictures. Nevertheless, the efficacy of DEBs in the ureters may be hindered by the unique properties of the urothelium. The stratified uroepithelium forms a distensible barrier that accommodates large changes in urine volume while preventing the unregulated exchange of substances between the urine and the blood supply. 19 The permeability to substances that normally can cross membranes with a rapid rate such as water and protons is extremely low in the case of urothelium. 20 This task takes place by the outermost umbrella cell layer including high resistance paracellular tight junctions, an apical glycan layer, and an apical membrane with a distinctive lipid and protein composition. 15,21 –25 Moreover, the umbrella cell layer has the potential to change the apical surface by mechanism of exocytosis and endocytosis. 26 –29
The above histology of the urothelium sets the background for the “tightest and most impermeable barrier in the body.” 20 Thus, the first step for the evaluation of DEB with PTX in the ureter would probably be the investigation of the distribution of PTX in the ureteral wall and the confirmation of the penetration of the substance to subepithelial SMCs.
We investigate the distribution of PTX released by a DEB in the porcine ureter.
Materials and Methods
Animals and materials
Animals
Nine domestic female pigs weighing between 20 and 25 kg were included in the experiment. The protocol was approved by the responsible public services.
Materials
Nine PTX eluting percutaneous angioplasty balloons (PEB) (IN Pact Admiral, Medtronic Inc., Minneapolis, MN) and nine CB (Admiral Xtreme, Medtronic Inc.) were inserted in the right and left ureter of each animal, respectively. The ureter treated by CB was the control for the contralateral ureter. The dimensions of the balloons were 80 mm length and 6 mm diameter.
Methods
Anesthesia
The induction to anesthesia included a combination of ketamine, xylazine, and atropine sulfate. All pigs were intubated and ventilated. Intravenous propofol 5% was administered to maintain the anesthesia. Postoperative analgesia and perioperative antibiotic prophylaxis were administered.
Intervention
Each pig was placed in the supine position. Cystoscopy was performed, and 0.035-inch hydrophilic guidewires were inserted in each ureter under fluoroscopic guidance. A 7F ureteral catheter was inserted over each hydrophilic guidewire and the latter was exchanged for a stiff guidewire. The balloons were inserted over the stiff guidewire, inflated to their maximal diameter for 5 minutes and then removed. The dilation was always performed in the distal third of the ureter; the CB was always the first to be inflated to avoid contamination of the control ureter with PTX.
Specimen removal
The animals were sacrificed and their ureters were removed at the following times after the balloon dilation: Group A: Immediately after the inflation of the balloons (t0); group B: after a period of 12 hours (t1); group C: after a period of 24 hours (t2).
Samples from the ureters of all groups were examined by nuclear magnetic resonance spectroscopy (NMR) and pathology-immunohistochemistry (IHC).
Sample examination
NMR
The presence of PTX was determined by the use of NMR, which allows the detection of specific molecules. A reference 1H 1D NMR spectrum of the PTX was obtained by washing out PTX from a PEB with 2 mL of dimethyl sulfoxide (DMSO)-d 6. The PTX white powder washout took place into a 15 mL Falcon tube, and PTX was solubilized in DMSO. Then, 0.6 mL of the solution was transferred to a 5-mm NMR tube and 1H 1D and 1H-13C heteronuclear single quantum coherence NMR spectra were recorded. Based on previously published PTX NMR data, 30 –32 we were able to identify and assign all proton resonances of PTX (Fig. 1).
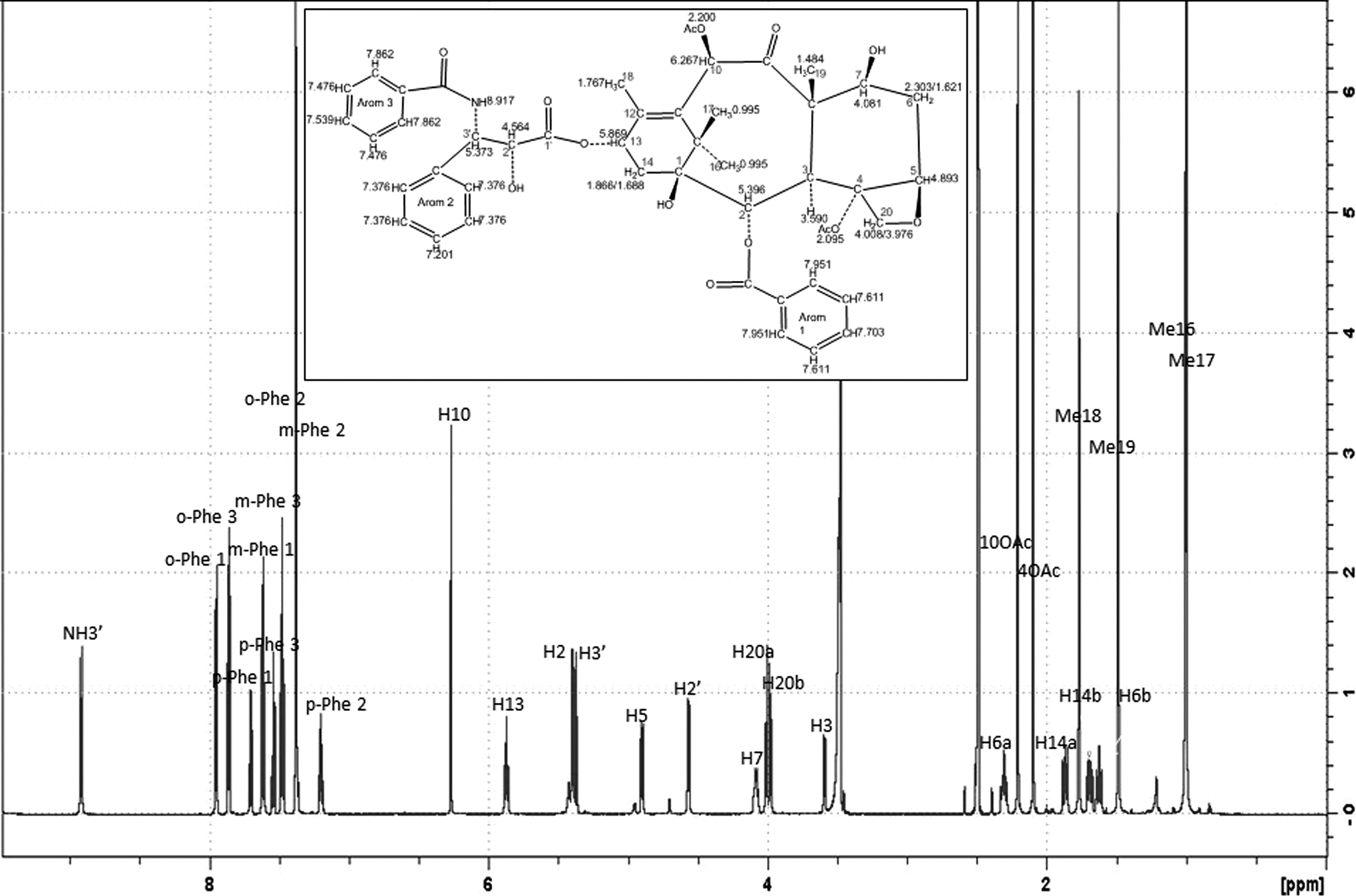
Supporting Information, 1H 1D NMR spectrum at 298K, 700MHz, chemical structure and proton chemical shifts of paclitaxel. NMR, nuclear magnetic resonance spectroscopy.
After the successful acquisition of the PTX referral spectra, 1 g specimens of all ureters of groups B and C were processed as follows: 900 mg of untreated or treated tissue (wet weight) were homogenized in 2 mL extraction solution A (50% CH3CN in water) at 4°C, and centrifuged at 12,000×g at the same temperature for 20 minutes. The pellet was extracted again with 2 mL extraction solution A and centrifuged again. The two supernatants were pooled, dried by SpeedVac evaporation, and used to determine PTX in the water-soluble fraction of the tissue extract. The remaining pellet was rinsed twice with 2 mL extraction solution A to remove any trace of water-soluble PTX. Then, it was homogenized twice in 2 mL of extraction solution B (75% CHCl3 in methanol) and centrifuged as described above. The obtained two supernatants were pooled, dried, and used to determine PTX in the lipid fraction of the tissue extract.
Before the NMR analysis, both dried extracts were dissolved in DMSO-d 6 and centrifuged at 12,000×g for 20 minutes. The supernatants were transferred to 5-mm NMR tubes. 1H 1D NMR spectra were recorded using identical experimental parameters with these applied for the NMR spectra of PTX. Spectra were recorded at 298K using a Bruker Avance III HD 700 MHz spectrometer equipped with a cryoprobe. 1H 1D NMR spectra were recorded using spectral width of 12 to 18 ppm, with suppression of the residual H2O signal using presaturation or excitation sculpting water suppression pulse sequences. 1H-13C heteronuclear spectra were recorded with a spectral width of 200 ppm at F1 dimension. Relaxation delay was set to 2 or 3 seconds. 1D data sets were acquired with 16k or 32k data points. For data processing and spectral analysis, the Topspin 3.2 and 3.3 versions (Bruker Corp, Coventry, UK) were used.
Pathology-IHC
One sample was obtained from each ureter of groups A, B, and C at the site of dilation. The pathologist evaluating the samples was blinded regarding the specimen groups.
Pathology
The histology specimens were fixed in formalin and underwent a standard embedding process with paraffin. The 4-μm–thick sections were stained with hematoxylin and eosin and mounted on gelatin-coated glass slides.
IHC
IHC with the use of polyclonal anti-PTX antibody aimed to elucidate the distribution of PTX in different layers of the ureter. IHC was performed on 4-μm–thick formalin-fixed, paraffin-embedded tissue sections mounted on gelatin-coated glass slides. The deparaffinization, rehydration, and antigen retrieval were performed in an electric pressure cooker using Trilogy retrieval solution (Cell Marque, Hot Springs, AR) for 30 minutes. For the primary antibody we used polyclonal antibody against Taxol (NBP1-05003, Novus Medical, Cambridge, UK) in a dilution of 1:3000. The sections were incubated with the primary antibody at room temperature for 1 hour, followed by a sequential 30-minute incubation with Dako EnVision Labelled Polymer (Dako North America Inc., Carpinteria, CA). Diaminobenzidine (Dako North America Inc.) was used as chromogen. Sections were counterstained with Harris hematoxylin (Vector, Burlingame, CA). In negative control slides, the same method was performed and the primary antibody was substituted by 1% TBS.
Evaluation of specimens
The slides were evaluated using a standard light microscope on which a camera was attached (Nikon ECLIPSE 50i and Nikon HD color camera head DS-Fi2, Nikon GmbH, Dűsseldorf, Germany). Three slides were obtained from each specimen for histology and three specimens for IHC. The presence of morphologic alterations and inflammation was evaluated in the case of histology. The inflammation of the ureteral wall was graded according to Nakada and associates. 33 Normal appearance in light microscopy of the ureteral wall was graded as 0 while severe inflammation was graded as 3. The presence of PTX and the location of the agent in the investigated slides were evaluated with IHC.
Results
Analysis
NMR
In accordance with the reference 1H spectrum of PTX, we were able to identify the well-resolved PTX proton resonance in 1H NMR (Table 1, Fig. 1). These spectra were obtained from ureteral tissue extract of specimens at 12 and 24 hours after the PEB dilation indicating the presence of the PTX proton resonances in these samples. The PTX resonances were not observed in any of the tissue extracts of specimens treated by CB. Although it is difficult to perform a quantitative analysis of the PTX concentration in the DMSO samples of the current tissue extracts, the signal-to-noise ratio along with the analysis of the relative proton resonances intensities (especially these for NH3' and some of the Phe1 and Phe3 PTX groups, Fig. 2), suggest that the concentration of PTX has been reduced in the samples of group C (Fig. 2C) compared with the amount of the PTX identified in the tissue extracts of group B (Fig. 2B).

Regions of the 1H 1D NMR spectra at 298K and 700MHz, of: (
1H & 13C chemical shifts (in ppm, 298K, DMSO-d 6, 700M Hz) of paclitaxel in dimethyl sulfoxide (DMSO).
Pathology
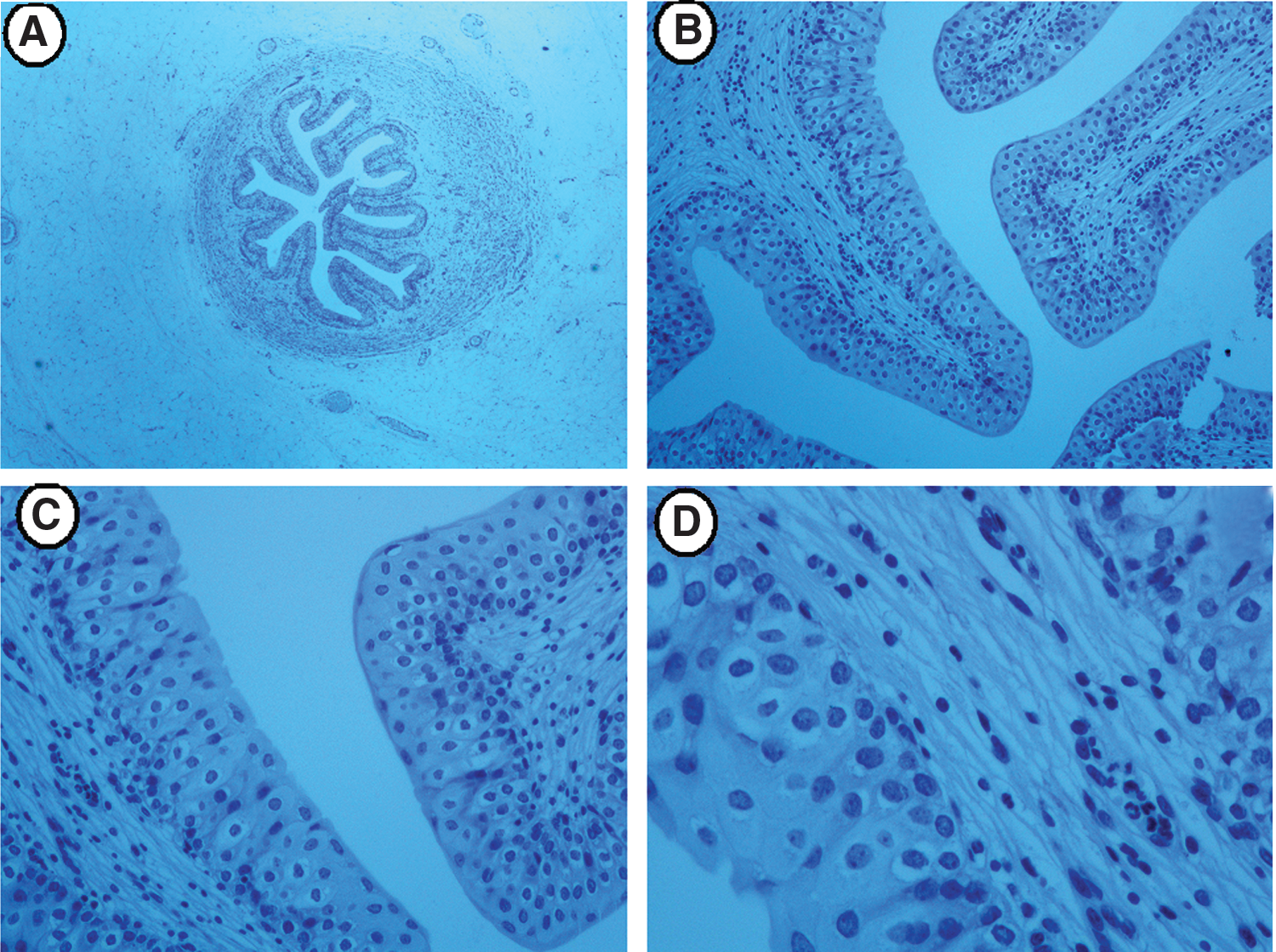
Seventy-two slides were evaluated (two slides from the control ureter and two from the DEB ureter). The dilation of the ureter by the use of a balloon had mechanical effects that were recognized in the pathologic evaluation (hematoxylin and eosin staining) because focal urothelium compression and rupture were present in all examined specimens regardless of the type of the balloon that was used for dilation (Table 2). Acute inflammation and granular tissue were present in all specimens of groups B and C. Specimens of group A hardly showed any inflammation. The inflammation was less in the case of group C specimens in comparison with group B when a PEB was used. On the contrary, the ureters treated by the CB had more inflammation in the case of group C in comparison with group B.
All alterations were focally observed. DEB, drug-eluting balloons.
IHC examination
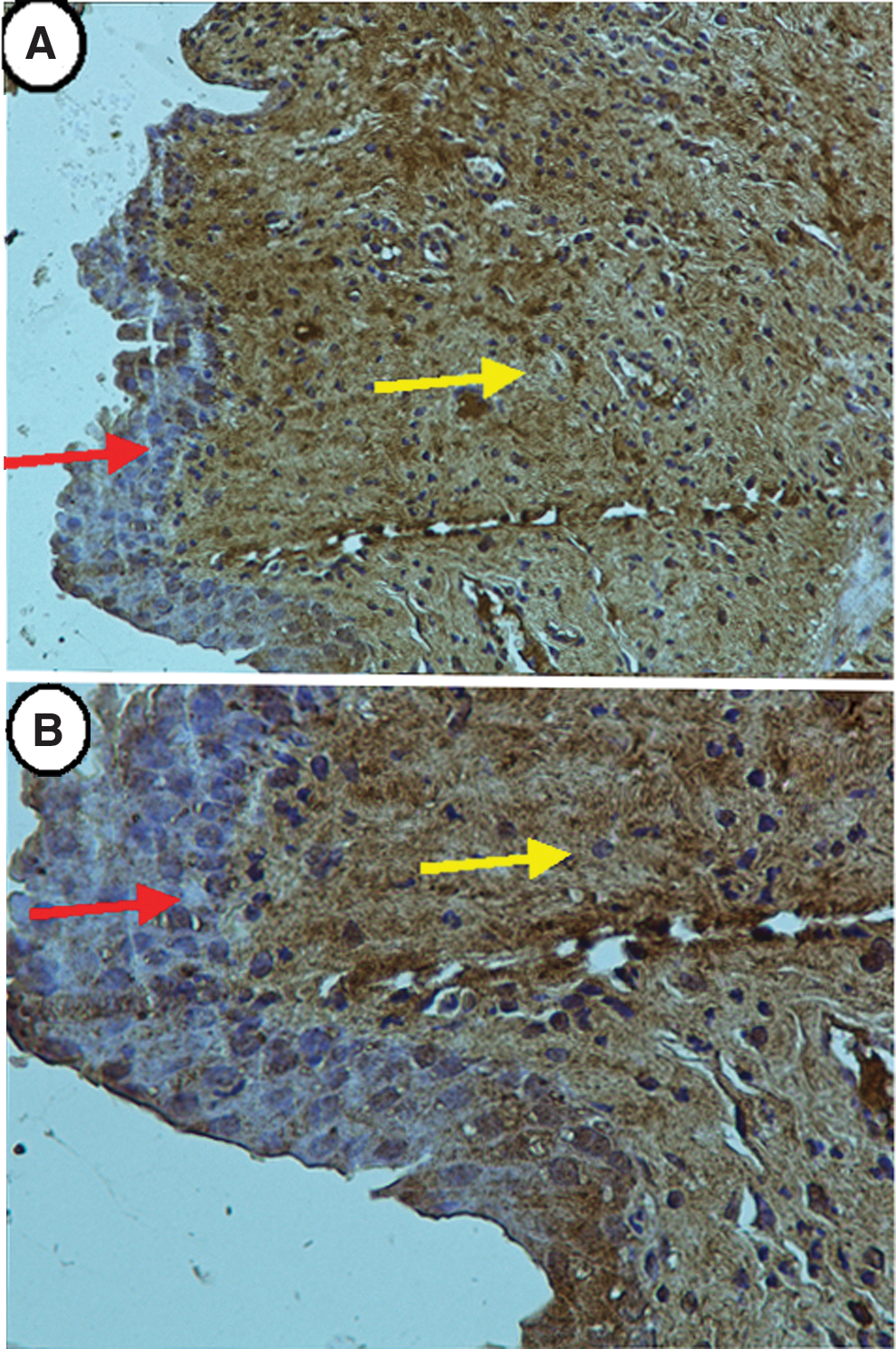
Thirty-three slides (27 slides from DEB dilated ureters and 6 slides of negative controls) were evaluated. PTX was distributed mostly in the urothelium and submucosal layer in group A. The agent was present in the submucosal and muscle layer in both groups B and C. The presence of PTX was more prominent in the case of group B. PTX was also present on the urothelium of groups B and C. Nevertheless, the presence of PTX on the urothelium of group A was more prominent compared with the other two groups. The result of the histologic alterations and the distribution of PTX are summarized in Table 2.
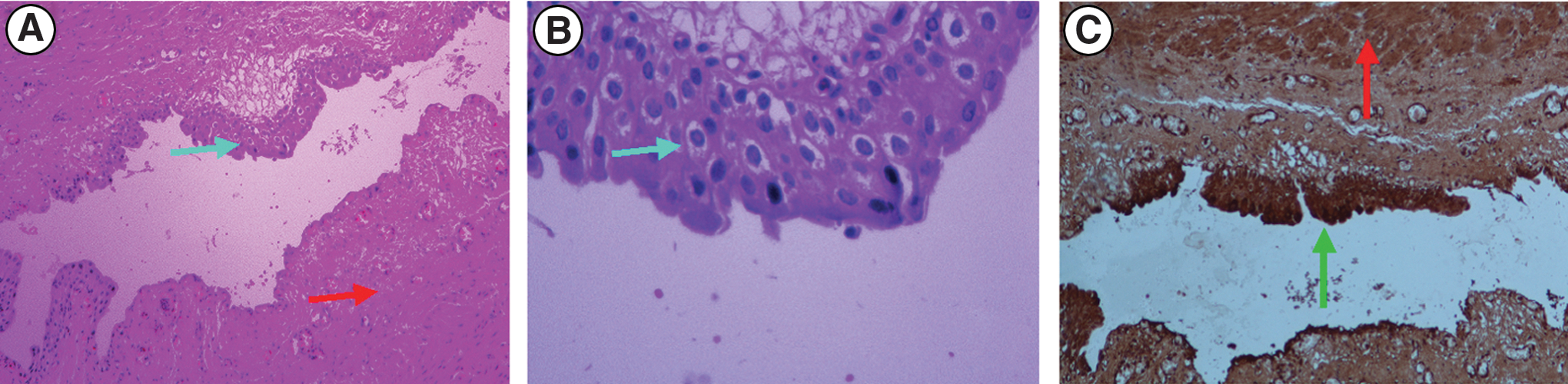
Figures 3 to 8 present histology and IHC images of ureters treated by PEB and CB from all groups of the study.

(

Ureter dilated by a drug-eluting balloon and immediate specimen removal (group A, t0). The green arrow (

(
(
(
Discussion
The current study aimed to answer questions regarding the penetration of PTX in the very impermeable barrier of the urothelium and to provide clues to the distribution of the agent in the layers of the ureteral wall as well as its effect on local inflammation. The penetration of the agent to the muscular layer should probably be considered as very important because of the aforementioned relation of the SMCs to the production of collagen and eventually stricture formation. 14
The selection of PTX was based on the known effect of the drug on the proliferation of the SMCs. 18 Nevertheless, the detection of PTX by means of IHC in the porcine ureter represented a significant challenge because the agent has never before been detected in the above setting. The NMR was used to detect PTX in the specimens and to confirm its presence in different periods. NMR also provided qualitative data on the concentration of PTX in the investigated tissue over the aforementioned periods. To our knowledge, the NMR has never before been used for the detection of PTX in porcine ureteral tissue.
The study showed that PTX was distributed deeper than the urothelial layer in the submucosal layer, reaching the muscular layer. PTX was present in the submucosal layer immediately after dilation, and this phenomenon should probably be attributed to the mechanical damage of the balloon to the ureteral wall. The presence of focal urothelial compression and rupture was practically uniform among the specimens. Nevertheless, rupture in the deeper layer was not evident probably because of the low diameter of the balloons. The selection of the balloon diameter was based on the fact that the diameter of the porcine ureter is 3 to 4 mm and is similar to the human ureter. 34 It was also important to avoid rupturing of the ureter, which would result in the dispersion of PTX to different layers or even outside of the lumen and probably provide misleading information.
Considering the lack of rupture of the deeper ureteral layers and the focal distribution of the damage, it could be advocated that the balloons did not result in significant mechanical damage of the ureter and the evident distribution of the substance was related to the characteristics of the drug rather than the mechanical effects of the balloons. Moreover, even in the case of the vascular use of DEB, the rupture of the vascular endothelium is important for the distribution of the drug and the distribution of PTX uses several different mechanisms, at least in the case of the vascular tissue. 35,36 Mechanical effects, from balloon dilation and probably from the other manipulations such as guidewire insertion, may be related to the induction of acute inflammation, which included all layers of the ureteral wall of groups B and C.
The PEB treated ureters had less acute inflammation in comparison with those treated by CB (Table 1). Furthermore, the increase of the inflammation grading in the CB treated ureters between 12 and 24 hours showed that the inflammation was progressing. The reduction of the inflammation in the PEB treated ureters during the same periods could be considered as a remission of the inflammation and probably should be attributed to the action of PTX.
PTX was detected in the muscle layers of the specimens of groups B and C. PTX was recognized only in one specimen of group A. Thus, the distribution of PTX probably should be related to a combination of mechanical rupture of the urothelium and diffusion of the substance because of its lipophilic nature. It has been reported in the literature that the initial binding of the drug in the endothelium of the vessels is very important for its further distribution. 37,38 This seems to also be the case for the use of DEB in the ureter. The drug was initially distributed on the urothelium and reached the deeper layers during the following hours. Another interesting finding was that PTX was more prominent in the submucosal and muscular layers of group B compared with group C. This finding, in conjunction with the presence of less inflammation in the case of group C in comparison with group B, probably dictates metabolism and action of PTX in the ureteral tissue.
The above observations were not based on specific quantitative evaluation of the IHC slides. Nonetheless, these observations were strengthened by the qualitative evaluation of the NMR spectra, which showed that the concentration of PTX was reduced in group C compared with group B. PTX was less prominent on the urothelial layers of groups B and C in comparison with group A in the IHC. This was probably related to the flushing of PTX by the urine. It should be noted that the current experiment represents the worst-case scenario because the ureteral wall did not undergo significant damage (rupture of the deeper ureteral layers) and the ureteral stretching compensated the balloon dilation. Thus, the aforementioned observations depict the distribution potential of PTX released from a DEB at least in the normal porcine ureter.
Limitation of the current study is the short period of investigation (24 hours). At the initiation of the experiment, even the penetration of the substance was questionable. Moreover, the investigators had a strong belief that the urine would probably flush the agent from the urothelium. The tissue levels of PTX applied by a DEB in porcine vessels reduce >80% in the first 24 hours, and the duration of the experiment probably should be considered as adequate. 39 In the light of the above evidence, a longer period of observation would have been interesting. A higher number of specimens would probably provide additional integrity to the study. Still, the uniformity of the results in each group, in addition to the double method of PTX tracing (NMR and IHC), sufficiently documents the conclusions of the study.
In addition, the methods of the current study were designed to provide descriptive evaluation of the presence of PTX in the ureteral tissue and not quantitative evaluation of PTX concentration. Thus, any conclusion regarding the differences in the concentration of PTX among the different study periods was based in the qualitative assessment by combining the results of NMR and IHC. Any precise quantitative data were not available.
The use of the porcine model is subject to the limitations of animal models, and the results of an experimental study in animals may not always be replicated in a clinical setting. Moreover, the current study does not evaluate the distribution and effect of PTX in the case of ureteral strictures, which is probably the most interesting potential clinical application of the DEBs.
Another limitation of the study is the use of DEBs designed for vascular application. The histology of arterial stenosis is different from ureteral stricture stenosis. The histology of the atherosclerotic lesions is associated with the natural history of the disease. 40 The histology of the atheromatous plaque has high diversity, and the treatment options are based on the classification of these plaques in vivo. The latter classification takes place by imaging techniques such as optical coherence tomography. 41 After treatment of vascular stenosis, the main cell implemented in the restenosis of vessels is the vascular SMC, which is activated because of the inflammation induced by the balloon dilation and related injury. 42 This inflammation and consequent restenosis process is inhibited with the drug distributed by the DEBs. On the other hand, the formation of the ureteral stricture is based on the action of the SMCs and the formation of connective tissue. The restenosis of the treated ureter is also the result of the SMCs and is related to the inflammation induced by the injury of the ureter. 10 –12,14
Considering the above findings, it seems that the mechanism related to the restenosis of the ureter has similarities to the vascular one, and the idea of using the DEBs is conceptually justified. The use of a material that is designed for vascular application is not an appropriate way to develop an effective therapeutic strategy. Nevertheless, its use for the experimental evaluation of the distribution of PTX through the impermeable urothelial barrier showed interesting results, and the objective of the current study was achieved. The distribution and effect of PTX delivered by a DEB in the porcine ureter was observed.
The aforementioned differences in the tissue composition and the mechanical properties (stretching potential) of the strictured ureters dictate the need for further investigation to draw conclusions on the distribution and effect of PTX in the case of ureteral strictures. Any possible clinical application of the vascular DEBs in the ureter should be considered in the context of significant differences among the histology of the ureter and the neointimal hyperplasia or atheromatous stenosis of the vessels as well as the need for significant experimental investigation of the mechanism of action and efficacy of DEBs in the ureter.
Conclusion
The distribution of PTX includes the urothelial, submucosal, and smooth muscle layers. Inflammation was less prominent in the case of DEB in comparison with the CB at 12 and 24 hours after the dilation of the ureters. The action of PTX should be considered responsible for the latter phenomenon.
Footnotes
Acknowledgment
“SEE-DRUG” Grant (EU FP7 REGPOT CT-2011-285950. Available at:
Disclosure Statement
No competing financial interests exist.